Why a common asthma drug will now carry extra safety warnings about depression
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australia’s Therapeutic Goods Administration (TGA) recently issued a safety alert requiring extra warnings to be included with the asthma and hay fever drug montelukast.
The warnings are for users and their families to look for signs of serious behaviour and mood-related changes, such as suicidal thoughts and depression. The new warnings need to be printed at the start of information leaflets given to both patients and health-care providers (sometimes called a “boxed” warning).
So why did the TGA issue this warning? And is there cause for concern if you or a family member uses montelukast? Here’s what you need to know.
First, what is montelukast?
Montelukast is a prescription drug also known by its brand names which include Asthakast, Lukafast, Montelair and Singulair. It’s used to manage the symptoms of mild-to-moderate asthma and seasonal hay fever in children and adults.
Asthma occurs when the airways tighten and produce extra mucus, which makes it difficult to get air into the lungs. Likewise, the runny nose characteristic of hay fever occurs due to the overproduction of mucus.
Leukotrienes are an important family of chemicals found throughout the airways and involved in both mucus production and airway constriction. Montelukast is a cysteinyl leukotriene receptor antagonist, meaning it blocks the site in the airways where the leukotrienes work.
Montelukast can’t be used to treat acute asthma (an asthma attack), as it takes time for the tablet to be broken down in the stomach and for it to be absorbed into the body. Rather, it’s taken daily to help prevent asthma symptoms or seasonal hay fever.
It can be used alongside asthma puffers that contain corticosteriods and drugs like salbutamol (Ventolin) in the event of acute attacks.
What is the link to depression and suicide?
The possibility that this drug may cause behavioural changes is not new information. Manufacturers knew this as early as 2007 and issued warnings for possible side-effects including depression, suicidality and anxiousness.
The United Kingdom’s Medicines and Healthcare products Regulatory Agency has required a warning since 2008 but mandated a more detailed warning in 2019. The United States’ Food and Drug Administration has required boxed warnings for the drug since 2020.

Montelukast is known to potentially induce a number of behaviour and mood changes, including agitation, anxiety, depression, irritability, obsessive-compulsive symptoms, and suicidal thoughts and actions.
Initially a 2009 study that analysed data from 157 clinical trials involving more than 20,000 patients concluded there were no completed suicides due to taking the drug, and only a rare risk of suicide thoughts or attempts.
The most recent study, published in November 2024, examined data from more than 100,000 children aged 3–17 with asthma or hay fever who either took montelukast or used only inhaled corticosteroids.
It found montelukast use was associated with a 32% higher incidence of behavioural changes. The behaviour change with the strongest association was sleep disturbance, but montelukast use was also linked to increases in anxiety and mood disorders.
In the past ten years, around 200 incidences of behavioural side-effects have been reported to the TGA in connection with montelukast. This includes 57 cases of depression, 60 cases of suicidal thoughts and 17 suicide attempts or incidents of intentional self-injury. There were seven cases where patients taking the drug did complete a suicide.
This is of course tragic. But these numbers need to be seen in the context of the number of people taking the drug. Over the same time period, more than 200,000 scripts for montelukast have been filled under the Pharmaceutical Benefits Scheme.
Overall, we don’t know conclusively that montelukast causes depression and suicide, just that it seems to increase the risk for some people.

And if it does change behaviour, we don’t fully understand how this happens. One hypothesis is that the drug and its breakdown products (or metabolites) affect brain chemistry.
Specifically, it might interfere with how the brain detoxifies the antioxidant glutathione or alter the regulation of other brain chemicals, such as neurotransmitters.
Why is the TGA making this change now?
The new risk warning requirement comes from a meeting of the Australian Advisory Committee on Medicines where they were asked to provide advice on ways to minimise the risk for the drug given current international recommendations.
Even though the 2024 review didn’t highlight any new risks, to align with international recommendations, and help address consumer concerns, the advisory committee recommended a boxed warning be added to drug information sheets.
If you have asthma and take montelukast (or your child does), you should not just stop taking the drug, because this could put you at risk of an attack that could be life threatening. If you’re concerned, speak to your doctor who can discuss the risks and benefits of the medication for you, and, if appropriate, prescribe a different medication.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14.
Nial Wheate, Professor of Pharmaceutical Chemistry, Macquarie University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cottage Cheese vs Ricotta – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cottage cheese to ricotta, we picked the ricotta.
Why?
Cottage cheese is a famous health food, mostly for being a low-fat, low-carb, source of protein. And yet, ricotta beats it in most respects.
Looking at the macros first, cottage cheese has more carbs, while ricotta has more protein and fat. The fat profile is pretty much the same, and in both cases it’s two thirds saturated fat, which isn’t good in either case, but cottage cheese has less overall fat which means less saturated fat in total even if the percentage is the same. Because the difference in carbs and protein is not large, while ricotta has considerably more fat, we’ll call this category a win for cottage cheese.
In terms of vitamins, cottage cheese has more of vitamins B1, B5, and B12, while ricotta has more of vitamins A, B2, B3, B9, D, E, and K, so this one’s a win for ricotta.
In the category of minerals, cottage cheese has slightly more copper, while ricotta has much more calcium, iron, magnesium, manganese, potassium, selenium, and zinc. In particular, 2.5x more calcium, and 5x more iron! An easy and clear win for ricotta here.
Taking everything into account: yes, cottage cheese has less fat (and thus, in total, less saturated fat, although the percentage is the same), but that doesn’t make up for ricotta winning in pretty much every other respect. Still, enjoy either or both (in moderation!) if you be so inclined.
Want to learn more?
You might like to read:
Take care!
Share This Post
-
Neurologists Debunk 11 Brain Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Neuroscientists Dr. Santoshi Billakota and Dr. Brad Kamitaki debunk 11 myths about the brain. How many did you know?
From the top
Without further ado, the myths are…
- “We only use 10% of our brains”: False! We use most parts of our brain at different times, depending on the activity. PET/MRI scans show widespread usage.
- “The bigger the brain, the smarter the creature”: False! While there’s often a correlation, intelligence depends on brain complexity and development of specific regions, not overall size. For this reason get, for example, some corvids that are more intelligent than some dogs.
- “IQ tests are an accurate measure of intelligence”: False! IQ tests measure limited aspects of intelligence and are influenced by external factors like test conditions and education.
- “Video games rot your brain”: False! Video games can improve problem-solving, strategy, and team-building skills when played in moderation.
- “Memory gets worse as you age”: Partly false. While episodic memory may decline, semantic and procedural memory often improve with age.
- “Left-brained people are logical, and right-brained people are creative”: False! Both hemispheres work together, and personality or skills are influenced by environment and experiences, not brain hemispheres.
- “You can’t prevent a stroke”: False! Strokes can often be prevented by managing risk factors like blood pressure, cholesterol, and lifestyle choices.
- “Eating fish makes you smarter”: False! Eating fish, especially those rich in omega-3s, can support brain health but won’t increase intelligence.
- “You can always trust your senses”: False! Senses can be deceptive and influenced by emotions, memories, or neurological conditions.
- “Different sexes have different brains”: False! Structurally, brains are the same regardless of chromosomal sex; differences arise from environmental (including hormonal) and experiential factors—and even there, there’s more than enough overlap that we are far from categorizable as sexually dimorphic.
- “If you have a seizure, you have epilepsy”: False! A seizure can occur from various causes, but epilepsy is defined by recurrent unprovoked seizures and requires specific diagnosis and treatment.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The Dopamine Myth ← a bonus 12th myth!
Take care!
Share This Post
-
Why You Can’t Just “Get Over” Trauma
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Time does not, in fact, heal all wounds. Sometimes they even compound themselves over time. Dr. Tracey Marks explains the damage that trauma does—the physiological presentation of “the axe forgets but the tree remembers”—and how to heal from that actual damage.
The science of healing
Trauma affects the mind and body (largely because the brain is, of course, both—and affects pretty much everything else), which can ripple out into all areas of life.
On the physical level, brain areas affected by trauma include:
- Amygdalae: becomes hyperactive, keeping a person in a heightened state of vigilance.
- Hippocampi: can shrink, causing fragmented or missing memories.
- Prefrontal cortex: reduces in activity, impairing decision-making and emotional regulation.
Trauma also activates the body’s fight or flight response, releasing stress hormones like cortisol and adrenaline. These are great things to have a pinch, but having them elevated all the time is equivalent to only ever driving your car at top speed—the only question becomes whether you’ll crash and burn before you break down.
However, there is hope! Neuroplasticity (the brain’s ability to rewire itself) can make trauma recovery possible through various interventions.
Evidence-based therapies for trauma include:
- Eye Movement Desensitization and Reprocessing (EMDR): this can help reprocess traumatic memories and reduce emotional intensity.
- Trauma-focused Cognitive Behavioral Therapy (CBT): this can help change unhelpful thought patterns and includes exposure therapy.
- Somatic therapies: these focus on the body and nervous system to release stored tension.
In this latter category, embodiment is key to trauma recovery—this may sound “wishy-washy”, but the evidence shows that reconnecting with the body does help manage emotional stress responses. Mind-body practices like mindfulness, yoga, and breathwork help cultivate embodiment and reduce trauma-related stress.
In short: you can’t just “get over” it, but with the right support and interventions, it’s possible to rewire the brain and body toward resilience and healing.
For more on all of this from Dr. Marks, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- PTSD, But, Well…. Complex.
- Undoing The Damage Of Life’s Hard Knocks
- A Surprisingly Powerful Tool: Eye Movement Desensitization & Reprocessing
Take care!
Share This Post
Related Posts
-

How does cancer spread to other parts of the body?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
All cancers begin in a single organ or tissue, such as the lungs or skin. When these cancers are confined in their original organ or tissue, they are generally more treatable.
But a cancer that spreads is much more dangerous, as the organs it spreads to may be vital organs. A skin cancer, for example, might spread to the brain.
This new growth makes the cancer much more challenging to treat, as it can be difficult to find all the new tumours. If a cancer can invade different organs or tissues, it can quickly become lethal.
When cancer spreads in this way, it’s called metastasis. Metastasis is responsible for the majority (67%) of cancer deaths.
Cells are supposed to stick to surrounding tissue
Our bodies are made up of trillions of tiny cells. To keep us healthy, our bodies are constantly replacing old or damaged cells.
Each cell has a specific job and a set of instructions (DNA) that tells it what to do. However, sometimes DNA can get damaged.
This damage might change the instructions. A cell might now multiply uncontrollably, or lose a property known as adherence. This refers to how sticky a cell is, and how well it can cling to other surrounding cells and stay where it’s supposed to be.
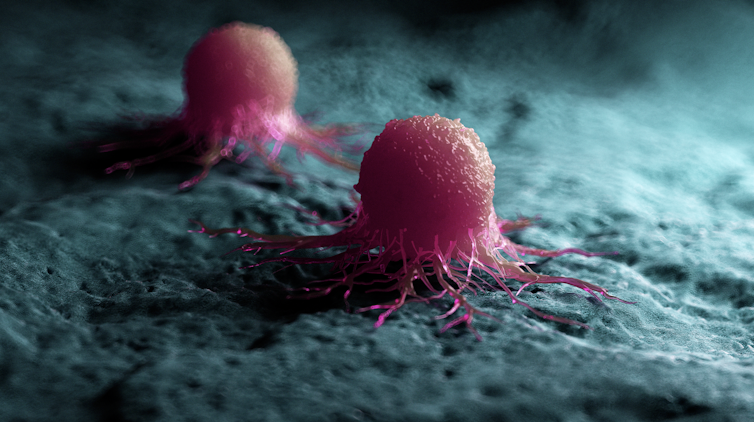
If a cancer cell loses its adherence, it can break off from the original tumour and travel through the bloodstream or lymphatic system to almost anywhere. This is how metastasis happens.
Many of these travelling cancer cells will die, but some will settle in a new location and begin to form new cancers.

Some cells settle in a new location.
Scipro/ShutterstockParticular cancers are more likely to metastasise to particular organs that help support their growth. Breast cancers commonly metastasise to the bones, liver, and lungs, while skin cancers like melanomas are more likely to end up in the brain and heart.
Unlike cancers which form in solid organs or tissues, blood cancers like leukaemia already move freely through the bloodstream, but can escape to settle in other organs like the liver or brain.
When do cancers metastasise?
The longer a cancer grows, the more likely it is to metastasise. If not caught early, a patient’s cancer may have metastasised even before it’s initially diagnosed.
Metastasis can also occur after cancer treatment. This happens when cancer cells are dormant during treatment – drugs may not “see” those cells. These invisible cells can remain hidden in the body, only to wake up and begin growing into a new cancer months or even years later.
For patients who already have cancer metastases at diagnosis, identifying the location of the original tumour – called the “primary site” – is important. A cancer that began in the breast but has spread to the liver will probably still behave like a breast cancer, and so will respond best to an anti-breast cancer therapy, and not anti-liver cancer therapy.
As metastases can sometimes grow faster than the original tumour, it’s not always easy to tell which tumour came first. These cancers are called “cancers of unknown primary” and are the 11th most commonly diagnosed cancers in Australia.
One way to improve the treatment of metastatic cancer is to improve our ways of detecting and identifying cancers, to ensure patients receive the most effective drugs for their cancer type.
What increases the chances of metastasis and how can it be prevented?
If left untreated, most cancers will eventually acquire the ability to metastasise.
While there are currently no interventions that specifically prevent metastasis, cancer patients who have their tumours surgically removed may also be given chemotherapy (or other drugs) to try and weed out any hidden cancer cells still floating around.
The best way to prevent metastasis is to diagnose and treat cancers early. Cancer screening initiatives such as Australia’s cervical, bowel, and breast cancer screening programs are excellent ways to detect cancers early and reduce the chances of metastasis.
The best way to prevent cancer spreading is to diagnose and treat them early.
Peakstock/ShutterstockNew screening programs to detect cancers early are being researched for many types of cancer. Some of these are simple: CT scans of the body to look for any potential tumours, such as in England’s new lung cancer screening program.
Using artificial intelligence (AI) to help examine patient scans is also possible, which might identify new patterns that suggest a cancer is present, and improve cancer detection from these programs.
More advanced screening methods are also in development. The United States government’s Cancer Moonshot program is currently funding research into blood tests that could detect many types of cancer at early stages.
One day there might even be a RAT-type test for cancer, like there is for COVID.
Will we be able to prevent metastasis in the future?
Understanding how metastasis occurs allows us to figure out new ways to prevent it. One idea is to target dormant cancer cells and prevent them from waking up.
Directly preventing metastasis with drugs is not yet possible. But there is hope that as research efforts continue to improve cancer therapies, they will also be more effective at treating metastatic cancers.
For now, early detection is the best way to ensure a patient can beat their cancer.

Sarah Diepstraten, Senior Research Officer, Blood Cells and Blood Cancer Division, Walter and Eliza Hall Institute and John (Eddie) La Marca, Senior Resarch Officer, Walter and Eliza Hall Institute
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The “Yes I Can” Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes, we are given to ask ourselves: “Can I produce a healthy and tasty salad out of what I have in?” and today we show how, with a well-stocked pantry, the answer is “yes I can”, regardless of what is (or isn’t) in the fridge.
You will need
- 1 can cannellini beans, drained
- 1 can sardines (if vegetarian/vegan, substitute ½ can chickpeas, drained)
- 1 can mandarin segments
- 1 handful pitted black olives, from a jar (or from a can, if you want to keep the “yes I can” theme going)
- ½ red onion, thinly sliced (this can be from frozen, defrosted—sliced/chopped onion is always a good thing to have in your freezer, by the way; your writer here always has 1–6 lbs of chopped onions in hers, divided into 1lb bags)
- 1 oz lemon juice
- 1 tbsp chopped parsley (this can be freeze-dried, but fresh is good if you have it)
- 1 tbsp extra virgin olive oil
- 1 tbsp chia seeds
- 1 tsp miso paste
- 1 tsp honey (omit if you don’t care for sweetness; substitute with agave nectar if you do like sweetness but don’t want to use honey specifically)
- 1 tsp red chili flakes
Method
(we suggest you read everything at least once before doing anything)
1) Combine the onion and the lemon juice in a small bowl, massaging gently
2) Mix (in another bowl) the miso paste with the chili flakes, chia seeds, honey, olive oil, and the spare juice from the can of mandarin segments, and whisk it to make a dressing.
3) Add the cannellini beans, sardines (break them into bite-size chunks), mandarin segments, olives, and parsley, tossing them thoroughly (but gently) in the dressing.
4) Top with the sliced onion, discarding the excess lemon juice, and serve:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Three Daily Servings of Beans?
- We Are Such Stuff As Fish Are Made Of
- Chia: The Tiniest Seeds With The Most Value
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Avoiding/Managing Osteoarthritis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Avoiding/Managing Osteoarthritis
Arthritis is the umbrella term for a cluster of joint diseases involving inflammation of the joints, hence “arthr-” (joint) “-itis” (suffix used to denote inflammation).
Inflammatory vs Non-Inflammatory Arthritis
Arthritis is broadly divided into inflammatory arthritis and non-inflammatory arthritis.
Some forms, such as rheumatoid arthritis, are of the inflammatory kind. We wrote about that previously:
See: Avoiding/Managing Rheumatoid Arthritis
You may be wondering: how does one get non-inflammatory inflammation of the joints?
The answer is, in “non-inflammatory” arthritis, such as osteoarthritis, the damage comes first (by general wear-and-tear) and inflammation generally follows as part of the symptoms, rather than the cause.
So the name can be a little confusing. In the case of osteo- and other “non-inflammatory” forms of arthritis, you definitely still want to keep your inflammation at bay as best you can; it’s just not the prime focus.
So, what should we focus on?
First and foremost: avoiding wear-and-tear if possible. Naturally, we all must live our lives, and sometimes that means taking a few knocks, and definitely it means using our joints. An unused joint would suffer just as much as an abused one. But, we can take care of our joints!
We wrote on that previously, too:
See: How To Really Look After Your Joints
New osteoarthritis medication (hot off the press!)
At 10almonds, we try to keep on top of new developments, and here’s a shiny new one from this month:
- Methotrexate to treat hand osteoarthritis with synovitis (12th Oct, clinical trial)
- New research has found an existing drug could help many people with painful hand osteoarthritis (24th Oct, pop-science article about the above, but still written by one of the study authors!)
Note also that Dr. Flavia Cicuttini there talks about what we talked about above—that calling it non-inflammatory arthritis is a little misleading, as the inflammation still occurs.
And finally…
You might consider other lifestyle adjustments to manage your symptoms. These include:
- Exercise—gently, though!
- Rest—while keeping mobility going.
- Mobility aids—if it helps, it helps.
- Go easy on the use of braces, splints, etc—these can offer short-term relief, but at a long term cost of loss of mobility.
- Only you can decide where to draw the line when it comes to that trade-off.
You can also check out our previous article:
See: Managing Chronic Pain (Realistically!)
Take good care of yourself!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: