The Recipe For Empowered Leadership – by Doug Meyer-Cuno
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is not a “here’s how to become a leader, you young would-be Machiavelli”; it’s more a “so you’re in a leadership role; now what?” book. The book’s subtitle describes well its contents: “25 Ingredients For Creating Value & Empowering Others”
The book is written with the voice of experience, but without the ego-driven padding that accompanies many such books. Especially: any anecdotal illustrations are short and to-the-point, no chapter-long diversions here.
Which we love!
Equally helpful is where the author does spend a little more time and energy: on the “down to brass tacks” of how exactly to do various things.
In short: if instead of a lofty-minded book of vague idealized notions selling a pipedream, you’d rather have a manual of how to actually be a good leader when it comes down to it, this is the book for you.
Pick Up The Recipe For Empowered Leadership On Amazon Today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Paulina Porizkova (Former Supermodel) Talks Menopause, Aging, & Appearances

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Are supermodels destined to all eventually become “Grizabella the Glamor Cat”, a washed-up shell of their former glory? Is it true that “men grow cold as girls grow old, and we all lose our charms in the end”? And what—if anything—can we do about it?
Insights from a retired professional
Paulina Porizkova is 56, and she looks like she’s… 56, maybe? Perhaps a little younger or a bit older depending on the camera and lighting and such.
It’s usually the case, on glossy magazine covers and YouTube thumbnails, that there’s a 20-year difference between appearance and reality, but not here. Why’s that?
Porizkova noted that many celebrities of a similar age look younger, and felt bad. But then she noted that they’d all had various cosmetic work done, and looked for images of “real” women in their mid-50s, and didn’t find them.
Note: we at 10almonds do disagree with one thing here: we say that someone who has had cosmetic work done is no less real for it; it’s a simple matter of personal choice and bodily autonomy. She is, in our opinion, making the same mistake as people make when they say such things as “real people, rather than models”, as though models are not also real people.
Porizkova found modelling highly lucrative but dehumanizing, and did not enjoy the objectification involved—and she enjoyed even less, when she reached a certain age, negative comments about aging, and people being visibly wrong-footed when meeting her, as they had misconceptions based on past images.
As a child and younger adult through her modelling career, she felt very much “seen and not heard”, and these days, she realizes she’s more interesting now but feels less seen. Menopause coincided with her marriage ending, and she felt unattractive and ignored by her husband; she questioned her self-worth, and felt very bad about it. Then her husband (they had separated, but had not divorced) died, and she felt even more isolated—but it heightened her sensitivity to life.
In her pain and longing for recognition, she reached out through her Instagram, crying, and received positive feedback—but still she struggles with expressing needs and feeling worthy.
And yet, when it comes to looks, she embraces her wrinkles as a form of expression, and values her natural appearance over cosmetic alterations.
She describes herself as a work in progress—still broken, still needing cleansing and healing, but proud of how far she’s come so far, and optimistic with regard to the future.
For all this and more in her own words, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The Many Faces Of Cosmetic Surgery
Take care!
Share This Post
-

Will there soon be a cure for HIV?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Human immunodeficiency virus, or HIV, is a chronic health condition that can be fatal without treatment. People with HIV can live healthy lives by taking antiretroviral therapy (ART), but this medication must be taken daily in order to work, and treatment can be costly. Fortunately, researchers believe a cure is possible.
In July, a seventh person was reportedly cured of HIV following a 2015 stem cell transplant for acute myeloid leukemia. The patient stopped taking ART in 2018 and has remained in remission from HIV.
Read on to learn more about HIV, the promise of stem cell transplants, and what other potential cures are on the horizon.
What is HIV?
HIV infects and destroys the immune system’s cells, making people more susceptible to infections. If left untreated, HIV will severely impair the immune system and progress to acquired immunodeficiency syndrome (AIDS). People living with untreated AIDS typically die within three years.
People with HIV can take ART to help their immune systems recover and to reduce their viral load to an undetectable level, which slows the progression of the disease and prevents them passing the virus to others.
How can stem cell transplants cure HIV?
Several people have been cured of HIV after receiving stem cell transplants to treat leukemia or lymphoma. Stem cells are produced by the spongy tissue located in the center of some bones, and they can turn into new blood cells.
A mutation on the CCR5 gene prevents HIV from infecting new cells and creates resistance to the virus, which is why some HIV-positive people have received stem cells from donors carrying this mutation. (One person was reportedly cured of HIV after receiving stem cells without the CCR5 mutation, but further research is needed to understand how this occurred.)
Despite this promising news, experts warn that stem cell transplants can be fatal, so it’s unlikely this treatment will be available to treat people with HIV unless a stem cell transplant is needed to treat cancer. People with HIV are at an increased risk for blood cancers, such as Hodgkin lymphoma and non-Hodgkin lymphoma, which stem cell transplants can treat.
Additionally, finding compatible donors with the CCR5 mutation who share genetic heritage with patients of color can be challenging, as donors with the mutation are typically white.
What are other potential cures for HIV?
In some rare cases, people who started ART shortly after infection and later stopped treatment have maintained undetectable levels of HIV in their bodies. There have also been some people whose bodies have been able to maintain low viral loads without any ART at all.
Researchers are studying these cases in their search for a cure.
Other treatment options researchers are exploring include:
- Gene therapy: In addition to stem cell transplants, gene therapy for HIV involves removing genes from HIV particles in patients’ bodies to prevent the virus from infecting other cells.
- Immunotherapy: This treatment is typically used in cancer patients to teach their immune systems how to fight off cancer. Research has shown that giving some HIV patients antibodies that target the virus helps them reach undetectable levels of HIV without ART.
- mRNA technology: mRNA, a type of genetic material that helps produce proteins, has been used in vaccines to teach cells how to fight off viruses. Researchers are seeking a way to send mRNA to immune system cells that contain HIV.
When will there be a cure for HIV?
The United Nations and several countries have pledged to end HIV and AIDS by 2030, and a 2023 UNAIDS report affirmed that reaching this goal is possible. However, strategies to meet this goal include HIV prevention and improving access to existing treatment alongside the search for a cure, so we still don’t know when a cure might be available.
How can I find out if I have HIV?
You can get tested for HIV from your primary care provider or at your local health center. You can also purchase an at-home HIV test from a drugstore or online. If your at-home test result is positive, follow up with your health care provider to confirm the diagnosis and get treatment.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post
-
Reflexology: What The Science Says
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How Does Reflexology Work, Really?

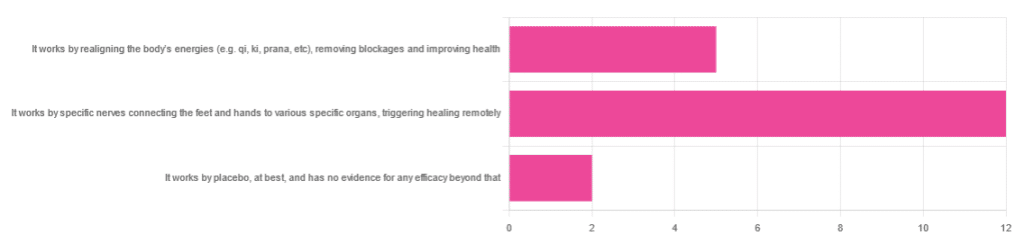
In Wednesday’s newsletter, we asked you for your opinion of reflexology, and got the above-depicted, below-described set of responses:
- About 63% said “It works by specific nerves connecting the feet and hands to various specific organs, triggering healing remotely”
- About 26% said “It works by realigning the body’s energies (e.g. qi, ki, prana, etc), removing blockages and improving health“
- About 11% said “It works by placebo, at best, and has no evidence for any efficacy beyond that”
So, what does the science say?
It works by realigning the body’s energies (e.g. qi, ki, prana, etc), removing blockages and improving health: True or False?
False, or since we can’t prove a negative: there is no reliable scientific evidence for this.
Further, there is no reliable scientific evidence for the existence of qi, ki, prana, soma, mana, or whatever we want to call it.
To save doubling up, we did discuss this in some more detail, exploring the notion of qi as bioelectrical energy, including a look at some unreliable clinical evidence for it (a study that used shoddy methodology, but it’s important to understand what they did wrong, to watch out for such), when we looked at [the legitimately very healthful practice of] qigong, a couple of weeks ago:
Qigong: A Breath Of Fresh Air?
As for reflexology specifically: in terms of blockages of qi causing disease (and thus being a putative therapeutic mechanism of action for attenuating disease), it’s an interesting hypothesis but in terms of scientific merit, it was pre-emptively supplanted by germ theory and other similarly observable-and-measurable phenomena.
We say “pre-emptively”, because despite orientalist marketing, unless we want to count some ancient pictures of people getting a foot massage and say it is reflexology, there is no record of reflexology being a thing before 1913 (and that was in the US, by a laryngologist working with a spiritualist to produce a book that they published in 1917).
It works by specific nerves connecting the feet and hands to various specific organs, triggering healing remotely: True or False?
False, or since we can’t prove a negative: there is no reliable scientific evidence for this.
A very large independent review of available scientific literature found the current medical consensus on reflexology is that:
- Reflexology is effective for: anxiety (but short lasting), edema, mild insomnia, quality of sleep, and relieving pain (short term: 2–3 hours)
- Reflexology is not effective for: inflammatory bowel disease, fertility treatment, neuropathy and polyneuropathy, acute low back pain, sub acute low back pain, chronic low back pain, radicular pain syndromes (including sciatica), post-operative low back pain, spinal stenosis, spinal fractures, sacroiliitis, spondylolisthesis, complex regional pain syndrome, trigger points / myofascial pain, chronic persistent pain, chronic low back pain, depression, work related injuries of the hip and pelvis
Source: Reflexology – a scientific literary review compilation
(the above is a fascinating read, by the way, and its 50 pages go into a lot more detail than we have room to here)
Now, those items that they found it effective for, looks suspiciously like a short list of things that placebo is often good for, and/or any relaxing activity.
Another review was not so generous:
❝The best evidence available to date does not demonstrate convincingly that reflexology is an effective treatment for any medical condition❞
~ Dr. Edzard Ernst (MD, PhD, FMedSci)
Source: Is reflexology an effective intervention? A systematic review of randomised controlled trials
In short, from the available scientific literature, we can surmise:
- Some researchers have found it to have some usefulness against chiefly psychosomatic conditions
- Other researchers have found the evidence for even that much to be uncompelling
It works by placebo, at best, and has no evidence for any efficacy beyond that: True or False?
Mostly True; of course reflexology runs into similar problems as acupuncture when it comes to testing against placebo:
How Does One Test Acupuncture Against Placebo Anyway?
…but not quite as bad, since it is easier to give a random foot massage while pretending it is a clinical treatment, than to fake putting needles into key locations.
However, as the paper we cited just above (in answer to the previous True/False question) shows, reflexology does not appear to meaningfully outperform placebo—which points to the possibility that it does work by placebo, and is just a placebo treatment on the high end of placebo (because the placebo effect is real, does work, isn’t “nothing”, and some placebos work better than others).
For more on the fascinating science and useful (applicable in daily life!) practicalities of how placebo does work, check out:
How To Leverage Placebo Effect For Yourself
Take care!
Share This Post

Related Posts
-

Inheritance – by Dr. Sharon Moalem
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We know genes make a big difference to a lot about us, but how much? And, the genes we have, we’re stuck with, right?
Dr. Sharon Moalem shines a bright light into some of the often-shadowier nooks and crannies of our genetics, covering such topics as:
- How much can (and can’t) be predicted from our parents’ genes—even when it comes to genetic traits that both parents have, and Gregor Mendel himself would (incorrectly) think obvious
- How even something so seemingly simple and clear as genetic sex, very definitely isn’t
- How traumatic life events can cause epigenetic changes that will scar us for generations to come
- How we can use our genetic information to look after our health much better
- How our life choices can work with, or overcome, the hand we got dealt in terms of genes
The style of the book is conversational, down to how there’s a lot of “I” and “you” in here, and the casual style belies the heavy, sharp, up-to-date science contained within.
Bottom line: if you’d like insight into the weird and wonderful nuances of genetics as found in this real, messy, perfectly chaotic world, this book is an excellent choice.
Click here to check out Inheritance, and learn more about yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Three Critical Kitchen Prescriptions
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Three Critical Kitchen Prescriptions

This is Dr. Saliha Mahmood-Ahmed. She’s a medical doctor—specifically, a gastroenterologist. She’s also a chef, and winner of the BBC’s MasterChef competition. So, from her gastroenterology day-job and her culinary calling, she has some expert insights to share on eating well!
❝Food and medicine are inextricably linked to one another, and it is an honour to be a doctor who specialises in digestive health and can both cook, and teach others to cook❞
~ Dr. Saliha Mahmood-Ahmed, after winning MasterChef and being asked if she’d quit medicine to be a full-time chef
Dr. Mahmood-Ahmed’s 3 “Kitchen Prescriptions”
They are:
- Cook, cook, cook
- Feed your gut bugs
- Do not diet
Let’s take a look at each of those…
Cook, cook, cook
We’re the only species on Earth that cooks food. An easy knee-jerk response might be to think maybe we shouldn’t, then, but… We’ve been doing it for at least 30,000 years, which is about 1,500 generations, while a mere 100 generations is generally sufficient for small evolutionary changes. So, we’ve evolved this way now.
More importantly in this context: we, ourselves, should cook our own food, at least per household.
Not ready meals; we haven’t evolved for those (yet! Give it another few hundred generations maybe)
Feed your gut bugs
The friendly ones. Enjoy prebiotics, probiotics, and plenty of fiber—and then be mindful of what else you do or don’t eat. Feeding the friendly bacteria while starving the unfriendly ones may seem like a tricky task, but it actually can be quite easily understood and implemented. We did a main feature about this a few weeks ago:
Making Friends With Your Gut (You Can Thank Us Later)
Do not diet
Dr. Mahmood-Ahmed is a strong critic of calorie-counting as a weight-loss strategy:
Rather than focusing on the number of calories consumed, try focusing on introducing enough variety of food into your daily diet, and on fostering good microbial diversity within your gut.
It’s a conceptual shift from restrictive weight loss, to prescriptive adding of things to one’s diet, with fostering diversity of microbiota as a top priority.
This, too, she recommends be undertaken gently, though—making small, piecemeal, but sustainable improvements. Nobody can reasonably incorporate, say, 30 new fruits and vegetables into one’s diet in a week; it’s unrealistic, and more importantly, it’s unsustainable.
Instead, consider just adding one new fruit or vegetable per shopping trip!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Is chocolate milk a good recovery drink after a workout? A dietitian reviews the evidence
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Whether you enjoy chocolate milk regularly, as a weekend treat, or as an occasional dose of childhood nostalgia, it probably wouldn’t be the first option you think of for post-workout recovery.
Unless you’re on TikTok, perhaps. According to many people on the social media platform, chocolate milk is not only delicious, but it offers benefits comparable to sports drinks after a workout.
So is there any evidence to support this? Let’s take a look.

eldar nurkovic/Shutterstock Rehydrating after a workout is important
Water accounts for somewhere between 50% and 60% of our body weight. Water has many important functions in the body, including helping to keep our body at the right temperature through sweating.
We lose water naturally from our bodies when we sweat, as well as through our breathing and when we go to the toilet. So it’s important to stay hydrated to replenish the water we lose.
When we don’t, we become dehydrated, which can put a strain on our bodies. Signs and symptoms of dehydration can range from thirst and dizziness to low blood pressure and confusion.
Athletes, because of their higher levels of exertion, lose more water through sweating and from respiration (when their breathing rate gets faster). If they’re training or competing in hot or humid environments they will sweat even more.
Dehydration impacts athletes’ performance and like for all of us, can affect their health.
So finding ways to ensure athletes rehydrate quickly during and after they train or compete is important. Fortunately, sports scientists and dietitians have done research looking at the composition of different fluids to understand which ones rehydrate athletes most effectively.
The beverage hydration index
The best hydrating drinks are those the body retains the most of once they’ve been consumed. By doing studies where they give people different drinks in standardised conditions, scientists have been able to determine how various options stack up.
To this end, they’ve developed something called the beverage hydration index, which measures to what degree different fluids hydrate a person compared to still water.
According to this index beverages with similar fluid retention to still water include sparkling water, sports drinks, cola, diet cola, tea, coffee, and beer below 4% alcohol. That said, alcohol is probably best avoided when recovering from exercise.
Beverages with superior fluid retention to still water include milk (both full-fat and skim), soy milk, orange juice and oral rehydration solutions.
This body of research indicates that when it comes to rehydration after exercise, unflavoured milk (full fat, skim or soy) is better than sports drinks.
But what about chocolate milk?
A small study looked at the effects of chocolate milk compared to plain milk on rehydration and exercise performance in futsal players (futsal is similar to soccer but played on a court indoors). The researchers found no difference in rehydration between the two. There’s no other published research to my knowledge looking at how chocolate milk compares to regular milk for rehydration during or after exercise.
But rehydration isn’t the only thing athletes look for in sports drinks. In the same study, drinking chocolate milk after play (referred to as the recovery period) increased the time it took for the futsal players to become exhausted in further exercise (a shuttle run test) four hours later.
This was also shown in a review of several clinical trials. The analysis found that, compared to different placebos (such as water) or other drinks containing fat, protein and carbohydrates, chocolate milk lengthened the time to exhaustion during exercise.
What’s in chocolate milk?
Milk contains protein, carbohydrates and electrolytes, each of which can affect hydration, performance, or both.
Protein is important for building muscle, which is beneficial for performance. The electrolytes in milk (including sodium and potassium) help to replace electrolytes lost through sweating, so can also be good for performance, and aid hydration.
Compared to regular milk, chocolate milk contains added sugar. This provides extra carbohydrates, which are likewise beneficial for performance. Carbohydrates provide an immediate source of energy for athletes’ working muscles, where they’re stored as glycogen. This might contribute to the edge chocolate milk appears to have over plain milk in terms of athletic endurance.
The added sugar in chocolate milk provides extra carbohydrates. Brent Hofacker/Shutterstock Coffee-flavoured milk has an additional advantage. It contains caffeine, which can improve athletic performance by reducing the perceived effort that goes into exercise.
One study showed that a frappe-type drink prepared with filtered coffee, skim milk and sugar led to better muscle glycogen levels after exercise compared to plain milk with an equivalent amount of sugar added.
So what’s the verdict?
Evidence shows chocolate milk can rehydrate better than water or sports drinks after exercise. But there isn’t evidence to suggest it can rehydrate better than plain milk. Chocolate milk does appear to improve athletic endurance compared to plain milk though.
Ultimately, the best drink for athletes to consume to rehydrate is the one they’re most likely to drink.
While many TikTok trends are not based on evidence, it seems chocolate milk could actually be a good option for recovery from exercise. And it will be cheaper than specialised sports nutrition products. You can buy different brands from the supermarket or make your own at home with a drinking chocolate powder.
This doesn’t mean everyone should look to chocolate milk when they’re feeling thirsty. Chocolate milk does have more calories than plain milk and many other drinks because of the added sugar. For most of us, chocolate milk may be best enjoyed as an occasional treat.
Evangeline Mantzioris, Program Director of Nutrition and Food Sciences, Accredited Practising Dietitian, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: