The Magic of L-theanine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
All The Benefits Of Caffeine And More, Without The Drawbacks? What’s The Catch?
It just takes one extra supplement.
For many of us, our morning brew is practically a ritual, but caffeine can also cause all kinds of problems ranging from caffeine jitters to caffeine crashes to caffeine addiction and withdrawal. Surely, something could be better?
Well, yes it could! You doubtlessly know about green tea’s antioxidant properties, but its amino acid, l-theanine (which can be taken as a supplement with coffee, if you don’t enjoy green tea) has so much more to offer:
- L-theanine has been found to reduce stress responses—and let’s face it, when we most want/need a coffee is often when facing stress
- It also reduces anxiety, making it a very safe “downer” without the problems of, for example, alcohol—or other potentially addictive substances
- It’s far more than just that, though! Paradoxically, l-theanine also improves alertness (what other calming things promote alertness? Not so many)
- Part of its trick is that it also improves accuracy—whereas stimulants like caffeine may produce a twitchy, jumpy, responsiveness, l-theanine’s signature effect is a calm state of sharp readiness. Caffeine works by stimulating the adrenal gland and increasing blood pressure, while simultaneously blocking adenosine receptors so that your body doesn’t notice its own tiredness—which is why you’re likely to crash later, when the tiredness that had been masked, all hits at once. Instead, l-theanine taken with caffeine acts as a moderator of that, making for a longer, gentler curve. In terms of subjective experience, what this can mean for many people is: no more caffeine jitters!
- All this means that while l-theanine can boost all kinds of cognitive function, including alertness and accuracy, many like to take in the evening as it can also promote a good night’s sleep, ready to be at your best the next day.
- How much to take? 200mg is a commonly used dosage, which in supplement terms is usually a single capsule. A lot easier to take than the 40 cups of green tea that this dosage would otherwise be!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Can you get sunburnt or UV skin damage through car or home windows?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When you’re in a car, train or bus, do you choose a seat to avoid being in the sun or do you like the sunny side?
You can definitely feel the sun’s heat through a window. But can you get sunburn or skin damage when in your car or inside with the windows closed?
Let’s look at how much UV (ultraviolet) radiation passes through different types of glass, how tinting can help block UV, and whether we need sunscreen when driving or indoors.

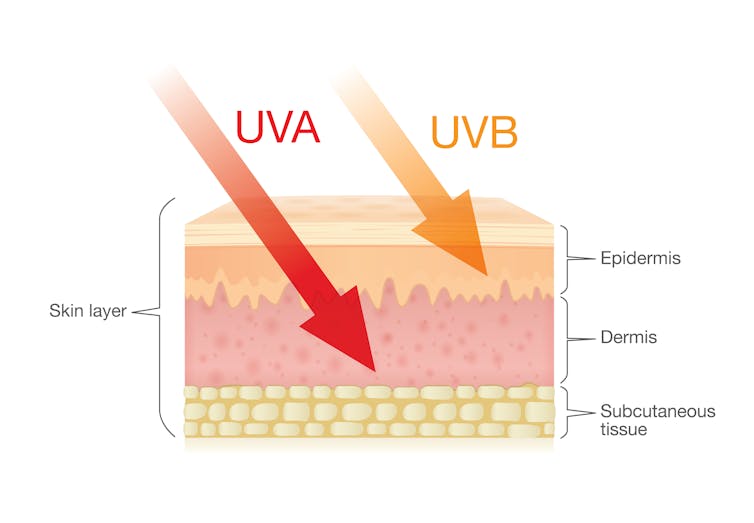
Zac Harris/Unsplash What’s the difference between UVA and UVB?
Of the total UV radiation that reaches Earth, about 95% is UVA and 5% is UVB.
UVB only reaches the upper layers of our skin but is the major cause of sunburn, cataracts and skin cancer.
UVA penetrates deeper into our skin and causes cell damage that leads to skin cancer.
UVA penetrates deeper than UVB. Shutterstock/solar22 Glass blocks UVA and UVB radiation differently
All glass used in house, office and car windows completely blocks UVB from passing through.
But only laminated glass can completely block UVA. UVA can pass through other glass used in car, house and office windows and cause skin damage, increasing the risk of cancer.
Car windscreens block UVA, but the side and rear windows don’t
A car’s front windscreen lets in lots of sunshine and light. Luckily it blocks 98% of UVA radiation because it is made of two layers of laminated glass.
But the side and rear car windows are made of tempered glass, which doesn’t completely block UVA. A study of 29 cars found a range from 4% to almost 56% of UVA passed through the side and rear windows.
The UVA protection was not related to the car’s age or cost, but to the type of glass, its colour and whether it has been tinted or coated in a protective film. Grey or bronze coloured glass, and window tinting, all increase UVA protection. Window tinting blocks around 95% of UVA radiation.
In a separate study from Saudi Arabia, researchers fitted drivers with a wearable radiation monitor. They found drivers were exposed to UV index ratings up to 3.5. (In Australia, sun protection is generally recommended when the UV index is 3 or above – at this level it takes pale skin about 20 minutes to burn.)
So if you have your windows tinted, you should not have to wear sunscreen in the car. But without tinted windows, you can accumulate skin damage.
UV exposure while driving increases skin cancer risk
Many people spend a lot of time in the car – for work, commuting, holiday travel and general transport. Repeated UVA radiation exposure through car side windows might go unnoticed, but it can affect our skin.
Indeed, skin cancer is more common on the driver’s side of the body. A study in the United States (where drivers sit on the left side) found more skin cancers on the left than the right side for the face, scalp, arm and leg, including 20 times more for the arm.
Another US study found this effect was higher in men. For melanoma in situ, an early form of melanoma, 74% of these cancers were on the on the left versus 26% on the right.
Earlier Australian studies reported more skin damage and more skin cancer on the right side.
Cataracts and other eye damage are also more common on the driver’s side of the body.
What about UV exposure through home or office windows?
We see UV damage from sunlight through our home windows in faded materials, furniture or plastics.
Most glass used in residential windows lets a lot of UVA pass through, between 45 and 75%.
Residential windows can let varied amounts of UVA through. Sherman Trotz/Pexels Single-pane glass lets through the most UVA, while thicker, tinted or coated glass blocks more UVA.
The best options are laminated glass, or double-glazed, tinted windows that allow less than 1% of UVA through.
Skylights are made from laminated glass, which completely stops UVA from passing through.
Most office and commercial window glass has better UVA protection than residential windows, allowing less than 25% of UVA transmission. These windows are usually double-glazed and tinted, with reflective properties or UV-absorbent chemicals.
Some smart windows that reduce heat using chemical treatments to darken the glass can also block UVA.
So when should you wear sunscreen and sunglasses?
The biggest risk with skin damage while driving is having the windows down or your arm out the window in direct sun. Even untinted windows will reduce UVA exposure to some extent, so it’s better to have the car window up.
For home windows, window films or tint can increase UVA protection of single pane glass. UVA blocking by glass is similar to protection by sunscreen.
When you need to use sunscreen depends on your skin type, latitude and time of the year. In a car without tinted windows, you could burn after one hour in the middle of the day in summer, and two hours in the middle of a winter’s day.
But in the middle of the day next to a home window that allows more UVA to pass through, it could take only 30 minutes to burn in summer and one hour in winter.
When the UV index is above three, it is recommended you wear protective sunglasses while driving or next to a sunny window to avoid eye damage.
Theresa Larkin, Associate Professor of Medical Sciences, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Fasting Without Crashing?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Intermittent Fasting: What’s the truth?
Before we get to facts and fictions, let’s quickly cover:
What is Intermittent Fasting?
Intermittent Fasting (IF) is an umbrella term for various kinds of time-restricted fasting, based on a schedule. Types include:
Time-restricted IF, for example:
- 16:8—Fast for 16 hours, eat during an 8-hour window
- 18:6–Fast for 18 hours, eat during a 6-hour window
- 20:4—Fast for 20 hours, eat during a 4-hour window
24hr fasting, including:
- Eat Stop Eat—basically, take a day off from eating once a week
- Alternate Day Fasting—a more extreme version of the above; it is what it sounds like; eat one day, fast the next, repeat
Non-fast fasting, e.g:
- 5:2—Eat normally for 5 days, have a very reduced calorie intake (⅓ of normal intake) for the other 2 days
- Fruit Fasting—have a small amount of fruit on “fast” days, but no other food
- The Warrior Diet—as above, but include a small amount of non-starchy vegetables
Why IF?
While IF is perhaps most commonly undertaken as a means of fat loss or fat management (i.e., keeping fat down when it is already low), others cite different reasons, such as short term cognitive performance or long-term longevity.
But… Does it work?
Here we get into the myth-busting bit!
“IF promotes weight loss”
Mix of True and False. It can! But it also doesn’t have to. If you’re a bodybuilder who downs 4,000 calories in your 4hr eating window, you’re probably not going to lose weight! For such people, this is of course “a feature, not a bug” of IF—especially as it has been found that, in an acute study, IF did not adversely impact muscle protein synthesis.
“IF promotes fat loss, without eating less”
Broadly True. IF was found to be potentially equal to, but not necessarily better than, eating less.
“IF provides metabolic benefits for general health”
Broadly True. IF (perhaps counterintuitively) decreases the risk of insulin resistance, and also has anti-inflammatory effects, benefits a healthy gut microbiome, and promotes healthy autophagy (which as we noted in a previous edition of 10almonds, is important against both aging and cancer)
However, results vary according to which protocol you’re observing…
For what it’s worth, 16:8 is perhaps the most-studied protocol. Because such studies tend to have the eating window from midday to 8pm, this means that—going against popular wisdom—part of the advice here is basically “skip breakfast”.
“Unlike caloric restriction, IF is sustainable and healthy as a long-term protocol”
Broadly True. Of course, there’s a slight loophole here in that IF is loosely defined—technically everyone fasts while they’re sleeping, at the very least!
However, for the most commonly-studied IF method (16:8), this is generally very sustainable and healthy and for most people.
On the other hand, a more extreme method such as Alternate Day Fasting, may be trickier to sustain (even if it remains healthy to do so), because it’s been found that hunger does not decrease on fasting days—ie, the body does not “get used to it”.
The American Journal of Clinical Nutrition wrote:
❝Alternate-day fasting was feasible in nonobese subjects, and fat oxidation increased. However, hunger on fasting days did not decrease, perhaps indicating the unlikelihood of continuing this diet for extended periods of time. Adding one small meal on a fasting day may make this approach to dietary restriction more acceptable.❞
“IF improves mood and cognition”
Mix of True and False (plus an honest “We Don’t Know” from researchers).
Many studies have found benefits to both mood and cognition, but in the short-term, fasting can make people “hangry” (or: “experience irritability due to low blood sugar levels”, as the scientists put it), and in the long term, it can worsen symptoms of depression for those who already experience such—although some studies have found it can help alleviate depressive symptoms.
Basically this is one where researchers typically append the words “more research is needed” to their summaries.
“Anyone can do IF”
Definitely False, unless going by the absolute broadest possible interpretation of what constitutes “Intermittent Fasting” to the point of disingenuity.
For example, if you are Type 1 Diabetic, and your blood sugars are hypo, and you wait until tomorrow to correct that, you will stand a good chance of going into a coma instead. So please don’t.
(On the other hand, IF may help achieve remission of type 2 diabetes)
Lastly, IF is broadly not recommend to children and adolescents, anyone pregnant or breastfeeding, and certain underlying health conditions not mentioned above (we’re not going to try to give an exhaustive list here, but basically, if you have a chronic health condition, we recommend you check with your doctor first).
WHICH APP?
Choosing a fasting app
Thinking of giving IF a try and would like a little extra help? We’ve got you covered!
Check out: Livewire’s 7 Best Intermittent Fasting Apps of 2023
Prefer to just trust us with a recommendation?
We like BodyFast—it’s #2 on Lifewire’s list, but it has an array of pre-set plans to choose from (unlike Lifewire’s #1, Zero), and plenty of clear tracking, scheduling help, and motivational features.
Both are available on both iOS and Android:
Share This Post
-
How To Reverse Skin Thinning
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Andrea Suarez makes it easy for us:
Not so thin-skinned after all
Skin thinning (skin atrophy) happens when both the outer layer (epidermis) and the deeper layer (dermis) become thinner, which makes your skin fragile, easier to bruise or tear, and slower to heal.
Collagen and elastin gradually decline after your 30s at a rate of about 1% per year, fibroblasts produce less structural protein, hyaluronic acid decreases so your skin holds less water, and sun-induced enzymes break down existing collagen.
How to slow or prevent skin thinning:
- Sun protection: daily broad-spectrum sunscreen, sun-protective clothing, and avoiding tanning beds reduce collagen-destroying UV exposure.
- Don’t smoke: smoking damages collagen production and accelerates dermal aging.
- Enjoy a balanced diet: sufficient protein, fruits, and vegetables support collagen formation and help avoid nutrient deficiencies that worsen skin fragility.
- Avoid unnecessary steroid use: long-term topical or systemic corticosteroids can cause skin atrophy if overused.
Treatments that can help reverse or improve thinning skin
- Topical retinoids: prescription retinoids such as tretinoin and tazarotene stimulate fibroblasts to produce collagen, reduce collagen-destroying enzymes, and increase epidermal cell turnover, which can gradually thicken skin.
- Hyaluronic acid: topical hyaluronic acid can improve hydration and elasticity, and studies using mid-size hyaluronic acid fragments showed improvements in skin thickness and fewer actinic purpura spots.
- Lactic acid (ammonium lactate): applying 12% ammonium lactate twice daily for several months can increase epidermal and dermal thickness while smoothing the skin.
Hormonal approaches to do both:
- DHEA creams or supplements: topical or oral dehydroepiandrosterone can increase oil production, hydration, and skin thickness in older adults.
- Estrogen therapy: bioidentical estradiol hormone replacement therapy can improve dermal thickness and collagen, amongst other markers of skin health.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Signs Of Low Estrogen In Women: What Your Skin, Hair, & Nails Are Trying To Tell You
Take care!
Share This Post



-
Spelt vs Bulgur – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing spelt to bulgur, we picked the spelt.
Why?
An argument could be made for bulgur, but we say spelt comes out on top. Speaking of “sorting the wheat from the chaff”, be aware: spelt is a hulled wheat product and bulgur is a cracked wheat product.
Looking at macros first, it’s not surprising therefore that spelt has proportionally more carbs and bulgur has proportionally more fiber, resulting in a slightly lower glycemic index. That said, for the exact same reason, spelt is proportionally higher in protein. Still, fiber is usually the most health-relevant aspect in the macros category, so we’re going to call this a moderate win for bulgur.
When it comes to micronutrients, however, spelt is doing a lot better:
In the category of vitamins, spelt is higher in vitamins A, B1, B2, B3, and E (with the difference in E being 26x more!), while bulgur is higher only in vitamin B9 (and that, only slightly). A clear win for spelt here.
Nor are the mineral contents less polarized; spelt has more copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while bulgur is not higher in any minerals. Another easy win for spelt.
Adding these up makes a win for spelt, but again we’d urge to not underestimate the importance of fiber. Enjoy both in moderation, unless you are avoiding wheat/gluten in which case don’t, and for almost everyone, mixed whole grains are always going to be best.
Want to learn more?
You might like to read:
- Grains: Bread Of Life, Or Cereal Killer?
- Gluten: What’s The Truth?
- Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fruit & Veg In The Fridge: Pros & Cons
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝What effect does refrigeration have on the nutritional value of fruit and vegetables??❞
It’s difficult to give a single definitive answer, because naturally there are a lot of different fruits and vegetables, and a lot of different climates. The answer may be different for tomatoes in Alaska vs bananas in Arizona!
However, we can still generalize at least somewhat
Refrigeration will generally slow down any degradation process, and in the case of fruit and vegetables, that can mean slowing down their “ripening” too, as applicable.
However…
Refrigeration will also impede helpful bioactivity too, and that includes quite a list of things.
Here’s a good study that’s quite illustrative; we’d summarize the conclusions but the rather long title already does that nicely:
So, this really is a case of “there are pros and cons, but probably more cons on balance”.
In practical terms, a good take-away from this can be twofold:
- don’t keep fruit and veg in the fridge unless the ambient temperature really requires it
- if the ambient temperature does require it, it’s best to get the produce in fresh each day if that’s feasible, to minimize time spent in the fridge
An extra thing not included there: often when it comes to the spoilage of fruit and veg, the problem is that it respires and oxidizes; reducing the temperature does lower the rate of those, but often a far better way is to remove the oxygen. So for example, if you get carried away and chop too many carrot batons for your hummus night, then putting them in a sealed container can go a long way to keeping them fresh.
See also: How Does the Nutritional Value of Fruits and Vegetables Change Over Time?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

With all this bird flu around, how safe are eggs, chicken or milk?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Enzo Palombo, Swinburne University of Technology
Recent outbreaks of bird flu – in US dairy herds, poultry farms in Australia and elsewhere, and isolated cases in humans – have raised the issue of food safety.
So can the virus transfer from infected farm animals to contaminate milk, meat or eggs? How likely is this?
And what do we need to think about to minimise our risk when shopping for or preparing food?
AS Foodstudio/Shutterstock How safe is milk?
Bird flu (or avian influenza) is a bird disease caused by specific types of influenza virus. But the virus can also infect cows. In the US, for instance, to date more than 80 dairy herds in at least nine states have been infected with the H5N1 version of the virus.
Investigations are under way to confirm how this happened. But we do know infected birds can shed the virus in their saliva, nasal secretions and faeces. So bird flu can potentially contaminate animal-derived food products during processing and manufacturing.
Indeed, fragments of bird flu genetic material (RNA) were found in cow’s milk from the dairy herds associated with infected US farmers.
However, the spread of bird flu among cattle, and possibly to humans, is likely to have been caused through contact with contaminated milking equipment, not the milk itself.
The test used to detect the virus in milk – which uses similar PCR technology to lab-based COVID tests – is also highly sensitive. This means it can detect very low levels of the bird flu RNA. But the test does not distinguish between live or inactivated virus, just that the RNA is present. So from this test alone, we cannot tell if the virus found in milk is infectious (and capable of infecting humans).
It’s best to stick with pasteurised milk. Amnixia/Shutterstock Does that mean milk is safe to drink and won’t transmit bird flu? Yes and no.
In Australia, where bird flu has not been reported in dairy cattle, the answer is yes. It is safe to drink milk and milk products made from Australian milk.
In the US, the answer depends on whether the milk is pasteurised. We know pasteurisation is a common and reliable method of destroying concerning microbes, including influenza virus. Like most viruses, influenza virus (including bird flu virus) is inactivated by heat.
Although there is little direct research on whether pasteurisation inactivates H5N1 in milk, we can extrapolate from what we know about heat inactivation of H5N1 in chicken and eggs.
So we can be confident there is no risk of bird flu transmission via pasteurised milk or milk products.
However, it’s another matter for unpasteurised or “raw” US milk or milk products. A recent study showed mice fed raw milk contaminated with bird flu developed signs of illness. So to be on the safe side, it would be advisable to avoid raw milk products.
How about chicken?
Bird flu has caused sporadic outbreaks in wild birds and domestic poultry worldwide, including in Australia. In recent weeks, there have been three reported outbreaks in Victorian poultry farms (two with H7N3 bird flu, one with H7N9). There has been one reported outbreak in Western Australia (H9N2).
The strains of bird flu identified in the Victorian and Western Australia outbreaks can cause human infection, although these are rare and typically result from close contact with infected live birds or contaminated environments.
Therefore, the chance of bird flu transmission in chicken meat is remote.
Nonetheless, it is timely to remind people to handle chicken meat with caution as many dangerous pathogens, such as Salmonella and Campylobacter, can be found on chicken carcasses.
Always handle chicken meat carefully when shopping, transporting it home and storing it in the kitchen. For instance, make sure no meat juices cross-contaminate other items, consider using a cool bag when transporting meat, and refrigerate or freeze the meat within two hours.
Avoid washing your chicken before cooking to prevent the spread of disease-causing microbes around the kitchen.
Finally, cook chicken thoroughly as viruses (including bird flu) cannot survive cooking temperatures.
Are eggs safe?
The recent Australian outbreaks have occurred in egg-laying or mixed poultry flocks, so concerns have been raised about bird flu transmission via contaminated chicken eggs.
Can flu viruses contaminate chicken eggs and potentially spread bird flu? It appears so. A report from 2007 said it was feasible for influenza viruses to enter through the eggshell. This is because influenza virus particles are smaller (100 nanometres) than the pores in eggshells (at least 200 nm).
So viruses could enter eggs and be protected from cleaning procedures designed to remove microbes from the egg surface.
Therefore, like the advice about milk and meat, cooking eggs is best.
The US Food and Drug Administration recommends cooking poultry, eggs and other animal products to the proper temperature and preventing cross-contamination between raw and cooked food.
In a nutshell
If you consume pasteurised milk products and thoroughly cook your chicken and eggs, there is nothing to worry about as bird flu is inactivated by heat.
The real fear is that the virus will evolve into highly pathogenic versions that can be transmitted from human to human.
That scenario is much more frightening than any potential spread though food.
Enzo Palombo, Professor of Microbiology, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: