The GLP-1 Lifestyle – by Dr. Joshua Hackett
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
While GLP-1 receptor agonists (i.e. semaglutide drugs such as Ozempic and Wegovy) have enjoyed the spotlight as a miracle cure (with some drawbacks), this book argues very reasonably that we should see them as a tool that we can use (or not) as part of a holistic approach to manage our metabolism.
Unusually, Dr. Hackett doesn’t argue strongly for one way or another, when it comes to using GLP-1 RAs. Rather, he makes the case that they indeed have pros and cons, and we should not only be aware of those pros and cons before making a decision either way, but also, we must understand the process of what goes on.
In contrast to the “inject it and forget it” marketing, he explains how if we actually understand what’s happening in our metabolism, we can improve things for ourselves and, at the very least, avoid sabotaging ourselves. Again, this knowledge is applicable with or without the drugs.
Much of the book is spent covering the physiological underpinnings and how things work for people of various different sizes and metabolic rates, as well as everything you’d expect about dosing, side effects, and whatnot—as well as things you might not have considered closely related, such gut health, and the question of “is there any way to retain the slimmer figure after stopping?”.
The style is methodical and clear, and not at all sensationalized. It’s very much a “read it cover to cover” book rather than a “dip in” book, so be ready for that, though.
Bottom line: if you and/or a loved one are on GLP1-RAs—or on the fence about them—this is a very even-minded and helpfully explanatory book.
Click here to check out The GLP-1 Lifestyle, and transform your metabolism!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Water Bath + More Cookbook for Beginners – by Sarah Roslin

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Whether you want to be prepared for the next major crisis that shuts down food supply chains, or just learn a new skill, this book provides the tools!
Especially beneficial if you also grow your own vegetables, but even you just buy those… Home-canned food is healthy, contains fewer additives and preservatives, and costs less in the long run.
Roslin teaches an array of methods, including most importantly:
- fermentation and pickling
- water bath canning, and
- pressure canning.
As for what’s inside? She covers not just vegetables, but also fruit, seafood, meat… Basically, anything that can be canned.
The book explains the tools and equipment you will need as well as how to perform it safely—as well as common mistakes to avoid!
Lest we be intimidated by the task of acquiring appropriate equipment, she also walks us through what we’ll need in that regard too!
Last but not least, there’s also a (sizeable) collection of simple, step-by-step recipes, catering to a wide variety of tastes.
Bottom line: a highly valuable resource that we recommend heartily.
Share This Post
-

How Does Fat Actually Leave The Body? Where Does It Go?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fat loss is often misunderstood, with many believing it simply “vanishes” through exercise, is simply excreted in solid form in the bathroom, or materially disappears when converted for energy. However, the principle of conservation of mass plays out here, in that the mass in fat doesn’t disappear—it changes its arrangement:
In and out
Fat is composed of carbon, hydrogen, and oxygen atoms, with an example common form of fat in the body being C55H104O6. That’s a lot of Cs and Hs, and a few Os.
When fat leaves the body, it has been primarily converted into carbon dioxide (CO2) and water (H2O).
According to a 2014 study by the University of South Wales, 84% of the mass of fat exits the body as CO2 exhaled through breathing, while 16% leaves as water through sweat, urine, and other bodily fluids (all of which contain H2O).
You’ll notice there are a lot more Os going out, proportionally, than we originally had in the C55H104O6. For this reason, the process requires oxygen intake; for every 10 kilograms of fat burned, by simple mathematics the body needs around 29 kilograms of oxygen.
Physical activity plays a crucial role in fat loss. When the body exerts itself, it naturally switches to a higher oxygen metabolism necessary for fat breakdown. This effect is amplified during intermittent fasting, which boosts human growth hormone (HGH), a hormone that aids in fat metabolism.
However, simply hyperventilating won’t work; exercise is essential to activate these processes—otherwise it’s just a case of oxygen in, oxygen out, without involving the body’s chemical energy reserves.
Consequently, one of the best diet-and-exercise combinations for fat loss is intermittent fasting with high-intensity interval training.
And, as for what to eat, this video says raw vegan, but honestly, that’s not scientific consensus. However, a diet rich in unprocessed (or minimally processed) fruits and vegetables definitely is where it’s at, with the plant-heavy Mediterranean diet generally scoring highest—which can be further improved by skipping the mammals to make it pesco-Mediterranean. Current scientific consensus does not give any extra benefits for also omitting moderate consumption of fish and fermented dairy products, so include those if you want, or skip those if you prefer.
For more on all of this, enjoy:

Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Are You A Calorie-Burning Machine? (Calorie Mythbusting)
Take care!
Share This Post
-

What happens in my brain when I get a migraine? And what medications can I use to treat it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine is many things, but one thing it’s not is “just a headache”.
“Migraine” comes from the Greek word “hemicrania”, referring to the common experience of migraine being predominantly one-sided.
Some people experience an “aura” preceding the headache phase – usually a visual or sensory experience that evolves over five to 60 minutes. Auras can also involve other domains such as language, smell and limb function.
Migraine is a disease with a huge personal and societal impact. Most people cannot function at their usual level during a migraine, and anticipation of the next attack can affect productivity, relationships and a person’s mental health.

Francisco Gonzelez/Unsplash What’s happening in my brain?
The biological basis of migraine is complex, and varies according to the phase of the migraine. Put simply:
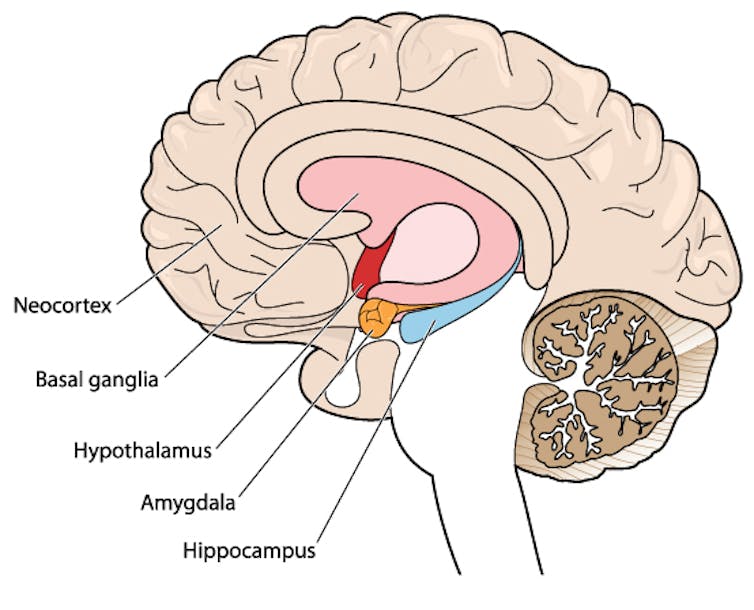
The earliest phase is called the prodrome. This is associated with activation of a part of the brain called the hypothalamus which is thought to contribute to many symptoms such as nausea, changes in appetite and blurred vision.
The hypothalamus is shown here in red. Blamb/Shutterstock Next is the aura phase, when a wave of neurochemical changes occur across the surface of the brain (the cortex) at a rate of 3–4 millimetres per minute. This explains how usually a person’s aura progresses over time. People often experience sensory disturbances such as flashes of light or tingling in their face or hands.
In the headache phase, the trigeminal nerve system is activated. This gives sensation to one side of the face, head and upper neck, leading to release of proteins such as CGRP (calcitonin gene-related peptide). This causes inflammation and dilation of blood vessels, which is the basis for the severe throbbing pain associated with the headache.
Finally, the postdromal phase occurs after the headache resolves and commonly involves changes in mood and energy.
What can you do about the acute attack?
A useful way to conceive of migraine treatment is to compare putting out campfires with bushfires. Medications are much more successful when applied at the earliest opportunity (the campfire). When the attack is fully evolved (into a bushfire), medications have a much more modest effect.
Aspirin
For people with mild migraine, non-specific anti-inflammatory medications such as high-dose aspirin, or standard dose non-steroidal medications (NSAIDS) can be very helpful. Their effectiveness is often enhanced with the use of an anti-nausea medication.
Triptans
For moderate to severe attacks, the mainstay of treatment is a class of medications called “triptans”. These act by reducing blood vessel dilation and reducing the release of inflammatory chemicals.
Triptans vary by their route of administration (tablets, wafers, injections, nasal sprays) and by their time to onset and duration of action.
The choice of a triptan depends on many factors including whether nausea and vomiting is prominent (consider a dissolving wafer or an injection) or patient tolerability (consider choosing one with a slower onset and offset of action).
As triptans constrict blood vessels, they should be used with caution (or not used) in patients with known heart disease or previous stroke.
Triptans should be used cautiously in patients with heart disease. CDC/Unsplash Gepants
Some medications that block or modulate the release of CGRP, which are used for migraine prevention (which we’ll discuss in more detail below), also have evidence of benefit in treating the acute attack. This class of medication is known as the “gepants”.
Gepants come in the form of injectable proteins (monoclonal antibodies, used for migraine prevention) or as oral medication (for example, rimegepant) for the acute attack when a person has not responded adequately to previous trials of several triptans or is intolerant of them.
They do not cause blood vessel constriction and can be used in patients with heart disease or previous stroke.
Ditans
Another class of medication, the “ditans” (for example, lasmiditan) have been approved overseas for the acute treatment of migraine. Ditans work through changing a form of serotonin receptor involved in the brain chemical changes associated with the acute attack.
However, neither the gepants nor the ditans are available through the Pharmaceutical Benefits Scheme (PBS) for the acute attack, so users must pay out-of-pocket, at a cost of approximately A$300 for eight wafers.
What about preventing migraines?
The first step is to see if lifestyle changes can reduce migraine frequency. This can include improving sleep habits, routine meal schedules, regular exercise, limiting caffeine intake and avoiding triggers such as stress or alcohol.
Despite these efforts, many people continue to have frequent migraines that can’t be managed by acute therapies alone. The choice of when to start preventive treatment varies for each person and how inclined they are to taking regular medication. Those who suffer disabling symptoms or experience more than a few migraines a month benefit the most from starting preventives.
Some people will take medicines to prevent migraines. Tbel Abuseridze/Unsplash Almost all migraine preventives have existing roles in treating other medical conditions, and the physician would commonly recommend drugs that can also help manage any pre-existing conditions. First-line preventives include:
- tablets that lower blood pressure (candesartan, metoprolol, propranolol)
- antidepressants (amitriptyline, venlafaxine)
- anticonvulsants (sodium valproate, topiramate).
Some people have none of these other conditions and can safely start medications for migraine prophylaxis alone.
For all migraine preventives, a key principle is starting at a low dose and increasing gradually. This approach makes them more tolerable and it’s often several weeks or months until an effective dose (usually 2- to 3-times the starting dose) is reached.
It is rare for noticeable benefits to be seen immediately, but with time these drugs typically reduce migraine frequency by 50% or more.
‘Nothing works for me!’
In people who didn’t see any effect of (or couldn’t tolerate) first-line preventives, new medications have been available on the PBS since 2020. These medications block the action of CGRP.
The most common PBS-listed anti-CGRP medications are injectable proteins called monoclonal antibodies (for example, galcanezumab and fremanezumab), and are self-administered by monthly injections.
These drugs have quickly become a game-changer for those with intractable migraines. The convenience of these injectables contrast with botulinum toxin injections (also effective and PBS-listed for chronic migraine) which must be administered by a trained specialist.
Up to half of adolescents and one-third of young adults are needle-phobic. If this includes you, tablet-form CGRP antagonists for migraine prevention are hopefully not far away.
Data over the past five years suggest anti-CGRP medications are safe, effective and at least as well tolerated as traditional preventives.
Nonetheless, these are used only after a number of cheaper and more readily available first-line treatments (all which have decades of safety data) have failed, and this also a criterion for their use under the PBS.
Mark Slee, Associate Professor, Clinical Academic Neurologist, Flinders University and Anthony Khoo, Lecturer, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post




Related Posts
-
The Menopause Risk That Nobody Talks About
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In this week’s health news round up, we cover menopausal disordered eating, air pollution & Alzheimer’s, and cold sore comebacks:
When the body starts changing…
Eating disorders are often thought of as a “teenage girl thing”. But in fact, eating disorders in girls/women mostly occur along with “the three Ps”:
- Puberty
- Pregnancy
- Perimenopause & menopause
In very many cases, it’s likely “my body is changing and I have strong opinions on how it should be”. Those opinions are often reflective of societal norms and pressures, but still, they are earnestly felt also. In the case of pregnancy, the societal pressures and standards are generally lifted while pregnant, but come back immediately postpartum, with an expectation to rebound quickly into the same shape one was in beforehand. And in the case of menopause, this is often concurrent with a sense of loss of identity, and can be quite reactionary against what is generally considered to be the ravages of time.
Of course, looking after one’s health is great at any age, and certainly there is no reason not to pursue health goals and try to get one’s body the way one wants it. However, it is all-too-easy for people to fall into the trap of taking drastic steps that are not actually that healthy, in the hopes of quick results.
Further, 13% of women over 50 report current core eating disorder symptoms, and that is almost certain vastly underreported.
Read in full: Eating disorders don’t just affect teen girls—the risk may also go up around pregnancy and menopause
Related: Body Image Dissatisfaction/Appreciation Across The Ages From Age 16 To Age 88
Where there’s smoke…
It’s been known for a while that air pollution is strongly associated with Alzheimer’s disease incidence, but exactly how this happens has not been entirely clear, beyond that it involves S-nitrosylation, in which NO-related particles bind to sulfur (S) atoms, forming SNO (and scientists being how they are, the term for the resultant brain effect has been called a SNO-STORM).
However, researchers have now found that it has to do with how certain toxins in the air (notwithstanding our heading here, they don’t have to be smoke—it can be household chemicals or other things too) cause this resultant SNO to interfere with protein CRTC1, which is critical for forming/maintaining connections between brain cells.
This is important, because it means that if a drug can be made that selectively blocks S-nitrosylatoin actions affecting CRTC1, it can reverse a lot of Alzheimer’s brain damage (as was found in the laboratory, when testing the theory with CRTC1 proteins that had been genetically engineered to resist S-nitrosylation, which is not something we can do with living human brains yet, but it is “proof of principle” and means funding will likely be forthcoming to find drugs to do the same thing).
Read in full: Study reveals how air pollution contributes to Alzheimer’s disease
Related: 14 Powerful Strategies To Prevent Dementia
The virus that comes back from the cold
Cold sores are created by the Herpes simplex virus (yes, the same one as for the genital variety), and by adulthood, most of us are either infected (and periodically get cold sores), or else infected (as an asymptomatic carrier). A noteworthy minority, but a minority nevertheless, are immune. Unless you’ve never had physical contact with other humans, it’s highly unlikely you’re not in one of the above three categories.
For those who do get cold sores, they can seem random in their reoccurrence, but in reality the virus never went away; it was just dormant for a while.
This much was known already, but scientists have now identified the trigger protein (known as “UL 12.5” to its friends) that acts as an alarm clock for the virus—which may pave the way to a greatly-improved treatment, if a way can be found to safely interfere with that wake-up call:
Read in full: Cold sore discovery identifies unknown trigger for those annoying flare-ups
Related: Beyond Supplements: The Real Immune-Boosters!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Aging Backwards – by Miranda Esmonde-White
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In this book, there’s an upside and a downside to the author’s professional background:
- Upside: Miranda Esmonde-White is a ballet-dancer-turned-physical-trainer, and it shows
- Downside: Miranda Esmonde-White is not a scientist, and it shows
She cites a lot of science, but she either does not understand it or else intentionally misrepresents it. We will assume the former. But as one example, she claims:
“for every minute you exercise, you lengthen your life by 7 minutes”
…which cheat code to immortality is absolutely not backed-up by the paper she cites for it. The paper, like most papers, was much more measured in its proclamations; “there was an association” and “with these conditions”, etc.
Nevertheless, while she misunderstands lots of science along the way, her actual advice is good and sound. Her workout programs really will help people to become younger by various (important, life-changing!) metrics of biological age, mostly pertaining to mobility.
And yes, this is a workout-based approach; we won’t read much about diet and other lifestyle factors here.
Bottom line: it has its flaws, but nevertheless delivers on its premise of helping the reader to become biologically younger through exercises, mostly mobility drills.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Get Past Executive Dysfunction
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In mathematics, there is a thing called the “travelling salesman problem”, and it is hard. Not just subjectively; it is classified in mathematical terms as an “NP-hard problem”, wherein NP stands for “nondeterministic polynomial”.
The problem is: a travelling salesman must visit a certain list of cities, order undetermined, by the shortest possible route that visits them all.
To work out what the shortest route is involves either very advanced mathematics, or else solving it by brute force, which means measuring every possible combination order (which number gets exponentially larger very quickly after the first few cities) and then selecting the shortest.
Why are we telling you this?
Executive dysfunction’s analysis paralysis
Executive dysfunction is the state of knowing you have things to do, wanting to do them, intending to do them, and then simply not doing them.
Colloquially, this can be called “analysis paralysis” and is considered a problem of planning and organizing, as much as it is a problem of initiating tasks.
Let’s give a simple example:
You wake up in the morning, and you need to go to the bathroom. But the bathroom will be cold, so you’ll want to get dressed first. However, it will be uncomfortable to get dressed while you still need to use the bathroom, so you contemplate doing that first. Those two items are already a closed loop now. You’re thirsty, so you want to have a drink, but the bathroom is calling to you. Sitting up, it’s colder than under the covers, so you think about getting dressed. Maybe you should have just a sip of water first. What else do you need to do today anyway? You grab your phone to check, drink untouched, clothes unselected, bathroom unvisited.
That was a simple example; now apply that to other parts of your day that have much more complex planning possible.
This is like the travelling salesman problem, except that now, some things are better if done before or after certain other things. Sometimes, possibly, they are outright required to be done before or after certain other things.
So you have four options:
- Solve the problem of your travelling-salesman-like tasklist using advanced mathematics (good luck if you don’t have advanced mathematics)
- Solve the problem by brute force, calculating all possible variations and selecting the shortest (good luck getting that done the same day)
- Go with a gut feeling and stick to it (people without executive dysfunction do this)
- Go towards the nearest item, notice another item on the way, go towards that, notice a different item on the way there, and another one, get stuck for a while choosing between those two, head towards one, notice another one, and so on until you’ve done a very long scenic curly route that has narrowly missed all of your targetted items (this is the executive dysfunction approach).
So instead, just pick one, do it, pick another one, do it, and so forth.
That may seem “easier said than done”, but there are tools available…
Task zero
We’ve mentioned this before in the little section at the top of our daily newsletter that we often use for tips.
One of the problems that leads to executive function is a shortage of “working memory”, like the RAM of a computer, so it’s easy to get overwhelmed with lists of things to do.
So instead, hold only two items in your mind:
- Task zero: the thing you are doing right now
- Task one: the thing you plan to do next
When you’ve completed task zero, move on to task one, renaming it task zero, and select a new task one.
With this approach, you will never:
- Think “what did I come into this room for?”
- Get distracted by alluring side-quests
Do not get corrupted by the cursed artefact
In fantasy, and occasionally science fiction, there is a trope: an item that people are drawn towards, but which corrupts them, changes their motivations and behaviors for the worse, as well as making them resistant to giving the item up.
An archetypal example of this would be the One Ring from The Lord of the Rings.
It’s easy to read/watch and think “well I would simply not be corrupted by the cursed artefact”.
And then pick up one’s phone to open the same three apps in a cycle for the next 40 minutes.
This is because technology that is designed to be addictive hijacks our dopamine processing, and takes advantage of executive dysfunction, while worsening it.
There are some ways to mitigate this:
Rebalancing Dopamine (Without “Dopamine Fasting”)
…but one way to avoid it entirely is to mentally narrate your choices. It’s a lot harder to make bad choices with an internal narrator going:
- “She picked up her phone absent-mindedly, certain that this time it really would be only a few seconds”
- “She picked up her phone for the eleventy-third time”
- “Despite her plan to put her shoes on, she headed instead for the kitchen”
This method also helps against other bad choices aside from those pertaining to executive dysfunction, too:
- “Abandoning her plan to eat healthily, she lingered in the confectionary aisle, scanning the shelves for sugary treats”
- “Monday morning will be the best time to start my new exercise regime”, she thought, for the 35th week so far this year
Get pharmaceutical or nutraceutical help
While it’s not for everyone, many people with executive dysfunction benefit from ADHD meds. However, they have their pros and cons (perhaps we’ll do a run-down one of these days).
There are also gentler options that can significantly ameliorate executive dysfunction, for example:
Bacopa Monnieri: A Well-Evidenced Cognitive Enhancer For Focus & More
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: