Are Waist Trainers Just A Waste, And Are Posture Fixers A Quick Fix?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Are Waist Trainers Just A Waste, And Are Posture Fixers A Quick Fix?
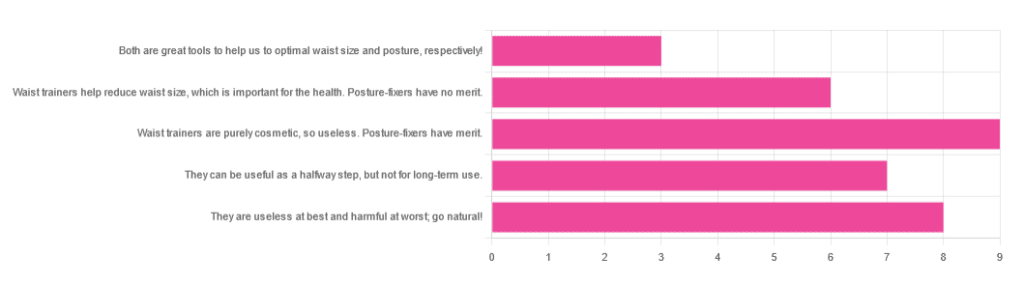
Yesterday, we asked you for your opinions on waist trainers and posture-fixing harnesses, and got the above-depicted, below-described set of results:
- The most popular response was “Waist trainers are purely cosmetic, so useless. Posture-fixers have merit”, with a little over a quarter of the votes.
- The least popular response was “Both are great tools to help us to optimal waist size and posture, respectively!”
- The other three answers each got a little under a quarter of the vote. In terms of discrete data, these were all 7±1, so basically, there was nothing in it.
The sample size was smaller than usual—perhaps the cluster of American holiday dates yesterday and today kept people busy! But, pressing on…
What does the science say?
Waist trainers are purely cosmetic, so, useless. True or False?
True, simply. Honestly, they’re not even that great for cosmetic purposes. They will indeed cinch in your middle, and this shape will be retained for a (very) short while after uncinching, because your organs have been squished inwards and may take a short while to get back to where they are supposed to be.
The American Board of Cosmetic Surgery may not be an unbiased source, but we’re struggling to find scientists who will even touch one of these, so, let’s see what these doctors have to say:
- Waist training can damage vital organs
- You will be slowly suffocating yourself
- Waist training simply doesn’t work
- You cannot drastically change your body shape with a piece of fabric*
Read: ABCS | 4 Reasons to Throw Your Waist Trainer in the Trash
*”But what about foot-binding?”—feet have many bones, whose growth can be physically restricted. Your waist has:
- organs: necessary! (long-term damage possible, but they’re not going away)
- muscles: slightly restrictable! (temporary restriction; no permanent change)
- fat: very squeezable! (temporary muffin; no permanent change)
Posture correctors have merit: True or False?
True—probably, and as a stepping-stone measure only.
The Ergonomics Health Association (a workplace health & safety organization) says:
❝Looking at the clinical evidence of posture correctors, we can say without a doubt that they do work, just not for everyone and not in the same way for all patients.❞
Source: Do Posture Correctors Work? Here’s What Our Experts Think
That’s not very compelling, so we looked for studies, and found… Not much, actually. However, what we did find supported the idea that “they probably do help, but we seriously need better studies with less bias”:
That is also not a compelling title, but here is where it pays to look at the studies and not just the titles. Basically, they found that the results were favorable to the posture-correctors—the science itself was just trash:
❝ The overall findings were that posture-correcting shirts change posture and subjectively have a positive effect on discomfort, energy levels and productivity.
The quality of the included literature was poor to fair with only one study being of good quality. The risk of bias was serious or critical for the included studies. Overall, this resulted in very low confidence in available evidence.❞
Since the benefit of posture correctors like this one is due to reminding the wearer to keep good posture, there is a lot more (good quality!) science for wearable biofeedback tech devices, such as this one:
Spine Cop: Posture Correction Monitor and Assistant
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Energy Plan – by James Collins

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There’s a lot of conflicting advice out there about how we should maintain our energy levels, for example:
- Eat fewer carbs!
- Eat more carbs!
- Eat slow-release carbs!
- Eat quick-release carbs!
- Practise intermittent fasting!
- Graze constantly throughout the day!
- Forget carbs and focus on fats!
- Actually it’s all about B-vitamins!
…and so on.
What Collins does differently is something much less-often seen:
Here, we’re advised on how to tailor our meals to our actual lifestyle, taking into account the day we actually have each day. For example:
- What will our energy needs be for the day?
- Will our needs be intense, or long, or both, or neither?
- What kind of recovery have we had, or do we need, from previous activities?
- Do we need to replace lost muscle glycogen, or are we looking to trim the fat?
- Are we doing a power-up or just maintenance today?
Rather than bidding us have a five-way spreadsheet and do advanced mathematics for every meal, though, Collins has done the hard work for us. The book explains the various principles in a casual format with a light conversational tone, and gives us general rules to follow.
These rules cover what to do for different times of day… and also, at different points in our life (the metabolic needs of a 13-year-old, 33-year-old, and 83-year-old, are very different!). That latter’s particularly handy, as a lot of books assume an age bracket for the reader, and this one doesn’t.
In short: a great book for anyone who wants to keep their energy levels up (throughout life’s ups and downs in activity) without piling on the pounds or starving oneself.
Click here to check out The Energy Plan on Amazon and fuel your days better!
Share This Post
-

What is cannabis use disorder? And how do you know if you have a problem?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Around 41% of Australians report they’ve used cannabis at some point in their life.
Research estimates that 22% of recreational cannabis consumers meet criteria for a cannabis use disorder. This condition can make it difficult to control how often or how much cannabis they use.
For medicinal cannabis, our research estimated the percentage of cannabis consumers who meet criteria for a cannabis use disorder was similar, around 25%.
These figures may come as a surprise, as the perceived risks associated with cannabis have been steadily declining in many countries.
So, how can you tell if your cannabis use is a problem?
What does cannabis use disorder look like?
A person might use cannabis to relax after a stressful day at work or to help them sleep. At first, they might do so every now and then. But over time, they might come to rely on using cannabis to stop feeling uncomfortable, stressed and sleepless.
They might begin to use cannabis daily to feel “normal”.
With regular use, the body develops tolerance to the effects of cannabis. So the person needs to use more cannabis to get the same “high”.
People who consume cannabis might use more cannabis than they intended or might have problems performing at work because they’re high at the start of the work day, or they fail to do important things such as paying bills, and buy cannabis instead.
The person might keep using cannabis despite noticing their use is causing clouded thoughts, memory issues and anxiety.
Friends and family might notice problems with their cannabis use and recommend they stop or cut back. This can be difficult for people with cannabis use disorder because they may feel anxious, irritable and have difficulty sleeping if they suddenly stop using cannabis.

Some people who use cannabis can’t function like they used to. PeopleImages.com – Yuri A/Shutterstock These withdrawal symptoms can make it harder to quit or cut back. Withdrawal symptoms are quickly relieved by using cannabis, creating a cycle of relapse.
How is it diagnosed?
Health professionals use specific criteria to diagnose a cannabis use disorder.
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM), a person may have a cannabis use disorder if they show at least two symptoms within one year. Symptoms can include:
- using larger amounts over longer periods than intended
- cravings for cannabis, where the person feels a strong urge or desire to use cannabis
- trying and failing to cut back on cannabis use
- continuing cannabis use despite worsening physical or psychological problems
- failing to fulfil major role obligations at work, school or home
- needing to use a greater amount for the same effect, known as tolerance
- experiencing withdrawal symptoms such as feeling anxious, irritable or having trouble sleeping.
According to the DSM, two to three symptoms indicate a mild cannabis use disorder and few problems. A moderate disorder involves four to five symptoms, while six-plus symptoms means a severe disorder.
Who is at greatest risk?
In both recreational and medicinal consumers, the risk of cannabis use disorder is higher for people who use cannabis:
- frequently, especially daily
- by smoking or vaping
- with higher levels of THC or in larger amounts.
Other risk factors are starting cannabis use at a younger age and using cannabis to relieve symptoms of anxiety, depression and chronic pain.
What’s the relationship with chronic pain?
People struggling to manage their pain may turn to cannabis hoping to find relief.
However, recent studies question the effectiveness of cannabis to manage pain.
People who use cannabis to relieve chronic pain often use it more frequently. AYO Production/Shutterstock So people may increase how often they use cannabis or use more potent cannabis products in an unsuccessful attempt to control their pain.
This can lead to a cannabis use disorder, making it more difficult to manage their pain and impairing their ability to cope with the demands of everyday life.
How to reduce your risk
Legal changes in many countries, including Australia, have allowed greater access to cannabis for medical reasons. People now often use cannabis for both recreational and medical reasons (dual-use).
If you use cannabis, reduce your risk of developing a cannabis use disorder by avoiding daily use and avoiding cannabis products with high THC.
If you’re concerned about your cannabis use, consult your medical practitioner or contact the National Alcohol and Other Drug Hotline on 1800 250 015 for confidential advice.
Danielle Dawson, PhD Candidate, School of Psychology and National Centre for Youth Substance Use Research, The University of Queensland; Valentina Lorenzetti, Deputy Director, Healthy Brain and Mind Research Centre Program Lead, Neuroscience of Addiction and Mental Health Program, Australian Catholic University, and Wayne Hall, Emeritus Professor, National Centre for Youth Substance Use Research, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Celery vs Parsley – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing celery to parsley, we picked the parsley.
Why?
Firstly, you may be thinking: “What kind of a comparison is this?! Parsley is a seasoning or a garnish; who uses it as a salad option option?!” and the answer is that nobody can stop you from using herbs as a main greenery option, and in fact, we recommend it (both for adding a lot of flavor to your plate, and getting in a lot of nutrients).
So, with that in mind, let’s get to it:
In terms of macros, parsley has 2x the fiber for 2x the carbs and 5x the protein, winning in this category easily.
In the category of vitamins, celery is not higher in any vitamins, while parsley has a lot more of vitamins A, B1, B2, B3, B5, B6, B7, B9, C, E, and K, sweeping its second round completely.
Looking at minerals, celery does have more selenium, while parsley has a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc, convincingly winning its third round in a row.
In other considerations, they both are great sources of polyphenols, though celery (albeit notably the leaves thereof, not the stalks so much) does have more flavonoids specifically, and may arguably pick up a point here.
Adding up the sections makes for a clear overall win for parsley, but by all means do enjoy either or both, as diversity is best!
(Unless you are allergic to celery, in which case, definitely do stick the parsley!)
Want to learn more?
You might like:
Invigorating Sabzi Khordan ← another great way to enjoy parsley as main ingredient rather than just a seasoning
Enjoy!
Share This Post





Related Posts
-

Healing Your Gut: Anastasia’s Journey and Tips
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anastasia Gurova shares her inspiring journey from chronic gut issues to vibrant health.
A Personal Journey to Gut Health
In the below video, Anastasia shares her long struggle with gut problems, including SIBO, IBS, and gastritis. She talks about ending up in the hospital with severe bloating, only to find that a range of medical approaches didn’t provide her with any lasting relief. This led her to explore the importance of the microbiome and its crucial role in gut health, which is what we’ll be focusing on in this overview.
Key Insights and Tips
The most valuable parts of Anastasia’s story for 10almonds readers are, in our opinion, the solutions she discovered to her gut issues. You’ll have to watch her video to discover all of them, but here are some of our favorites:
- Reintroduce Whole Grains and Legumes: Despite the popularity of grain-free diets, Anastasia found significant improvements in her gut health by adding whole grains like quinoa, oats, and buckwheat back into her diet. These foods provide essential fibers that feed beneficial gut bacteria.
- Soaking and Fermenting Foods: To make grains and legumes more digestible, Anastasia recommends soaking them overnight. This is similar to the common technique people use on oats. She also includes fermented foods like sauerkraut, kimchi, and yogurt in her diet, which introduce beneficial bacteria to the gut.
- Resistant Starches: Foods like cooked and cooled rice, potatoes, and green bananas contain resistant starches that promote healthy gut bacteria. Anastasia emphasizes incorporating these into meals to support gut health.
- Mindful Eating: Anastasia found that taking time to chew food thoroughly and savor each bite helped improve her digestion. She avoids distractions like TV while eating and pays attention to the textures and flavors of her meals.
- Avoid Overly Restrictive Diets: Anastasia warns against overly restrictive diets like keto and strict SIBO diets that cut out all carbs and fiber. These can worsen gut health by starving beneficial bacteria.
That’s Only The Beginning
Anastasia’s video goes far beyond what we’ve covered in this short introduction; she provides a detailed look at the steps she took, from dietary changes to lifestyle adjustments, and offers tips that anyone can apply. Plus, she explains the science behind these changes, which, of course, we love.
Enjoy the video! (It would be remiss for us to not bring up our general intro to gut health, or our more specific article on the gut-brain connection)
Good luck on your gut-health journey!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Parenting a perfectionist? Here’s how you can respond
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Some children show signs of perfectionism from early on. Young children might become frustrated and rip up their drawing if it’s not quite right. Older children might avoid or refuse to do homework because they’re afraid to make a mistake.
Perfectionism can lead to children feeling overwhelmed, angry and frustrated, or sad and withdrawn.
And yet perfectionism isn’t considered all bad in our society. Being called a “perfectionist” can be a compliment – code for being a great worker or student, someone who strives to do their best and makes sure all jobs are done well.
These seemingly polarised views reflect the complex nature of perfectionism.
Annie Spratt/Unsplash What is perfectionism?
Researchers often separate perfectionism into two parts:
- perfectionistic strivings: being determined to meet goals and achieve highly
- perfectionistic concerns: worry about being able to meet high standards, and self-criticism about performance.
While perfectionistic strivings can be positive and lead to high achievement, perfectionistic concerns can lead to a higher chance of children developing eating disorders or anxiety and depression, and having lower academic achievement.
Perfectionistic concerns can result in lower academic achievement. Jessica Lewis/Unsplash Children and adolescents may experience perfectionism in relation to school work, sport, performance in art or music, or in relation to their own body.
Signs of perfectionistic concerns in children and adolescents may include:
- children being highly critical of themselves
- their reactions to mistakes seeming to be an overreaction
- intense preoccupation and worry over their standards and goals and/or procrastination
- significant change in performance, for example, lower academic results
- irritability and negative emotions, stress and feelings of worthlessness
- social problems with peers and friends, such as bullying and alienating themselves from peers.
A range of genetic, biological and environmental factors influence perfectionism in children. And as a parent, our role is important. While research evidence suggests we can’t successfully increase positive perfectionistic strivings in our children, harsh or controlling parenting can increase negative perfectionistic concerns in children.
Parents who are perfectionistic themselves can also model this to their children.
So, how can we walk the line between supporting our child’s interests and helping them to achieve their potential, without pressuring them and increasing the risk of negative outcomes?
Give them space to grow
A great metaphor is the gardener versus the carpenter described by psychology professor Alison Gopnik.
Instead of trying to build and shape our children by controlling them and their environment (like a carpenter), parents can embrace the spirit of the gardener – providing lots of space for children to grow in their own direction, and nourishing them with love, respect and trust.
Parents don’t need to control their child and their environment. Noah Silliman/Unsplash We can’t control who they become, so it’s better to sit back, enjoy the ride, and look forward to watching the person they grow into.
However, there is still plenty we can do as parents if our child is showing signs of perfectionism. We can role model to our children how to set realistic goals and be flexible when things change or go wrong, help our children manage stress and negative emotions, and create healthy balance in our family daily routine.
Set realistic goals
People with perfectionistic tendencies will often set unattainable goals. We can support the development of flexibility and realistic goal setting by asking curious questions, for example, “what would you need to do to get one small step closer to this goal?” Identifying upper and lower limits for goals is also helpful.
If your child is fixed on a high score at school, for example, set that as the “upper limit” and then support them to identify a “lower limit” they would find acceptable, even if they are less happy with the outcome.
This strategy may take time and practice to widen the gap between the two, but is useful to create flexibility over time.
If a goal is performance-based and the outcome cannot be guaranteed (for example, a sporting competition), encourage your child to set a personal goal they have more control over.
Parents can help children set goals they can achieve. liz99/Unsplash We can also have conversations about perfectionism from early on, and explain that everyone makes mistakes. In fact, it’s great to model this to our children – talking about our own mistakes and feelings, to show them that we ourselves are not perfect.
Talk aloud practices can help children to see that we “walk the walk”. For example, if you burn dinner you could reflect:
I’m disappointed because I put time and effort into that and it didn’t turn out as I expected. But we all make mistakes. I don’t get things right every time.
Manage stress and negative emotions
Some children and adolescents have a natural tendency towards perfectionism. Rather than trying to control their behaviour, we can provide gentle, loving support.
When our child or adolescent becomes frustrated, angry, sad or overwhelmed, we support them best by helping them to name, express and validate all of their emotions.
Parents may fear that acknowledging their child’s negative emotions will make the emotions worse, but the opposite is true.
Creating healthy balance
The building blocks of healthy child development are strong loving family relationships, good nutrition, creative play and plenty of physical activity, sleep and rest.
Perfectionism is associated with rigidity, and thinking that there is only one correct way to succeed. We can instead encourage flexibility and creativity in children.
Children’s brains grow through play. There is strong research evidence showing that creative, child-led play is associated with higher emotion regulation skills, and a range of cognitive skills, including problem-solving, memory, planning, flexibility and decision-making.
Play helps children’s brains grow. Mi Pham/Unsplash Play isn’t just for young children either – there’s evidence that explorative, creative play of any kind also benefits adolescents and adults.
There is also evidence that getting active outdoors in nature can promote children’s coping skills, emotion regulation and cognitive development.
Elizabeth Westrupp, Associate Professor in Psychology, Deakin University; Gabriella King, Associate Research Fellow, Deakin University, and Jade Sheen, Associate Professor, School of Psychology, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Fix 90% Of Your Body’s Problems In 30 Days
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to mobility problems and associated pain, the key is targeting the root cause, not doing random stretches (bearing in mind, random stretches might actually make some things worse in some cases, if an underlying problem isn’t addressed first).
Targeting weak points to fix
Here are 7 exercises that, between them, will cover most bases. However, you may also wish to just do the one(s) that pertain(s) to your specific mobility issue and/or pain, per the descriptions. If that’s you, then by all means go for it; simply doing what you need to in a targeted fashion is very much the spirit of what this is about; you don’t have to do everything all the time, or else health and fitness would be truly a full-time occupation, and more!
The exercises:
- 90/90 knee drops: improve hip internal/external rotation to reduce strain on knees, ankles, and lower back; perform slowly with control, using regressions if needed (10–20 reps per side).
- Deep squat with reach: open hips and improve torso rotation by squatting deeply, pushing knees out with elbows, and alternating arm reaches while looking up (3–5 reps per side).
- Banded glute bridges: strengthen glutes to support proper running mechanics and reduce knee/lower back strain by engaging the core, lifting hips, and resisting inward knee movement (10–15 reps).
- Hip flexor & hamstring rock-backs: alternate between forward lunge to stretch hip flexors and rocking back to stretch hamstrings, addressing tightness from prolonged sitting (5 reps per leg).
- Thread the needle: improve upper back mobility and posture by threading one arm under the body while on hands and knees, holding at the bottom briefly (5–10 reps per side).
- Stork stand: build balance and stability—stand on one leg for 30 seconds, then with eyes closed; improves coordination and is linked to longevity and injury prevention.
- Lunge with rotation: combine deep lunge, elbow-to-ankle, and upward arm reach to stretch hip flexors, hamstrings, back, and improve rotation (5 reps per side, optional progression by lifting back knee).
For more on each of these, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Best Mobility Exercises For Each Joint
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: