The Twenty-Four Hour Mind – by Dr. Rosalind Cartwright
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed books about sleep before, and even about dreaming, so what does this one have to offer that’s new?
Quite a lot, actually! Before Dr. Cartwright, there were mainly two models of sleep and dreaming:
- The “top-down” model of psychoanalysts: our minds shape our dreams which in turn reveal things about us as people
- The “bottom-up” model of neuroscientists: our brains need to go through regular maintaince cycles, of which vivid hallucinations are a quirky side-effect.
And now, as Dr. Cartwright puts it:
❝I will lay out a new [horizontal] psychological model of the twenty-four hour mind; that is, how the predominantly conscious (waking) and unconscious (sleeping) forms of mental behavior interact through the brain’s regular, but differently organized, states of waking, sleeping, and dreaming.❞
This she does in the exploratory style of a 224-page lecture, which sounds like it might be tedious, but is actually attention-grabbing and engaging throughout. This book is more of a page-turner than soporific bedtime reading!
Bottom line: if you’d like to know more about the effect your waking and sleeping brain have on each other (to include getting in between those and making adjutments as appropriate), this is very much an elucidating read!
Click here to check out The Twenty-Four Hour Mind, and learn more about yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Heart Healthy Diet Plan – by Stephen William

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve covered heart-healthy cooking books before, but variety is good, and boredom is an enemy of health, so let’s shake it up with a fresh stack of recipes!
After a brief overview of the relevant science (which if you’re a regular 10almonds reader, probably won’t be new to you), the author takes the reader on a 28-day journey. Yes, we know the subtitle says 30 days, but unless they carefully hid the other two days somewhere we didn’t find, there are “only” 28 inside. Perhaps the publisher heard it was a month and took creative license. Or maybe there’s a different edition. Either way…
Rather than merely giving a diet plan (though yes, he also does that), he gives a wide range of “spotlight ingredients”, such that many of the recipes, while great in and of themselves, can also be jumping-off points for those of us who like to take recipes and immediately do our own things to them.
Each day gets a breakfast, lunch, dinner, and he also covers drinks, desserts, and such like.
Notwithstanding the cover art being a lot of plants, the recipes are not entirely plant-based; there are a selection of fish dishes (and other seafood, e.g. shrimp) and also some dairy products (e.g. Greek yoghurt). The recipes are certainly very “plant-forward” though and many are just plants. If you’re a strict vegan though, this probably isn’t the book for you.
Bottom line: if you’d like to cook heart-healthy but are often stuck wondering “aaah, what to cook again today?”, then this is the book to get you out of any culinary creative block!
Click here to check out the Heart Healthy Diet Plan, and widen your heart-healthy repertoire!
Share This Post
-

Why You Can’t Skimp On Amino Acids
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our body requires 20 amino acids (the building blocks of protein), 9 of which it can’t synthesize (thus called: “essential”) and absolutely must get from food. Normally, we get these amino acids from protein in our diet, and we can also supplement them by taking amino acid supplements if we wish.
Specifically, we require (per kg of bodyweight) a daily average of:
- Histidine: 10 mg
- Isoleucine: 20 mg
- Leucine: 39 mg
- Lysine: 30 mg
- Methionine: 10.4 mg
- Phenylalanine*: 25 mg
- Threonine: 15 mg
- Tryptophan: 4 mg
- Valine: 26 mg
*combined with the non-essential amino acid tyrosine
Source: Protein and Amino Acid Requirements In Human Nutrition: WHO Technical Report
Why this matters
A lot of attention is given to protein, and making sure we get enough of it, especially as we get older, because the risk of sarcopenia (muscle mass loss) increases with age:
However, not every protein comes with a complete set of essential amino acids, and/or have only trace amounts of of some amino acids, meaning that a dietary deficiency can arrive if one’s diet is too restrictive.
And, if we become deficient in even just one amino acid, then bad things start to happen quite soon. We only have so much space, so we’re going to oversimplify here, but:
- Histidine: is needed to produce histamine (vital for immune responses, amongst other things), and is also important for maintaining the myelin sheaths on nerve cells.
- Isoleucine: is very involved in muscle metabolism and makes up the bulk of muscle tissue.
- Leucine: is critical for muscle synthesis and repair, as well as wound healing in general, and blood sugar regulation.
- Lysine: is also critical in muscle synthesis, as well as calcium absorption and hormone production, as well as making collagen.
- Methionine: is very important for energy metabolism, zinc absorption, and detoxification.
- Phenylalanine: is a necessary building block of a lot of neurotransmitters, as well as being a building block of some amino acids not listed here (i.e., the ones your body synthesizes, but can’t without phenylalanine).
- Threonine: is mostly about collagen and elastin production, and is also very important for your joints, as well as fat metabolism.
- Tryptophan: is the body’s primary precursor to serotonin, so good luck making the latter without the former.
- Valine: is mostly about muscle growth and regeneration.
So there you see, the ill effects of deficiency can range from “muscle atrophy” to “brain stops working” and “bones fall apart” and more. In short, any essential amino acid deficiency not remedied will ultimately result in death; we literally become non-viable as organisms without these 9 things.
What to do about it (the “life hack” part)
Firstly, if you eat a lot of animal products, those are “complete” proteins, meaning that they contain all 9 essential amino acids in sensible quantities. The reason that all animal products have these, is because they are just as essential for the other animals as they are for us, so they, just like us, must consume (and thus contain) them.
However, a lot of animal products come with other health risks:
Do We Need Animal Products To Be Healthy? ← this covers which animal products are definitely very health-risky, and which are probably fine according to current best science
…so many people may prefer to get more (or possibly all) dietary protein from plants.
However, plants, unlike us, do not need to consume all 9 essential amino acids, and this may or may not contain them all.
Soy is famously a “complete” protein insofar as it has all the amino acids we need.
But what if you’re allergic to soy?
Good news! Peas are also a “complete” protein and will do the job just fine. They’re also usually cheaper.
Final note
An oft-forgotten thing is that some other amino acids are “conditionally essential”, meaning that while we can technically synthesize them, sometimes we can’t synthesize enough and must get them from our diet.
The conditions that trigger this “conditionally essential” status are usually such things as fighting a serious illness, recovering from a serious injury, or pregnancy—basically, things where your body has to work at 110% efficiency if it wants to get through it in one piece, and that extra 10% has to come from somewhere outside the body.
Examples of commonly conditionally essential amino acids are arginine and glycine.
Arginine is critical for a lot of cell-signalling processes as well as mitochondrial function, as well as being a precursor to other amino acids, including creatine.
As for glycine?
Check out: The Sweet Truth About Glycine
Enjoy!
Share This Post
-

Seed Saving Secrets – by Alice Mirren
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We all know that home-grown is best, and yet many of us are not exactly farmers (this reviewer tries with mixed results—hardy crops survive; others, not so much). While it’s easy to blame the acidic soil, the harsh climate, or not having enough time and money (this reviewer blames all of the above), the fact remains that a skilled gardener can produce a good crop in any conditions.
That’s where this book helps; right from the beginning, from the seeds. Have you ever bought a pack of seeds, excitedly sown them, and then had a germination rate of zero or something close to that (this reviewer has)?
Alice Mirren takes us on a tour of how to save seeds from plants you know are regionally viable (not the product of some vast globalized industry that doesn’t know you live in an ancient bog with a cold south-east wind blowing in from Siberia), and then how to care for and curate them, how to store them for future years, how to keep a self-perpetuating seed bank.
She goes beyond that, though. Regular 10almonds readers might remember about the supercentenarian “Blue Zones”, and how big factors in healthy longevity include community and purpose; Mirren advocates for organizing community seed banks, which will also mean that everyone (including you) has access to much more diverse seeds, and when it comes to the perils of natural selection, diversity means survival. Otherwise, if you have just one seed type, a single blight can wipe out everything pretty much overnight.
Bottom line: if you grow your own food or would like to, this is a “bible of…” level book that you absolutely should have to hand.
Click here to check out Seed Saving Secrets, and see the results in your kitchen and on your plate!
Share This Post

Related Posts
-
Paracetamol pack sizes and availability are changing. Here’s what you need to know
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Changes are coming into effect from February 1 about how paracetamol is sold in Australia.
This mainly affects pack sizes of paracetamol sold outside pharmacies and how paracetamol is accessed in pharmacies.
The changes, announced by Australia’s drug regulator, are in line with moves internationally to reduce the harms of liver toxicity and the risk of overdose.
However, there are no new safety concerns when paracetamol is used as directed. And children’s products are not affected.

Bowonpat Sakaew/Shutterstock What is paracetamol?
Paracetamol is commonly sold under brand names such as Panadol, Dymadon and Panamax. It’s used to treat mild pain and fever for short periods or can be prescribed for chronic (long-term) pain.
Millions of packs of this cheap and accessible medicine are sold in Australia every year.
Small packs (up to 20 tablets) have been available from supermarkets and other retailers such as petrol stations. Larger packs (up to 100 tablets) are only available from pharmacies.
Paracetamol is relatively safe when used as directed. However, at higher-than-recommended doses, it can cause liver toxicity. In severe cases and when left untreated, this can be lethal.
Why are the rules changing?
In 2022, we wrote about how the Therapeutic Goods Administration (TGA) was considering changes to paracetamol access because of an increase in people going to hospital with paracetamol poisoning.
An expert review it commissioned found there were about 40–50 deaths every year from paracetamol poisoning between 2007 and 2020. Between 2009–10 and 2016–17, hospital admissions for this increased (from 8,617 to 11,697), before reducing in 2019–20 (8,723). Most admissions were due to intentional self-poisonings, and about half of these were among people aged ten to 24.
After the report, the TGA consulted with the public to work out how to prevent paracetamol poisonings.
Options included reducing pack sizes, limiting how many packs could be bought at once, moving larger packs behind the pharmacy counter and restricting access by age.
Responses were mixed. Although responses supported the need to prevent poisonings, there were concerns about how changes might affect:
- people with chronic pain, especially those in regional areas, where it may be harder to access pharmacies and, therefore, larger packs
- people on limited incomes, if certain products were made prescription-only.
Although deaths from paracetamol poisoning are tragic and preventable, they are rare considering how much paracetamol Australians use. There is less than one death due to poisoning for every million packs sold.
Because of this, it was important the TGA addressed concerns about poisonings while making sure Australians still had easy access to this essential medicine.
If you buy large packs of paracetamol for chronic pain, you’ll need to go to the pharmacy counter. StratfordProductions/Shutterstock So what’s changing?
The key changes being introduced relate to new rules about the pack sizes that can be sold outside pharmacies, and the location of products sold in pharmacies.
From February 1, packs sold in supermarkets and places other than pharmacies will reduce from a maximum 20 tablets to 16 tablets per pack. These changes bring Australia in line with other countries. These include the United Kingdom, which restricted supermarket packs to 16 tablets in 1998, and saw reductions in poisonings.
In all jurisdictions except Queensland and Western Australia, packs sold in pharmacies larger than 50 tablets will move behind the pharmacy counter and can only be sold under pharmacist supervision. In Queensland and WA, products containing more than 16 tablets will only be available from behind the pharmacy counter and sold under pharmacist supervision.
In all jurisdictions, any packs containing more than 50 tablets will need to be sold in blister packs, rather than bottles.
Several paracetamol products are not affected by these changes. These include children’s products, slow-release formulations (for example, “osteo” products), and products already behind the pharmacy counter or only available via prescription.
What else do I need to know?
These changes have been introduced to reduce the risk of poisonings from people exceeding recommended doses. The overall safety profile of paracetamol has not changed.
Paracetamol is still available from all current locations and there are no plans to make it prescription-only or remove it from supermarkets altogether. Many companies have already been updating their packaging to ensure there are no gaps in supply.
The reduction in pack sizes of paracetamol available in supermarkets means a pack of 16 tablets will now last two days instead of two-and-a-half days if taken at the maximum dose (two tablets, four times a day). Anyone in pain that does not improve after short-term use should speak to their pharmacist or GP.
For people who use paracetamol regularly for chronic pain, it is more cost-effective to continue buying larger packs from pharmacies. As larger packs (50+ tablets) need to be kept out of sight, you will need to ask at the pharmacy counter. Pharmacists know that for many people it’s appropriate to use paracetamol daily for chronic pain.
Natasa Gisev, Clinical pharmacist and Scientia Associate Professor at the National Drug and Alcohol Research Centre, UNSW Sydney and Ria Hopkins, Postdoctoral Research Fellow, National Drug and Alcohol Research Centre, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Great Cholesterol Myth, Revised and Expanded – by Dr. Jonny Bowden and Dr. Stephen Sinatra
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The topic of cholesterol, and saturated fat for that matter, is a complex and often controversial one. How does this book treat it?
With strong opinions, is how—but backed by good science. The authors, a nutritionist and a cardiologist, pull no punches about outdated and/or cherry-picked science, and instead make the case for looking at what, statistically speaking, appear to be the real strongest risk factors.
So, are they advocating for Dave Asprey-style butter-guzzling, or “the carnivore diet”? No, no they are not. Those things remain unhealthy, even if they give some short-term gains (of energy levels, weight loss, etc).
They do advocate, however, for enjoying saturated fats in moderation, and instead of certain polyunsaturated seed oils that do far worse. They also advocate strongly for avoiding sugar, stress, and (for different reasons) statins (in most people’s cases).
They also demystify in clear terms, and often with diagrams and infographics, the various kinds of fats and their components, broken down in far more detail than any other pop-science source this reviewer has seen.
Bottom line: if you want to take a scientific approach to heart health, this book can help you to focus on what will actually make the biggest difference.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cannabis Myths vs Reality
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cannabis Myths vs Reality

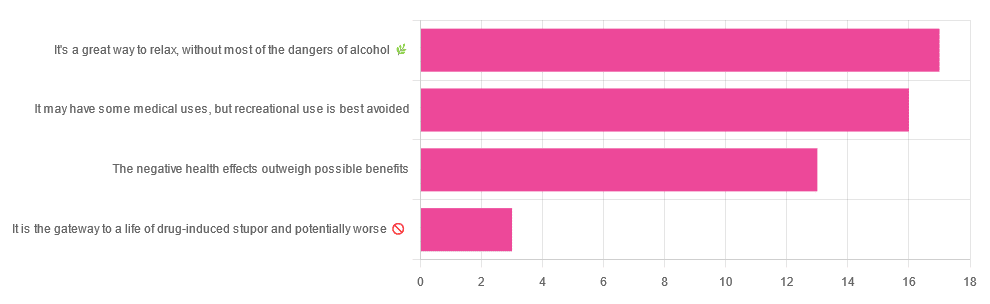
We asked you for your (health-related) opinion on cannabis use—specifically, the kind with psychoactive THC, not just CBD. We got the above-pictured, below-described, spread of responses:
- A little over a third of you voted for “It’s a great way to relax, without most of the dangers of alcohol”.
- A little under a third of you voted for “It may have some medical uses, but recreational use is best avoided”.
- About a quarter of you voted for “The negative health effects outweigh the possible benefits”
- Three of you voted for “It is the gateway to a life of drug-induced stupor and potentially worse”
So, what does the science say?
A quick legal note first: we’re a health science publication, and are writing from that perspective. We do not know your location, much less your local laws and regulations, and so cannot comment on such. Please check your own local laws and regulations in that regard.
Cannabis use can cause serious health problems: True or False?
True. Whether the risks outweigh the benefits is a personal and subjective matter (for example, a person using it to mitigate the pain of late stage cancer is probably unconcerned with many other potential risks), but what’s objectively true is that it can cause serious health problems.
One subscriber who voted for “The negative health effects outweigh the possible benefits” wrote:
❝At a bare minimum, you are ingesting SMOKE into your lungs!! Everyone SEEMS TO BE against smoking cigarettes, but cannabis smoking is OK?? Lung cancer comes in many forms.❞
Of course, that is assuming smoking cannabis, and not consuming it as an edible. But, what does the science say on smoking it, and lung cancer?
There’s a lot less research about this when it comes to cannabis, compared to tobacco. But, there is some:
❝Results from our pooled analyses provide little evidence for an increased risk of lung cancer among habitual or long-term cannabis smokers, although the possibility of potential adverse effect for heavy consumption cannot be excluded.❞
Read: Cannabis smoking and lung cancer risk: Pooled analysis in the International Lung Cancer Consortium
Another study agreed there appears to be no association with lung cancer, but that there are other lung diseases to consider, such as bronchitis and COPD:
❝Smoking cannabis is associated with symptoms of chronic bronchitis, and there may be a modest association with the development of chronic obstructive pulmonary disease. Current evidence does not suggest an association with lung cancer.❞
Read: Cannabis Use, Lung Cancer, and Related Issues
Cannabis edibles are much safer than smoking cannabis: True or False?
Broadly True, with an important caveat.
One subscriber who selected “It may have some medical uses, but recreational use is best avoided”, wrote:
❝I’ve been taking cannabis gummies for fibromyalgia. I don’t know if they’re helping but they’re not doing any harm. You cannot overdose you don’t become addicted.❞
Firstly, of course consuming edibles (rather than inhaling cannabis) eliminates the smoke-related risk factors we discussed above. However, other risks remain, including the much greater ease of accidentally overdosing.
❝Visits attributable to inhaled cannabis are more frequent than those attributable to edible cannabis, although the latter is associated with more acute psychiatric visits and more ED visits than expected.❞
Note: that “more frequent” for inhaled cannabis, is because more people inhale it than eat it. If we adjust the numbers to control for how much less often people eat it, suddenly we see that the numbers of hospital admissions are disproportionately high for edibles, compared to inhaled cannabis.
Or, as the study author put it:
❝There are more adverse drug events associated on a milligram per milligram basis of THC when it comes in form of edibles versus an inhaled cannabis. If 1,000 people smoked pot and 1,000 people at the same dose in an edible, then more people would have more adverse drug events from edible cannabis.❞
See the numbers: Acute Illness Associated With Cannabis Use, by Route of Exposure
Why does this happen?
- It’s often because edibles take longer to take effect, so someone thinks “this isn’t very strong” and has more.
- It’s also sometimes because someone errantly eats someone else’s edibles, not realising what they are.
- It’s sometimes a combination of the above problems: a person who is now high, may simply forget and/or make a bad decision when it comes to eating more.
On the other hand, that doesn’t mean inhaling it is necessarily safer. As well as the pulmonary issues we discussed previously, inhaling cannabis has a higher risk of cannabinoid hyperemesis syndrome (and the resultant cyclic vomiting that’s difficult to treat).
You can read about this fascinating condition that’s sometimes informally called “scromiting”, a portmanteau of screaming and vomiting:
Cannabinoid Hyperemesis Syndrome
You can’t get addicted to cannabis: True or False?
False. However, it is fair to say that the likelihood of developing a substance abuse disorder is lower than for alcohol, and much lower than for nicotine.
See: Prevalence of Marijuana Use Disorders in the United States Between 2001–2002 and 2012–2013
If you prefer just the stats without the science, here’s the CDC’s rendering of that:
Addiction (Marijuana or Cannabis Use Disorder)
However, there is an interesting complicating factor, which is age. One is 4–7 times more likely to develop a substance abuse disorder, if one starts use as an adolescent, rather than later in life:
Cannabis is the gateway to use of more dangerous drugs: True or False?
False, generally speaking. Of course, for any population there will be some outliers, but there appears to be no meaningful causal relation between cannabis use and other substance use:
Interestingly, the strongest association (where any existed at all) was between cannabis use and opioid use. However, rather than this being a matter of cannabis use being a gateway to opioid use, it seems more likely that this is a matter of people looking to both for the same purpose: pain relief.
As a result, growing accessibility of cannabis may actually reduce opioid problems:
- Cannabis as a Gateway Drug for Opioid Use Disorder
- Association between medical cannabis laws and opioid overdose mortality has reversed over time
Some final words…
Cannabis is a complex drug with complex mechanisms and complex health considerations, and research is mostly quite young, due to its historic illegality seriously cramping science by reducing sample sizes to negligible. Simply put, there’s a lot we still don’t know.
Also, we covered some important topics today, but there were others we didn’t have time to cover, such as the other potential psychological benefits—and risks. Likely we’ll revisit those another day.
Lastly, while we’ve covered a bunch of risks today, those of you who said it has fewer and lesser risks than alcohol are quite right—the only reason we couldn’t focus on that more, is because to talk about all the risks of alcohol would make this feature many times longer!
Meanwhile, whether you partake or not, stay safe and stay well.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: