Vegan Eager for Milk Alternatives
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Q: Thanks for the info about dairy. As a vegan, I look forward to a future comment about milk alternatives
Thanks for bringing it up! What we research and write about is heavily driven by subscriber feedback, so notes like this really help us know there’s an audience for a given topic!
We’ll do a main feature on it, to do it justice. Watch out for Research Review Monday!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Functional Exercise For Seniors – by James Atkinson

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of exercises books are tailored to 20-year-old athletes training for their first Tough Mudder. Others, that the only thing standing between us and a perfect Retroflex Countersupine Divine Pretzel position is a professionally-lit Instagrammable photo.
This one’s not like that.
But! Nor does it think being over a certain age is a reason to not have genuinely robust health, of the kind that may make some younger people envious. So, it lays out, in progressive format, guidelines for exercises targeted at everything we need to build and maintain as we get older.
The writing style is clear, and the illustrations too (the cover art is the same style as the illustrations inside).
Bottom line: if you’re looking for a workout guide that understands you are nearer 80 than 18, and/but also doesn’t assume your age limits your exercise potential to “wrist exercises in chair”, then this book is a fine pick.
Share This Post
-

Anti-Inflammatory Brownies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Brownies are usually full of sugar, butter, and flour. These ones aren’t! Instead, they’re full of fiber (good against inflammation), healthy fats, and anti-inflammatory polyphenols:
You will need
- 1 can chickpeas (keep half the chickpea water, also called aquafaba, as we’ll be using it)
- 4 oz of your favorite nut butter (substitute with tahini if you’re allergic to nuts)
- 3 oz rolled oats
- 2 oz dark chocolate chips (or if you want the best quality: dark chocolate, chopped into very small pieces)
- 3 tbsp of your preferred plant milk (this is an anti-inflammatory recipe and unfermented dairy is inflammatory)
- 2 tbsp cocoa powder (pure cacao is best)
- 1 tbsp glycine (if unavailable, use 2 tbsp maple syrup, and skip the aquafaba)
- 2 tsp vanilla extract
- ½ tsp baking powder
- ¼ tsp low-sodium salt
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 350℉ / 180℃, and line a 7″ cake tin with baking paper.
2) Blend the oats in a food processor, until you have oat flour.
3) Add all the remaining ingredients except the dark chocolate chips, and process until the mixture resembles cookie dough.
3) Transfer to a bowl, and fold in the dark chocolate chips, distributing evenly.
4) Add the mixture to the cake tin, and smooth the surface down so that it’s flat and even. Bake for about 25 minutes, and let them cool in the tin for at least 10 minutes, but longer is better, as they will firm up while they cool. Cut into cubes when ready to serve:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
- Cacao vs Carob – Which is Healthier?
- Keep Inflammation At Bay
- The Sweet Truth About Glycine
- The Best Kind Of Fiber For Overall Health?
Take care!
Share This Post
-
Keep Cellulite At Bay
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Does anything actually get rid of cellulite? Nothing seems to❞
Let’s get the bad news over with in one go:
Nothing (that the scientific world currently knows of) can get rid of cellulite permanently, nor completely guard against it proactively. Which, given that it affects up to 98% of women to some degree, and often shows up not long after puberty (though it can appear at any time and often increases later in life), any pre-emptive health regime would need to be started as a child in any case.
As with many things that predominantly affect women, the world of medicine isn’t entirely sure what causes it, let alone how to effectively treat it.
Obviously hormones are implicated, namely estrogen.
Obviously adiposity is implicated, because one can’t have dimples in one’s fat if one doesn’t have enough fat to dimple.
Other hypothesized contributory factors include genetics, poor diet, inactivity, unhealthy lifestyle (in ways not previously mentioned, e.g. use of alcohol, tobacco, etc), accumulated toxins, and pregnancy.
Here’s an old paper (from 2004); today’s reviews say pretty much the same thing, but we love how succinctly (albeit, somewhat depressingly) this abstract states how little we know and how little we can do:
Cellulite: a review of its physiology and treatment
However, all is not lost!
There are some things that can affect how much cellulite we get, and there are some things that can reduce it, and even some things that can get rid of it completely—albeit temporarily.
First, a quick refresher on what it actually is, physiologically speaking: cellulite occurs when connective tissue bands pull the skin down in places, where fat tissue has been able to squeeze through. One of the reasons it is hypothesized women get this more than men is because our fat is not merely different in distribution and overall percentage, but also in how the fat cells stack up; we generally have have of a vertical stacking structure going on, while men generally have a more horizontal structure. This means that it can be easier for ours to get moved about differently, causing the connective tissue to pull on the skin unevenly in places.
With that in mind…
Prevention is, as we say, probably impossible if your body is running on estrogen. However, those contributory factors we mentioned above? Most of those are modifiable, including these things that it is hypothesized can reduce it:
Diet: as it seems to be worsened by inflammation (what isn’t?), an anti-inflammatory diet is recommended.
Exercise: there are three things here: 1) exercises to improve circulation and thus the body’s ability to sort things out by itself 2) HIIT exercise to reduce body fat percentage, if one has a high enough starting body fat percentage for that to be a healthy goal 3) mobility exercises, to ensure our connective tissues are the right amount of mobile.
Creams and lotions
These reduce the superficial appearance of cellulite, without actually treating the thing itself. Mostly they are caffeine-based, which when used topically increases blood flow and works as a local diuretic, reducing the water content of the fat cells, diminishing the appearance of the cellulite by making each fat cell physically smaller (while still containing the same amount of fat, and it’ll bounce back in size as soon as the body can restore osmotic balance).
Medical procedures
There are too many of these to discuss them all separately, but they all work on the principle of breaking up the tough bands of connective tissue to eliminate the dimpling of cellulite.
The methods they use vary from ultrasound to cryolipolysis to lasers to “vacuum-assisted precise tissue release”, which involves a suction pump and a multipronged robotic assembly with needles to administer anaesthetic as it goes and small blades to cut the connective tissues under the skin:
Tissue Stabilized–Guided Subcision for the Treatment of Cellulite
That last one definitely sounds like the least fun, but it’s also the only one that doesn’t take months to maybe see results.
Cellulite can and almost certainly will come back after all of these.
Home remedies
Aside from at-home versions of the above (not the robots with vacuum pumps and needles and microblades, hopefully, but for example homemade caffeine creams), and of course diet and exercise which can be considered “home remedies”, there are two more things worth mentioning:
Dry brushing: using a body brush to, as the name suggests, simply brush one’s skin. The “dry” aspect here is simply that it’s not done in the bath or shower; it’s done while dry. It can improve local circulation of blood and lymph, allowing for better detoxification and redistribution of needed bodily resources.
Here’s an example dry brushing body brush on Amazon; this writer has one and hates it, but I’ve also tried with other kinds of brush and hate them too, so it seems to be a me thing rather than a brush thing, and I have desisted in trying, now. Maybe you will like it better; many people do.
Self-massage: or massage by someone else, if that’s an option for you and you prefer. In this case, it works by a different mechanism than dry brushing; this time it’s working by the same principle as the medical techniques described in the previous section; it’s physically breaking down the toughened bits of connective tissue.
Here’s an example wooden massage roller on Amazon; this writer has one and loves it; it’s sooooooo good. I got it as a matter of general maintenance for my fascia, but it’s also very good if I get a muscular pain now and again. As for cellulite, I personally get just a little cellulite sometimes (in the backs of my thighs), and whenever I use this regularly, it goes away for at least a while.
A quick note in closing
Cellulite is normal for women and is not unhealthy. Much like gray hair for example, it’s something that can be increased by poor health, but the thing itself isn’t intrinsically unhealthy, and most of us get it to some degree at some point.
Nevertheless, aesthetic factors can also have a role to play in mental health, and we tend to feel best when we like the way our body looks. If for you that means wanting less/no cellulite, then the above are some ways towards that.
As a bonus, most of the nonmedical options are directly good for the physical health anyway, so doing them is of course good.
In particular that last one (the wooden massage roller), because that connective tissue we talked about? It matters for a lot more than just cellulite, and is heavily implicated in a lot of kinds of chronic pain, so it pays to keep it in good health:
Fascia: Why (And How) You Should Take Care Of Yours
(that article, also written by this same writer by the way, suggests a vibrating foam roller—those are very popular; I just really love my wooden one, and find it more effective)
Take care!
Share This Post


Related Posts
-

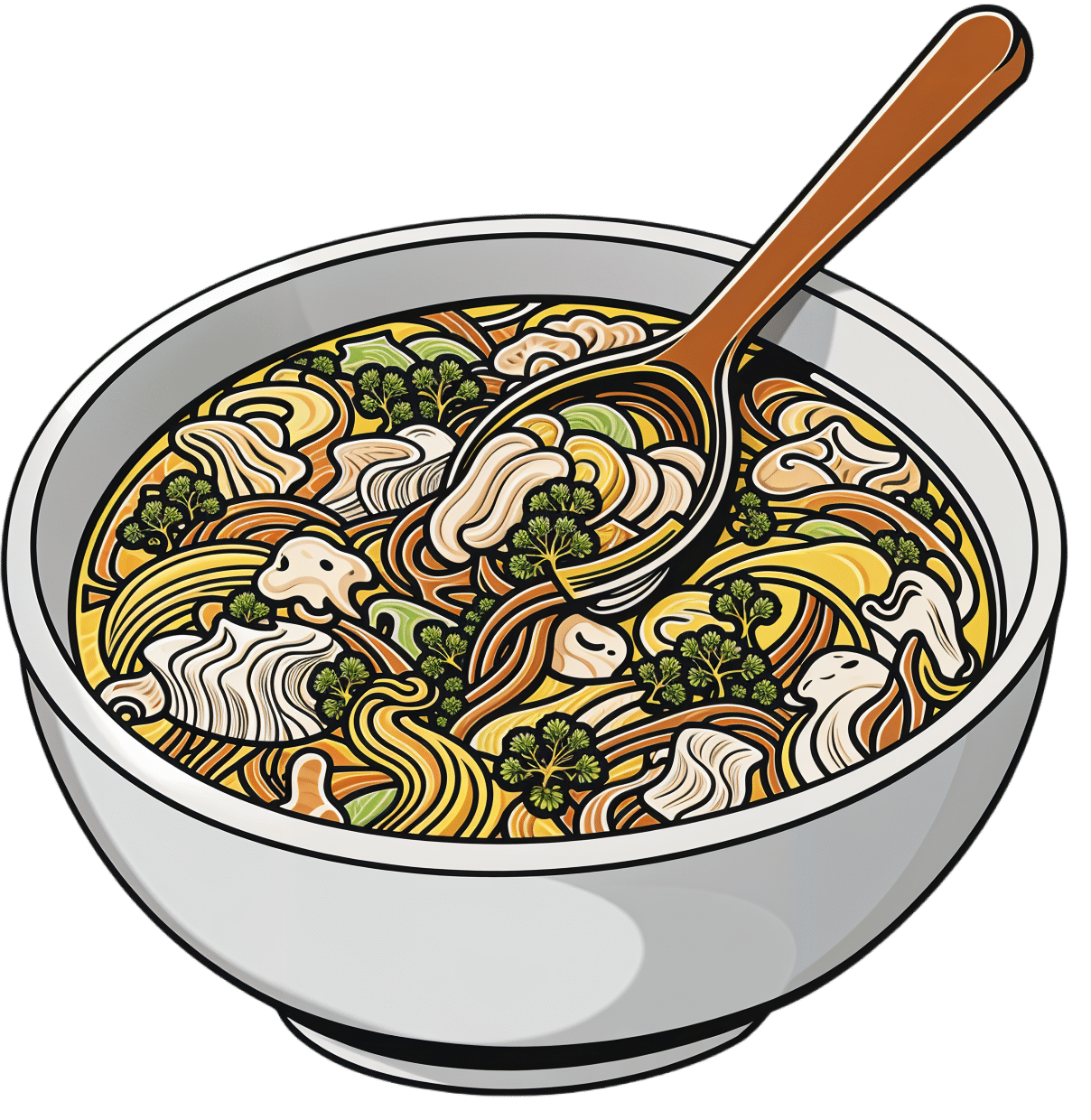
Hot And Sour Shiitake Soup
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a popular, easy, and delicious soup that nonetheless is not found in many western kitchens, despite being enjoyed in restaurants/take-out. Best of all, making it at home means that you know all the ingredients, can account for quality, and also can customize it per your preferences (i.e. how much heat/sourness you like).
You will need
- 3 cups shiitake mushrooms, sliced
- 3 cups bok choy, chopped
- 2 cups cherry tomatoes, quartered
- 1 cup carrot, grated
- 3 spring onions, chopped
- 2 shallots, sliced lengthways
- 2 serrano chilis (or similar), sliced thinly
- 2 tbsp apple cider vinegar
- 1 tbsp lemon juice
- 1 tbsp fresh ginger, sliced into 1″ strips
- 1 tsp black pepper, coarse ground
- ½ bulb garlic, crushed
- 6 cups low-sodium vegetable stock. Ideally you will have made it yourself from vegetable cuttings that you saved in the freezer until you had enough to make stock from, but if that’s not an option, then low-sodium vegetable stock cubes can be purchased and used.
- Garnish: ¼ cup (or 4 tbsp) cilantro, chopped, or if you have the soap gene, then this time we recommend chopped basil as the subsitution
Method
(we suggest you read everything at least once before doing anything)
1) Put the ginger in a big pot with the stock; cover and simmer for about 20 minutes (otherwise the ginger flavor will remain mostly concentrated in the ginger strips).
2) Bring it to a boil and add the bok choy, mushrooms, shallots, chili peppers, and the carrot; simmer for another 5 minutes
3) Add the remaining ingredients except for the garnish, and simmer for another 5 minutes
4) Serve, adding the garnish

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- The (Longevity) Magic of Mushrooms
- Our Top 5 Spices: How Much Is Enough For Benefits?
- An Apple (Cider Vinegar) A Day…
- Enjoy Bitter/Hot/Sour/Pungent Foods For Your Heart & Brain
- Brain Food? The Eyes Have It!
- Some Surprising Truths About Hunger And Satiety
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Can You Repair Your Own Teeth At Home?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝I liked your article on tooth remineralization, I saw a “home tooth repair kit”, and wondered if it is as good as what dentists do, or at least will do the job well enough to save a dentist visit?❞
Firstly, for any wondering about the tooth remineralization, here you go:
Tooth Remineralization: How To Heal Your Teeth Naturally
Now, to answer your question, we presume you are talking about something like this kit available on Amazon. In which case, some things to bear in mind:
- This kind of thing is generally intended as a stop-gap measure until you see a dentist, because you cracked your tooth or lost a filling or something today, and will see the dentist next week, say.
- This kind of thing is not what Dr. Michelle Jorgensen was talking about in another video* that we wrote about; rather, it is using a polymer filler to rebuild what is missing. The key difference is: this is using plastic, which is not what your teeth are made of, so it will never “take” as part of the tooth, as some biomimetic dentistry options can do.
- Yes, this does also mean you are putting microplastics (because the powder is usually micronized polymer beads with zinc oxide, to which you add a liquid to create a paste that will set) in your mouth and quite possibly right next to an open blood supply depending on what’s damaged and whether capillaries were reaching it.
- Because of the different material and application method, the adhesion is nothing like professional fillings (be they metal or resin), and thus the chances of it coming out again or so high that it’s more a question of when, rather than if.
- If you have damage under there (as we presume you do in any scenario where you are using this), then if it’s not professionally cleaned before the filling goes in, then it can get infected, and (less dramatically, but still importantly) any extant decay can also get worse. We say “professionally”, because you will not be able to do an adequate job with your toothbrush, floss, etc at home, and even if you got dentist’s tools (which you can buy, by the way, but we don’t recommend), you will no more be able to do the same quality job as a dentist who has done that many times a day every day for the past 20 years, as buying expensive paintbrushes would make you able to restore a Renaissance painting without messing it up.
*See: Dangers Of Root Canals And Crowns, & What To Do Instead ← what she recommends instead is biomimetic dentistry, which is also more prosaically called “conservative restorative dentistry”, i.e. it tries to conserve as much as possible, replace lost material on a like-for-like basis, and generally end up with a result that’s as close to natural as possible.
In other words, the short answer to your question is “no, sorry, it isn’t and it won’t”
However! A just like it’s good to have a first aid kit in the house even if it won’t do the same job as an ambulance crew, it can be good to have a tooth repair kit (essentially, a tooth first-aid kit) in the house, precisely to use it just as a stop-gap measure in the event that you one day crack a tooth or lose a filling or such, and don’t want to leave it open to all things in the meantime.
(The results of this sort of kit are so not long-term in nature that it will be quick and easy for your dentist to remove it to do their own job once you get there)
If in doubt, always see your dentist as soon as possible, as many things are a lot less work to treat now, than to treat later. Just, make sure to advocate for yourself and what you actually want/need, and don’t let them upsell you on something you didn’t come in for while you’re sitting in their chair—that’s a conversation to be had in advance with a clear head and no pressure (and nobody’s hands in your mouth)!
See also: Dentists Are Pulling ‘Healthy’ and Treatable Teeth To Profit From Implants, Experts Warn
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
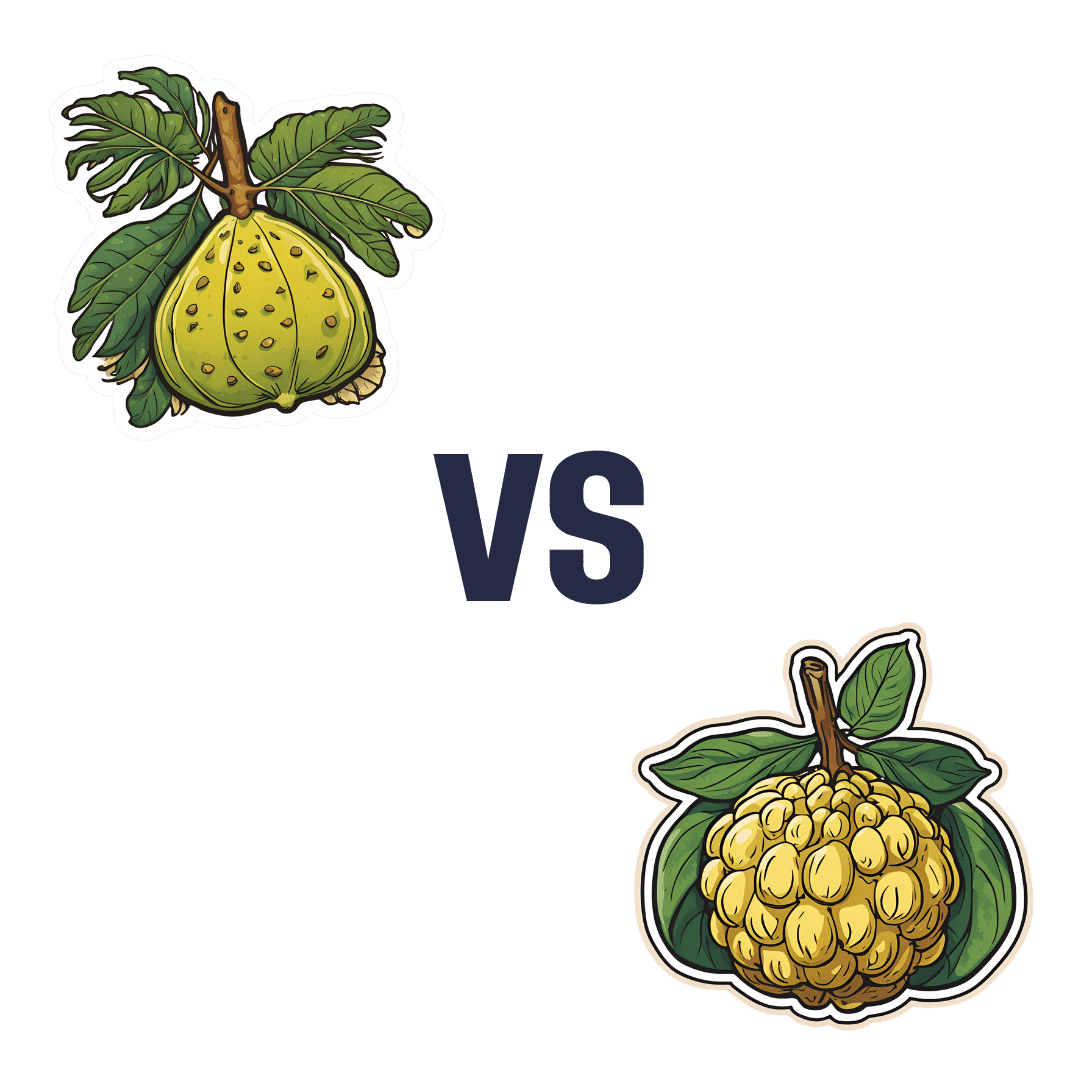
Breadfruit vs Custard Apple – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing breadfruit to custard apple, we picked the breadfruit.
Why?
Today in “fruits pretending to be less healthy things than they are”, both are great, but one of these fruits just edges out the other in all categories. This is quite simple today:
In terms of macros, being fruits they’re both fairly high in carbs and fiber, however the carbs are close to equal and breadfruit has nearly 2x the fiber.
This also means that breadfruit has the lower glycemic index, but they’re both medium-low GI foods with a low insulin index.
When it comes to vitamins, breadfruit has more of vitamins B1, B3, B5, and C, while custard apple has more of vitamins A, B2, and B6. So, a 4:3 win for breadfruit.
In the category of minerals, breadfruit has more copper, magnesium, phosphorus, potassium, and zinc, while custard apple has more calcium and iron.
In short, enjoy both, but if you’re going just for one, breadfruit is the healthiest.
Want to learn more?
You might like to read:
Which Sugars Are Healthier, And Which Are Just The Same?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: