The Foot Book – by Dr. Todd Brennan & Dr. Leslie Johnston
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book really is what the subtitle claims it to be: “everything you need to know to take care of your feet”.
Arthritis, bunions, corns, diabetes, eczema, fungus, gout, heel pain, ingrown toenails, joint issues, and that’s just one item for each of the first 10 letters of the alphabet.
There’s a lot in here; the point is that it covers everything from the “serious” to the “cosmetic”, so whether you want to be a foot model for an expensive perfume company or just want to walk without pain, the answer is probably in here.
The goal of this book is to be comprehensive like that, and also with an open agenda to educate the world as to what it actually is that podiatrists do (hint: their years of medical school and further training in residency are not just so that they can trim toenails nicely).
The style is very light and readable, as one might expect from a pair of doctors with many years of experience of explaining exactly these things to patients every day.
Bottom line: if you have feet and would like them to be/remain in good condition, this book is an invaluable resource!
Click here to check out The Foot Book, and take good care of yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is It Worth Taking Testosterone In Menopause?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Why are some people recommending taking testosterone for menopause, doesn’t testosterone go up in menopause anyway?❞
A good question with an interesting answer!
To answer the second part first though: testosterone goes up relative to estrogen, and this relative rise of testosterone is part of what’s responsible for androgenic (masculinizing) effects that occur in menopause. This is a process that, if untreated, will continue to have cumulative effects over time for the rest of one’s life.
See also: Menopause, & When Not To Let Your Guard Down
However, while testosterone goes up relative to estrogen, it actually goes down in terms of its own actual numbers—it’s just that testosterone undergoes a slow, gradual decline, while estrogen plummets quickly. Thus, because of the shortage of estrogen to oppose its masculinizing effects, even the technically now-lower total amount of testosterone is able to do more than the previously higher (but opposed by estrogen) levels were able to do.
It’s worth noting that prior to menopause, most women produce about 3x more testosterone than estrogen—it’s just that estrogen is a lot more powerful, mol for mol, mg for mg.
So of course, when that estrogen drops off, testosterone takes the wheel.
See also: What You Should Have Been Told About The Menopause Beforehand
You may be wondering where this testosterone comes from: circulating testosterone is produced by the ovaries (25%) and the adrenal glands (25%), and the rest comes from peripheral conversion of adrenal androgens in fat cells (50%). So, if for example you have a bilateral ovariectomy (also called oophorectomy), then you’ll only actually take a 25% hit to testosterone levels, assuming normal function beforehand. In contrast, someone having a bilateral orchiectomy (also called orchidectomy, and is the removal of the testes) would take a 95% hit to testosterone levels, assuming normal function beforehand.
This is because the ovaries/testes are (usually, aside from in some intersex conditions) specialized to produce mostly estrogen or testosterone, respectively, since they were differentiated during gestation (prior to that, they were the same basic undifferentiated gonads).
Alright, that’s the “doesn’t testosterone go up in menopause anyway?” part covered, now onto the “why are some people recommending taking testosterone for menopause?” part!
Why it gets prescribed
Testosterone—albeit at much lower levels than for men—can be important in women for bone density and muscle mass, cognitive function, mood, sexual function, and energy.
Of those 5 things, there is one that stands out as the reason that’s usually the reason, and that’s…
❝Numerous studies have shown that adding testosterone to hormonal therapy can improve sexual function and general wellbeing among women during their menopause. A recent systematic review and meta-analysis of testosterone treatment in women has provided robust support for a trial of testosterone in women when clinically indicated. In postmenopausal women, testosterone supplementation improved several domains of sexual response, including sexual desire, pleasure, arousal, orgasm, and self-image.❞
You may be wondering: are there any side effects?
And the answer is yes, but with nuance that’s worth understanding:
❝A significant rise in the amount of LDL-cholesterol, and reductions in the amounts of total cholesterol, HDL-cholesterol, and triglycerides, were seen with testosterone administered orally, but not when administered non-orally (e.g. by transdermal patch or cream).
An overall increase in weight* was recorded with testosterone treatment. No effects of testosterone were reported for body composition, musculoskeletal variables, or cognitive measures, although the number of women who contributed data for these outcomes was small.
Testosterone was associated with a significantly greater likelihood of reporting acne and [facial] hair growth, but no serious adverse events were recorded.❞
*However, since no effects were reported for body composition (i.e. they probably didn’t record it), there is a strong chance that the increase in weight was due to testosterone-induced increase in muscle mass, not an increase in fat. If anything, testosterone will tend towards reducing body fat percentage (which is why men’s healthy body fat levels are lower than women’s healthy body fat levels, on average; it is hormones that mediate this).
Read in full: Safety and efficacy of testosterone for women: a systematic review and meta-analysis of randomised controlled trial data
Further,
❝Androgenic Side Effects:
Exogenous androgen given to women in sufficient quantities or for a sufficient duration can promote androgenic side effects such as acne, hirsutism, and, in extreme cases, virilization.
Virilization includes deepening of the voice, clitoromegaly, masculinization of body habitus, and androgenic alopecia.❞
About some those terms:
- Androgenic alopecia = male pattern baldness; actually the same condition as female pattern baldness, but the visual pattern is slightly different according to testosterone levels.
- Clitoromegaly = the clitoris is receiving hormone-mediated instructions to be a penis (bearing in mind, these two organs are analogous, and were the same undifferentiated organ before they were normally differentiated during gestation), and as such, the visible glans clitoris (the part you can see) will grow (up to an inch or so) and start responding to stimulation like a penis instead of like a clitoris (what feels good to it will change accordingly), and the sensation of orgasm will change too. While many people might not mind this, it’s definitely something worth knowing about in advance!
Read in full: The Safety of Testosterone Therapy in Women
So, while we are neither your gynecologist nor your endocrinologist, we can say that the decision-making process might look something like this:
- Are your T-levels in healthy female ranges (5–55ng/DL, or 0.2–1.9nmol/L)? If so, supplementation will not be indicated for most women.
- If they’re below that, are you experiencing any of the problems commonly associated with such, of which the most evident is usually sexual function (where other* causes of loss of sexual function have been ruled out or otherwise adequately addressed)?
- If you are, do you want to fix that more than you want to avoid the side effects of taking T?
*for example, such as discussed in Come As You Are – by Dr. Emily Nagoski
If so, then talking to a potential prescriber seems like a fine option.
But! There is one last problem, and it’s hardly insurmountable, but it is an inconvenience. For obvious reasons, that vast majority of supplemental testosterone produced is made for men. Now, in and of itself this isn’t an issue; it’s the exact same substance and will work the exact same way in you as it will in a man.
However, it does mean that the doses in which testosterone is most readily available, tend to be aimed at delivering testosterone in normal male quantities, which is about 10x what you’ll want (unless your intention is actually to trans your gender, in which case, congratulations on your manliness). This means that, assuming you want a normal female amount of testosterone, then—depending on the source—you may have to get a bit fiddly with it, since you’re going to be taking the amount that the manufacturer expected to be a daily dose, and making that last 10 days.
For example, if you get T-gel in a dispenser at the standard 1.62% percent/20.25mg per pump, then if a man is prescribed 2 pumps per day then you might be prescribed 0.2 pumps per day. It’s the medical equivalent of a recipe that calls for ⅕ of an egg, which is awkward, and does create risks of accidentally taking more than you wanted.
One last note…
If the issue is libido, you might want to try progesterone (if you’re not already on it) before you try testosterone, as that does boost libido, and is also responsible for a number of other important things, including playing a critical role in bone turnover rates:
Progesterone Menopausal HRT: When, Why, And How To Benefit
And if it’s specifically vaginal dryness that’s the issue, often testosterone is the opposite of what’s needed (though DHEA can help):
Vaginal Dryness In Menopause | Causes & Solutions
Enjoy!
Share This Post
-

The Telomere Effect – by Dr. Elizabeth Blackburn and Dr. Elissa Epel
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Telomeres can be pretty mystifying to the person with a lay interest in longevity. Beyond “they’re the little caps that sit on the end of your DNA, and longer is better, and when they get short, damage occurs, and aging”, how do they fit into the big picture?
Dr. Elizabeth Blackburn and Dr. Elissa Epel excel at explaining the marvelous world of telomeres…
- how they work
- what affects them
- and how and why
…and the extent to which changes are or aren’t reversible.
For some of us, the ship has sailed on avoiding a lot of early-life damage to our telomeres, and now we have a damage-mitigation task ahead. That’s where the authors get practical.
Indeed, the whole third part of the book is titled “Help Your Body Protect Its Cells“, and indeed covers not just “from now on” protection, but undoing some of the damage already done (yes, telomeres can be lengthened—it gets harder as we get older, but absolutely can be done).
In short: if you’d like to avoid further damage to your telomeres where possible, and reverse some of the damage done already, this book will set you on the right track.
Share This Post
-

Which Comes First, Cardio or Weights? – by Alex Hutchinson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a book of questions and answers, myths and busts, and in short, all things exercise.
It’s laid out as many micro-chapters with questions as headers. The explanations are clear and easy to understand, with several citations (of studies and other academic papers) per question.
While it’s quite comprehensive (weighing in at a hefty 300+ pages), it’s not the kind of book where one could just look up any given piece of information that one wants.
Its strength, rather, lies in pre-emptively arming the reader with knowledge, and correcting many commonly-believed myths. It can be read cover-to-cover, or just dipped into per what interests you (the table of contents lists all questions, so it’s easy to flip through).
Bottom line: if you’ve found the world of exercise a little confusing and would like it demystifying, this book will result in a lot of “Oooooh” moments.
Click here to check out Which Comes First, Cardio or Weights?, and know your stuff!
PS: the short answer to the titular question is “mix it up and keep it varied”
Share This Post


-
Injured your ACL? It’s more than just a knee injury
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
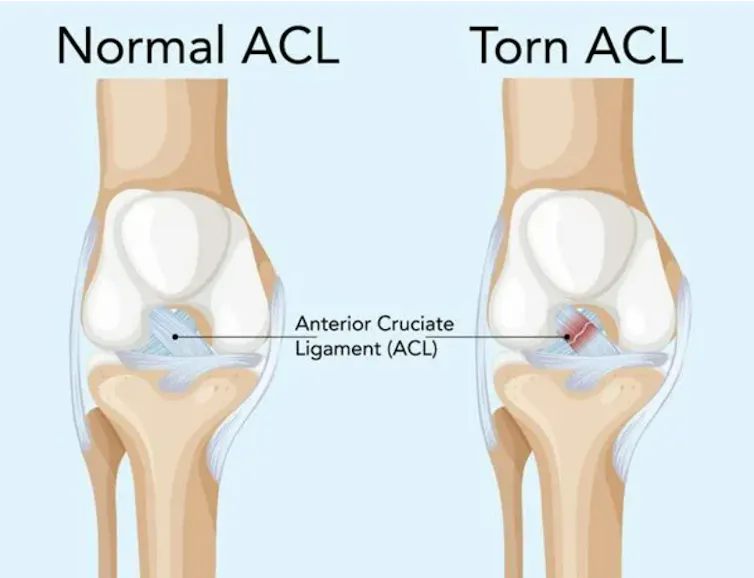
It’s an athlete’s worst fear. Hearing a loud “pop” and feeling severe pain are usually the first signs you’ve torn your anterior cruciate ligament, also known as the ACL.
The ACL connects your shin and thigh bones, and is one of the key ligaments that help stabilise your knee joint.
Research suggests ACL injuries are becoming increasingly common across all age groups. Children as young as ten are rupturing their ACLs, with many never regaining their pre-injury strength or ability.
So how do ACL injuries happen? And what makes them so serious?

Paul Kane/Getty Why the ACL matters
The ACL is an indispensable part of your knee joint. Its main job is to keep your knee stable by stopping it from rotating or extending too much. This is especially important if you regularly twist, pivot or land on your knee joint.
ACL injuries are most often a result of the fatigue-failure process. This is the idea that repeatedly using and putting strain on the ACL, without proper training, makes it significantly weaker over time.
Doing specific strength exercises and regular physical activity can help slow this process. But if you don’t do these activities, even minor movements can gradually weaken your ACL.
Importantly, ACL injuries don’t just affect elite athletes. Injury rates are just as high in amateur and community sport, where access to athletic rehabilitation is typically more limited. This means people playing at amateur levels can face longer, more uncertain paths to recovery compared to professional athletes who have a specialist team of medical and performance staff. As a result, many amateur athletes stop playing sport altogether.
Why are ACL injuries so severe?
Unlike many other tissues in the body, the ACL has a very limited capacity to heal. Once torn or damaged, it can’t regenerate in a way that restores its original structure or function.
The ACL is a crucial ligament in the knee joint. blueringmedia/Getty ACL injuries impact the stability of the knee, often causing the joint to “give way”. This leads to physical symptoms such as pain and swelling. But ACL injuries can also damage other parts of the leg including the meniscus, cartilage and other ligaments.
Over time, a person with an ACL injury may develop osteoarthritis, a painful condition where the cartilage in your knee breaks down and causes the bones to rub together. Even with appropriate medical care, one in two people who tear their ACL will have knee osteoarthritis.
The road to recovery
Recovering from an ACL injury can be a long, and at times painful, process that typically lasts between nine and 12 months. Any attempt to speed this up increases the risk of re-injury. And subsequent ACL injuries often have more severe consequences than the initial rupture.
The recovery process starts with diagnosis. This usually involves seeing a medical professional, such as a GP or physiotherapist, in a clinic. They often use MRI imaging to assess the damage to your ligaments and knee joint.
Many people will then have surgery to reconstruct their torn ACL. This requires the surgeon to take a piece of suitable tissue, known as a graft, from another part of the body to put it where the torn ligament was. Using special screws, they then secure the replacement tissue to the bone.
No matter how you treat an ACL injury, rehabilitation is key. An exercise physiologist or physiotherapist can help you rebuild the strength and flexibility of your knee joint through exercises focused on reducing swelling and restoring your range of motion.
Rehabilitation is particularly important if you’re planning to return to sport. As you heal and recover, you’ll go through several phases of exercises. By taking this gradual approach, you’ll be better prepared to perform more high-risk movements, such as pivoting or jumping.
Increasingly, ACL rehabilitation prioritises psychological health. This has given rise to a biopsychosocial approach to recovery, where recovery relies on physical healing as well as a positive mindset. Athletes can use strategies such as goal setting to manage the emotional ups-and-downs of sustaining a serious injury. This approach also recognises how crucial an athlete’s support network, which may include coaches, teammates and family, is to their recovery.
Injuring your ACL can take an immense physical and psychological toll. That’s why getting support from qualified medical professionals, as well as a close social network, is vital.
Daniel Kadlec, Researcher, Athlete Health and Performance, School of Medical and Health Sciences, Edith Cowan University and Caitlin Fox-Harding, Senior Lecturer/Researcher in Exercise and Sports Science, Edith Cowan University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Heart Healthy Diet Plan – by Stephen William
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve covered heart-healthy cooking books before, but variety is good, and boredom is an enemy of health, so let’s shake it up with a fresh stack of recipes!
After a brief overview of the relevant science (which if you’re a regular 10almonds reader, probably won’t be new to you), the author takes the reader on a 28-day journey. Yes, we know the subtitle says 30 days, but unless they carefully hid the other two days somewhere we didn’t find, there are “only” 28 inside. Perhaps the publisher heard it was a month and took creative license. Or maybe there’s a different edition. Either way…
Rather than merely giving a diet plan (though yes, he also does that), he gives a wide range of “spotlight ingredients”, such that many of the recipes, while great in and of themselves, can also be jumping-off points for those of us who like to take recipes and immediately do our own things to them.
Each day gets a breakfast, lunch, dinner, and he also covers drinks, desserts, and such like.
Notwithstanding the cover art being a lot of plants, the recipes are not entirely plant-based; there are a selection of fish dishes (and other seafood, e.g. shrimp) and also some dairy products (e.g. Greek yoghurt). The recipes are certainly very “plant-forward” though and many are just plants. If you’re a strict vegan though, this probably isn’t the book for you.
Bottom line: if you’d like to cook heart-healthy but are often stuck wondering “aaah, what to cook again today?”, then this is the book to get you out of any culinary creative block!
Click here to check out the Heart Healthy Diet Plan, and widen your heart-healthy repertoire!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Humor Habit – by Paul Osincup
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ask not for whom the bell tolls… It could be tolling for anyone. Don’t worry about it.It’s probably fine.
More seriously (heh), laughter is good for healthy lifespan, also called healthspan. It eases stress and anxiety, gives our brains neurochemicals they need to function well, and is very pro-social too, which in turn has knock-on positive effects for our own mental health as well as those around us.
This book is a guide to cultivating that humor, finding the funny side in difficult times, and bringing a light-hearted silliness to moments where it helps.
The title suggests it’s about habit-building (and it is!) but it’s also about knowing where to look in your daily life for humorous potential and how to find it, and how to bring that into being in the moment.
The style is that of an instruction manual with a healthy dose of pop-science; first and foremost this is a practical guide, not a several-hundred page exhortation on “find things funny!”, but rather a “hey, psst, here are many sneaky insider tricks for finding the funny“.
Bottom line: this book is not only a very enjoyable read, but also very much the gift that keeps on giving, so treat yourself!
Click here to check out The Humor Habit, and strength your funny-bones!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: