Syringe Exchange Fears Hobble Fight Against West Virginia HIV Outbreak
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
CHARLESTON, http://w.va/. — More than three years have passed since federal health officials arrived in central Appalachia to assess an alarming outbreak of HIV spread mostly between people who inject opioids or methamphetamine.
Infectious disease experts from the Centers for Disease Control and Prevention made a list of recommendations following their visit, including one to launch syringe service programs to stop the spread at its source. But those who’ve spent years striving to protect people who use drugs from overdose and illness say the situation likely hasn’t improved, in part because of politicians who contend that such programs encourage illegal drug use.
Joe Solomon is a Charleston City Council member and co-director of SOAR WV, a group that works to address the health needs of people who use drugs. He’s proud of how his close-knit community has risen to this challenge but frustrated with the restraints on its efforts.
“You see a city and a county willing to get to work at a scale that’s bigger than ever before,” Solomon said, “but we still have one hand tied behind our back.”
The hand he references is easier access to clean syringes.
In April 2021, the CDC came to Charleston — the seat of Kanawha County and the state capital, tucked into the confluence of the Kanawha and Elk rivers — to investigate dozens of newly detected HIV infections. The CDC’s HIV intervention chief called it “the most concerning HIV outbreak in the United States” and warned that the number of reported diagnoses could be just “the tip of the iceberg.”
Now, despite attention and resources directed toward the outbreak, researchers and health workers say HIV continues to spread. In large part, they say, the outbreak lingers because of restrictions state and local policymakers have placed on syringe exchange efforts.
Research indicates that syringe service programs are associated with an estimated 50% reduction in HIV and hepatitis C, and the CDC issued recommendations to steer a response to the outbreak that emphasized the need for improved access to those services.
That advice has thus far gone unheeded by local officials.
In late 2015, the Kanawha-Charleston Health Department launched a syringe service program but shuttered it in 2018 under pressure, with then-Mayor Danny Jones calling it a “mini-mall for junkies and drug dealers.”
SOAR stepped in, hosting health fairs at which it distributed naloxone, an opioid overdose reversal drug; offered treatment and referrals; provided HIV testing; and exchanged clean syringes for used ones.
But in April 2021, the state legislature passed a bill limiting the number of syringes people could exchange and made it mandatory to present a West Virginia ID. The Charleston City Council subsequently added guidelines of its own, including requiring individual labeling of syringes.
As a result of these restrictions, SOAR ceased exchanging syringes. West Virginia Health Right now operates an exchange program in the city under the restrictions.
Robin Pollini is a West Virginia University epidemiologist who conducts community-based research on injection drug use. “Anyone I’ve talked to who’s used that program only used it once,” she said. “And the numbers they report to the state bear that out.”
A syringe exchange run by the health department in nearby Cabell County — home to Huntington, the state’s largest city after Charleston — isn’t so constrained. As Solomon notes, that program exchanges more than 200 syringes for every one exchanged in Kanawha.
A common complaint about syringe programs is that they result in discarded syringes in public spaces. Jan Rader, director of Huntington’s Mayor’s Office of Public Health and Drug Control Policy, is regularly out on the streets and said she seldom encounters discarded syringes, pointing out that it’s necessary to exchange a used syringe for a new one.
In August 2023, the Charleston City Council voted down a proposal from the Women’s Health Center of West Virginia to operate a syringe exchange in the city’s West Side community, with opponents expressing fears of an increase in drug use and crime.
Pollini said it’s difficult to estimate the number of people in West Virginia with HIV because there’s no coordinated strategy for testing; all efforts are localized.
“You would think that in a state that had the worst HIV outbreak in the country,” she said, “by this time we would have a statewide testing strategy.”
In addition to the testing SOAR conducted in 2021 at its health fairs, there was extensive testing during the CDC’s investigation. Since then, the reported number of HIV cases in Kanawha County has dropped, Pollini said, but it’s difficult to know if that’s the result of getting the problem under control or the result of limited testing in high-risk groups.
“My inclination is the latter,” she said, “because never in history has there been an outbreak of injection-related HIV among people who use drugs that was solved without expanding syringe services programs.”
“If you go out and look for infections,” Pollini said, “you will find them.”
Solomon and Pollini praised the ongoing outreach efforts — through riverside encampments, in abandoned houses, down county roads — of the Ryan White HIV/AIDS Program to test those at highest risk: people known to be injecting drugs.
“It’s miracle-level work,” Solomon said.
But Christine Teague, Ryan White Program director at the Charleston Area Medical Center, acknowledged it hasn’t been enough. In addition to HIV, her concerns include the high incidence of hepatitis C and endocarditis, a life-threatening inflammation of the lining of the heart’s chambers and valves, and the cost of hospital resources needed to address them.
“We’ve presented that data to the legislature,” she said, “that it’s not just HIV, it’s all these other lengthy hospital admissions that, essentially, Medicaid is paying for. And nothing seems to penetrate.”
Frank Annie is a researcher at CAMC specializing in cardiovascular diseases, a member of the Charleston City Council, and a proponent of syringe service programs. Research he co-authored found 462 cases of endocarditis in southern West Virginia associated with injection drug use, at a cost to federal, state, and private insurers of more than $17 million, of which less than $4 million was recovered.
Teague is further concerned for West Virginia’s rural counties, most of which don’t have a syringe service program.
Tasha Withrow, a harm reduction advocate in bordering rural Putnam County, said her sense is that HIV numbers aren’t alarmingly high there but said that, with little testing and heightened stigma in a rural community, it’s difficult to know.
In a January 2022 follow-up report, the CDC recommended increasing access to harm reduction services such as syringe service programs through expansion of mobile services, street outreach, and telehealth, using “patient-trusted” individuals, to improve the delivery of essential services to people who use drugs.
Teague would like every rural county to have a mobile unit, like the one operated by her organization, offering harm reduction supplies, medication, behavioral health care, counseling, referrals, and more. That’s an expensive undertaking. She suggested opioid settlement money through the West Virginia First Foundation could pay for it.
Pollini said she hopes state and local officials allow the experts to do their jobs.
“I would like to see them allow us to follow the science and operate these programs the way they’re supposed to be run, and in a broader geography,” she said. “Which means that it shouldn’t be a political decision; it should be a public health decision.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Savoy Cabbage vs Pak Choi – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing savoy cabbage to pak choi, we picked the savoy.
Why?
Looking at the macros first, the savoy has a little more protein, just under 3x the carbs, and just over 3x the fiber. A modest yet respectable win for savoy.
In terms of vitamins, savoy has more of vitamins B1, B5, B9, E, K, and choline, while pak choi has more of vitamins A, B2, B3, and C. Thus, a 6:4 win for savoy.
When it comes to minerals, savoy has more copper, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while pak choi has more calcium, iron, and potassium. So this time, a 7:3 win for savoy.
On the other hand, pak choi scores higher on the polyphenols side, especially in the categories of kaempferol and quercetin.
Still, adding up the sections, we conclude this one’s an overall win for savoy cabbage. Of course, enjoy either or both, though!
Want to learn more?
You might like to read:
Fight Inflammation & Protect Your Brain, With Quercetin
Take care!
Share This Post
-
12 Foods That Fight Depression & Anxiety
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Food impacts mental health, and while it won’t magically cure mental illness, dietary changes can do a lot to improve mood. Here’s how:
Nutraceuticals
We’ll not keep the 12 nutraceutical foods a mystery; here’s what they are and a few words on how they work (in many cases, we could write whole articles about them; in some cases, we already have! You can find many of them by using the search function in the top-right of each page).
- Walnuts are rich in omega-3s for brain health; arguably the best nut for depression relief.
- Fermented foods because probiotics in foods like yogurt and sauerkraut support the gut-brain connection as well as serotonin production there, enhancing mood.
- Cherry tomatoes are rich in lycopene, which helps combat both depression and mood swings.
- Leafy greens reduce brain inflammation linked to depression.
- Apples and other fruit are high in fiber and antioxidants that stabilize blood sugar and mood, reducing brain inflammation.
- Beans are high in B vitamins, crucial for neurotransmitter production and mood regulation (without also being high in brain-harmful things, as red meat is).
- Berries are super-high antioxidants and cortisol-lowering anthocyanidins, promoting calmness and reducing stress.
- Oats contain the healthiest kind of fiber, β-glucan, and additionally help stabilize blood sugar and mood; they’re also rich in selenium, which boosts mood.
- Mushrooms help regulate blood sugar and act as prebiotics, supporting serotonin production in the gut.
- Avocados are famously rich in healthy fats, including omega-3s and oleic acid, which support brain health and combat depression.
- Dark chocolate contains antioxidants, magnesium, and gut-healthy prebiotics that indirectly reduce mental stress and improve brain function. Also a famous comfort food for many, of course, and that factor’s not to be overlooked either.
- Pumpkin seeds are rich in tryptophan, which boosts serotonin production. As a bonus, they also help some kinds of antidepressant to work better—check with your doctor or pharmacist to be sure in your case, though.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The 6 Pillars Of Nutritional Psychiatry
Take care!
Share This Post
-

Eat to Your Heart’s Content – by Dr. Sat Bains
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Making food heart-healthy and tasty is a challenge that vexes many, but it doesn’t have to be so difficult.
Dr. Sat Bains, a professional chef with multiple Michelin stars to his name, is an expert on “tasty”, and after surviving a heart attack himself, he’s become an expert on “heart-healthy” since then.
The book contains not only the recipes (of which there are 68, by the way), but also large sections of explanation of what makes various ingredients or methods heart-healthy or heart-unhealthy.
There’s science in there too, and these sections were written under the guidance of Dr. Neil Williams, a lecturer in physiology and nutrition.
You may be wondering as to why the author himself has a doctorate too; in fact he has three, none of which are relevant:
- Doctor of Arts
- Doctor of Laws
- Doctor of Hospitality (Honorary)
…but we prefix “Dr.” when people are that and he is that. The expertise we’re getting here though is really his culinary skill and extracurricular heart-healthy learning, plus Dr. Williams’ actual professional health guidance.
Bottom line: if you’d like heart-healthy recipes with restaurant-level glamour, this book is a fine choice.
Click here to check out Eat To Your Heart’s Content, and look after yours!
Share This Post
-

Migraine Mythbusting
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine: When Headaches Are The Tip Of The Neurological Iceberg

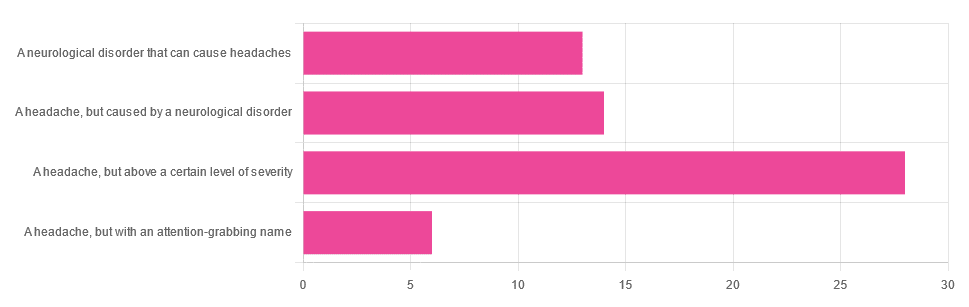
Yesterday, we asked you “What is a migraine?” and got the above-depicted, below-described spread of responses:
- Just under 46% said “a headache, but above a certain level of severity”
- Just under 23% said “a headache, but caused by a neurological disorder”
- Just over 21% said “a neurological disorder that can cause headaches”
- Just under 10% said “a headache, but with an attention-grabbing name”
So… What does the science say?
A migraine is a headache, but above a certain level of severity: True or False?
While that’s usually a very noticeable part of it… That’s only one part of it, and not a required diagnostic criterion. So, in terms of defining what a migraine is, False.
Indeed, migraine may occur without any headache, let alone a severe one, for example: Abdominal Migraine—though this is much less well-researched than the more common with-headache varieties.
Here are the defining characteristics of a migraine, with the handy mnemonic 5-4-3-2-1:
- 5 or more attacks
- 4 hours to 3 days in duration
- 2 or more of the following:
- Unilateral (affects only one side of the head)
- Pulsating
- Moderate or severe pain intensity
- Worsened by or causing avoidance of routine physical activity
- 1 or more of the following:
- Nausea and/or vomiting
- Sensitivity to both light and sound
Source: Cephalalgia | ICHD-II Classification: Parts 1–3: Primary, Secondary and Other
As one of our subscribers wrote:
❝I have chronic migraine, and it is NOT fun. It takes away from my enjoyment of family activities, time with friends, and even enjoying alone time. Anyone who says a migraine is just a bad headache has not had to deal with vertigo, nausea, loss of balance, photophobia, light sensitivity, or a host of other symptoms.❞
Migraine is a neurological disorder: True or False?
True! While the underlying causes aren’t known, what is known is that there are genetic and neurological factors at play.
❝Migraine is a recurrent, disabling neurological disorder. The World Health Organization ranks migraine as the most prevalent, disabling, long-term neurological condition when taking into account years lost due to disability.
Considerable progress has been made in elucidating the pathophysiological mechanisms of migraine, associated genetic factors that may influence susceptibility to the disease❞
Source: JHP | Mechanisms of migraine as a chronic evolutive condition
Migraine is just a headache with a more attention-grabbing name: True or False?
Clearly, False.
As we’ve already covered why above, we’ll just close today with a nod to an old joke amongst people with chronic illnesses in general:
“Are you just saying that because you want attention?”
“Yes… Medical attention!”
Want to learn more?
You can find a lot of resources at…
NIH | National Institute of Neurological Disorders & Stroke | Migraine
and…
The Migraine Trust ← helpfully, this one has a “Calm mode” to tone down the colorscheme of the website!
Particularly useful from the above site are its pages:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Felt Time – by Dr. Marc Wittmann
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book goes far beyond the obvious “time flies when you’re having fun / passes slowly when bored”, or “time seems quicker as we get older”. It does address those topics too, but even in doing so, unravels deeper intricacies within.
The author, a research psychologist, includes plenty of reference to actual hard science here, and even beyond subjective self-reports. For example, you know how time seems to slow down upon immediate apparent threat of violent death (e.g. while crashing, while falling, or other more “violent human” options)? We learn of an experiment conducted in an amusement park, where during a fear-inducing (but actually safe) plummet, subjective time slows down yes, but measures of objective perception and cognition remained the same. So much for adrenal superpowers when it comes to the brain!
We also learn about what we can change, to change our perception of time—in either direction, which is a neat collection of tricks to know.
The style is on the dryer end of pop-sci; we suspect that being translated from German didn’t help its levity. That said, it’s not scientifically dense either (i.e. not a lot of jargon), though it does have many references (which we like to see).
Bottom line: if you’ve ever wished time could go more quickly or more slowly, this book can help with that.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Longans vs Lychees – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing longans to lychees, we picked the lychees.
Why?
These two fruits are more closely related than they look from the outside, both being members of the soapberry family. However, there are some differences:
In terms of macros, longans have more protein while lychees have more carbs, and they are equal on fiber, giving longans the lower glycemic index. They’re both good, but longans nominally take the win on this one.
When it comes to vitamins, longans have more of vitamins B1, B2, and C, while lychees have more of vitamins B3, B6, B9, E, K, and choline, making for a respectable win for lychees in this category.
In the category of minerals, longans have more copper and potassium, while lychees have more calcium, iron, manganese phosphorus, and zinc. Thus, a win for lychees here too.
It’s worth looking at polyphenols too—lychees have around 10x more, which is notable.
Adding up the categories makes for an overall win for lychees, but by all means enjoy either or both! Diversity is good.
Want to learn more?
You might like to read:
Replacing Sugar: Top 10 Anti-Inflammatory Sweet Foods ← longans and lychees both make the list
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: