The Collagen Cure – by Dr. James DiNicolantonio
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Collagen is vital for, well, most of our bodies, really. Where me most tend to feel its deficiency is in our joints and skin, but it’s critical for bones and many other tissues too.
You may be wondering: why a 572-page book to say what surely must amount to “take collagen, duh”?
Dr. DiNicolantonio has a lot more of value to offer us than that. In this book, we learn about not just collagen synthesis and usage, different types of collagen, the metabolism of it in our diet (if we get it—vegans and vegetarians won’t). We also learn about the building blocks of collagen (vegans and vegetarians do get these, assuming a healthy balanced diet), with a special focus on glycine, the smallest amino acid which makes up about a third of the mass of collagen (a protein).
Not stopping there, we also learn about the interplay of other nutrients with our metabolism of glycine and, if applicable, collagen. Vitamin C and copper are star features, but there’s a lot more going on with other nutrients too, down to the level of “So take this 75 minutes before this but after that and/but definitely not with the other”, etc.
The style is incredibly clear and readable for something that’s also quite scientifically dense (over 1000 references and many diagrams).
Bottom line: if you’re serious about maintaining your body as you get older, and you’d like a book about collagen that’s a lot more helpful than “take collagen, duh”, then this is the book for you.
Click here to check out The Collagen Cure, and take care of yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Xylitol: Cavity Fighter Or Gut Disruptor?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Michelle Jorgensen explains:
The dose makes the poison
Xylitol is a natural sugar alcohol found in fruits and vegetables, and can also be synthesized in a lab. It neutralizes acids in the mouth, thus helping to prevent cavities.
Concerns about gut microbiome disruption become relevant only when xylitol is consumed in large amounts. The amount used in tooth powder and mouthwash is very small, and most of it is not swallowed (only about 10%, in the case of normal use).
To match harmful levels found in animal studies, you’d need to consume about 13 jars of tooth powder per day. So don’t do that.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Xylitol vs Erythritol – Which is Healthier? ← the answer is xylitol, but this does discuss a concern not mentioned here, which is xylitol’s pro-thrombotic effect.
Take care!
Share This Post
-
What Seasonal Allergies Mean For Your Heart
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most people associate seasonal allergies with itchy eyes and stuffy noses, but the effects can go a lot deeper.
This is because allergic reactions don’t just affect the respiratory system; they trigger chronic inflammation throughout the body, and in fact:
❝Allergic disease is a systemic and inflammatory condition❞
~ Dr. Rauno Joks, whose work we will cite in a moment
The important thing to understand in terms of heart health, is that chronic* systemic inflammation can contribute to coronary artery disease, where plaque buildup in arteries (bearing in mind, arterial plaque is in large part made of dead immune cells) raises the risk of heart attacks and strokes.
*Yes, a season once or twice per year counts as “chronic”.
A large (n=603,140) study found that allergic rhinitis (hay fever) increased the odds of coronary heart disease by 25% and heart attacks by 20%. Asthma, especially during flare-ups, posed an even greater risk:
Beyond biology
The effects aren’t just biological; allergies can limit physical activity, leading to a sedentary lifestyle that harms heart health.
In other words: if you’re not going outdoors because there’s pollen, and you’re not exercising because you’re exhausted, then the rest of your health is going to take a nose-dive (so to speak) too.
So, one more reason to take it seriously and not just dismiss it as “it’s just allergies, I’ll survive”.
Practical takeaways
Some things we can all do:
- Monitor your risk factors; i.e. keep on top of your heart health metrics, especially blood pressure and cholesterol, as well as any known genetic predisposition to cardiovascular disease.
- Watch out for alternative causes: symptoms like fatigue or shortness of breath may not always be allergies; they could signal asthma, reflux (for example if wheezing), or even heart disease. An allergist is a good first port-of-call, though.
- Be cautious with medications: some decongestants / allergy meds / asthma meds can raise blood pressure and/or interfere with other medications. Your pharmacist is the best person to speak to about this; they know this kind of thing much better than doctors, as a rule. And whenever you get a new medication, it is good practice to make a habit of always reading the information leaflet that comes with it, and/or look it up on a reputable website such as Drugs.com or the the BNF, to learn about what it is, how it works, what the risks are, what its contraindications are, etc.
- Don’t ignore warning signs: lightheadedness or chest pain could indicate a heart issue and should be addressed immediately. It’s better to be wrong and temporarily embarrassed, than wrong and permanently dead. Besides, even if it’s not a heart issue, it may be something else that would benefit from attention, so taking it seriously is always a good idea.
Want to know more?
Check out:
- What Your Mucus Says About Your Health
- Antihistamines’ Generation Gap
- Oh, Honey: The Bee’s Knees? ← what science has to say about “honey will inoculate you against allergies”
Take care!
Share This Post
-
Lung cancer screening hopes to save lives. But we also need to watch for possible harms
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There is much to commend about Australia’s lung cancer screening program, which started on July 1.
The program is based on gold-standard trial evidence showing this type of screening is likely to reduce lung cancer deaths.
Some people will have their life prolonged due to this screening, which involves taking low-dose CT scans to look for lung cancer in people with a significant smoking history.
In some of these people, cancer will be detected at an early stage, and they can be treated. Without screening, these people may have died of cancer because it would have been detected at a later, incurable stage.
However, for some people, screening could also harm.
How can screening harm?
Screening for disease, including cancer, can cause harm – during screening, diagnosis and treatment.
With lung cancer screening, a positive scan can prompt an invasive lung biopsy. This is where a sample of lung tissue is obtained with a special needle guided by imaging, or through surgery under anaesthesia.
If, after examination under the microscope, the pathologist thinks there is lung cancer, then more extensive surgery and other treatments will likely follow, all of which have a risk of side effects.
The diagnostic label “lung cancer” itself is distressing, and the stigma attached to the diagnosis may worsen this distress.
These harms and risks may be considered acceptable if the treatment prevents the person’s cancer from progressing.
However, as with other cancers, screening is likely to also cause overdiagnosis and overtreatment. That is, some of the lesions picked up through screening and diagnosed as cancer, would have never caused any trouble if they’d been left alone. If these lesions were left undetected (and untreated), they would never have caused symptoms or shortened the person’s life.
But all patients with a cancer diagnosis will be offered treatment – including surgery, radiotherapy and cancer drugs. Yet patients who really have an indolent (non-lethal) lesion have the same risk of harm from diagnosis and treatment as others, but without potentially benefiting from treatment.
A related issue is that of “incidental findings”. Reports from lung cancer screening programs overseas show there is a large potential to find things other than cancer on the CT scan.
For instance, some people have lung “nodules” (small spots on the scan) that fall short of being suspicious for cancer, but nonetheless need close monitoring with repeat scans for a while. For these people, we need to make sure health-care workers follow protocols that prevent unnecessary intervention in a nodule that is not growing.
The scans can also pick up other conditions. These include calcium in coronary arteries, small aneurysms of the aorta (bulges in the body’s largest artery), or abnormalities in abdominal organs such as the liver.
Some of these “incidental findings” may lead to early detection of disease that can be treated. However, in many cases the findings would not have caused any issues if they’d been left undetected, another example of overdiagnosis. These patients experience risks from further cascades of interventions triggered by the incidental finding, but without these interventions improving their health.
The potential for overdiagnosis and overtreatment is greater if screening extends beyond the high-risk group with a history of heavy smoking. Some people who don’t meet the eligibility criteria may still want to be screened. For example, lung cancer awareness campaigns may lead to people who don’t smoke requesting screening. If screening staff decide to refer them for imaging, this may result in unofficial “leakage” of the screening program to include people at lower risk of cancer.
For example in the United States, an estimated 45% of scans done in its screening program are for people who do not meet eligibility criteria. In China, about 64% of those screened may be technically ineligible.
We see the results of this in a number of Asian countries with widespread, non-targeted screening, including of people who do not smoke. This has resulted in high rates of cancer diagnosis – much higher than we would expect in this low-risk group – and even higher rates of lung surgeries.
These surgeries, which involve cutting into the chest wall to remove lung tissue, carry significant operative risks. They may also cause longer-term impacts by removing normal lung tissue.
Regular independent evaluation needed
In Australia, for the eligible population with a significant smoking history, we anticipate net benefit, on balance, from the screening program.
However, if unintended consequences from screening are higher in real life than in the trials, then this could tip it the other way into net harm.
So, regular independent re-evaluation of the program is needed to ensure anticipated benefits are realised and harms are kept to a minimum.
This should include analysis of data across the population to look for signs of benefit, such as decreases in rates of advanced-stage lung cancer and deaths.
These data should also be scrutinised for signs of harm from overdiagnosis and overtreatment – including of both cancer and non-cancer conditions.
There is much excitement about the potential for lung cancer screening to prevent some Australians from dying from this devastating disease. We too have cautious optimism the program could make a real difference.
But we can’t let this optimism blind us to the potential for harm.
This is the next article in our ‘Finding lung cancer’ series, which explores Australia’s first new cancer screening program in almost 20 years. Read other articles in the series.
More information about the program is available. If you need support to quit smoking, call Quitline on 13 78 48.
Katy Bell, Professor of Clinical Epidemiology, Sydney School of Public Health, University of Sydney; Brooke Nickel, NHMRC Emerging Leader Research Fellow, University of Sydney, and Mark Morgan, Professor of general practice, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post


Related Posts
-
Should I kick my diet soft-drink habit? Where do I start?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The average Australian drinks almost 60 litres of soft drink a year. Many people see diet soft drinks as a “healthier” choice than regular ones, and when it comes to sugar, that’s true.
For example, a 375 millilitre can of Coca-Cola contains about seven teaspoons of added sugar (almost to 40 grams). That’s close to the World Health Organization’s (WHO) daily recommended limit for added sugars of 50g.
In comparison, the Diet Coke version is sweetened with artificial sweeteners such as aspartame and does not contain sugar.
So if you reach for diet soft drinks, is that so bad? Or is it worth giving them up too?

Towfiqu barbhuiya/Pexels Are diet soft drinks really that bad?
Diet soft drinks provide few nutrients. They often contain artificial sweeteners and caffeine, and while they’re low in energy (kilojoules), they aren’t filling.
People who regularly drink diet soft drinks may have a higher risk of developing conditions such as heart disease and type 2 diabetes.
But this doesn’t necessarily mean the drinks cause these conditions. People who already have health concerns or are trying to manage their weight may be more likely to choose diet drinks, which might make this evidence a little misleading.
How about artificial sweeteners?
In 2023, the WHO classified aspartame (a common sweetener found in many diet soft drinks) as “possibly carcinogenic to humans”. This means the evidence linking aspartame to cancer is currently limited and not conclusive.
The WHO also emphasised that the public generally consumes safe levels of aspartame and only has evidence for concern if people drink the equivalent to 14 cans of soft drink a day.
There is also emerging evidence some artificial sweeteners might irritate the gut or alter the balance of gut bacteria. These effects are still being investigated. But they’ve added to concerns about the health impacts of drinking diet soft drinks over a long period of time.
Can I get used to the sweetness?
An occasional diet drink isn’t likely to fuel an addiction to sweet foods, but cutting back is still a good idea if this has become a daily habit.
After people cut back on very sweet foods or drinks, some research suggests they start noticing sweetness more easily and find very sweet things taste too sweet.
So if you’re trying to enjoy less-sweet drinks, give it time. Within a few weeks you might actually prefer the less-sweet taste.
Here are three evidence-based strategies to help you adjust.
1. Water it down
A gentle first step is to dilute your soft drink. Start by pouring less soft drink into a glass and topping it up with water or soda water, then gradually adjust the ratio over time.
It may taste less sweet at first, but your taste buds will adapt. This slow, steady approach can make change feel easier and more sustainable than quitting abruptly.
2. Make smarter swaps
Try replacing diet soft drink with a healthier alternative that still delivers flavour or fizz. Sparkling water or soda water with a squeeze of lime or lemon and a few mint leaves gives you the same bubbly refreshment with a natural and refreshing flavour. Add ice if it is a hot day, or to provide some crunch.
If you prefer plain water but it feels boring, infuse it with slices of fruit, cucumber, berries or herbs.
You could also try unsweetened iced tea, such as black, green or herbal tea. These offer a mild caffeine lift without the added sweeteners and can be served cold with ice and lemon.
Coconut water can also be a healthier alternative as it is low in sugar while providing some additional electrolytes, which help balance fluid in the body.
3. Know your triggers
If you often reach for a soft drink out of habit, boredom or an afternoon energy slump, paying attention to these moments can help. Once you spot your triggers, you can plan a different response. Take a short walk, call a friend or make a cup of tea instead.
Keeping a chilled, reusable water bottle nearby also helps. If your drink is always within reach, you’re less likely to grab a diet soft drink when you’re out and about.
If you drink diet soft drinks because you’re hungry, reach for something nourishing instead, such as a handful of nuts, a yoghurt or a piece of fruit. These foods will satisfy you for longer than a can of diet soft drink because they have nutrients, such as fibre, to keep you fuller for longer.
The bottom line
You don’t have to give up diet soft drinks altogether. But being mindful of how much soft drink you drink, and how often, can help you make choices that better support your long-term health.
Start small, be consistent and let your taste buds adjust. Over time, you might find what once tasted “flat” now feels refreshingly natural.
Lauren Ball, Professor of Community Health and Wellbeing, The University of Queensland; Emily Burch, Accredited Practising Dietitian and Lecturer, Southern Cross University, and Mackenzie Derry, Nutritionist, Dietitian & PhD Candidate, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Recent outbreaks highlight the risks of bacterial meningitis and the need to vaccinate
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Outbreaks of bacterial meningococcal disease in England and recent cases in students in New Zealand have raised awareness of this serious and life-threatening disease.
The disease is caused by the bacterium Neisseria meningitidis and presents as meningitis or blood poisoning (septicaemia).
Meningitis is an inflammation of the membranes that cover the brain and spinal cord (meninges), while septicaemia affects the whole body through the presence of bacteria in the blood stream.
Both can be also be caused by other infectious agents, but bacterial meningococcal disease is the most severe form.
Infants, children and young adults are at higher risk. While the disease is largely preventable through vaccination, only one vaccine is currently on the national immunisation schedule in Aotearoa New Zealand.
As part of ongoing research to explain the recent cases, we compared the meningococcal strains involved in both countries and explored the significance of people who carry the bacterium but don’t develop symptoms or disease.
There are several strains of Neisseria meningitidis and most belong to six groups (named A, B, C, W, X and Y). All have an extraordinary ability to swap genetic material between them and switch genes on and off through a process known as phase variation.
This can change the surface of the bacterium, enabling it to escape the body’s immune system.
The strains responsible for both the UK and recent Dunedin cases belong to Group B meningococci. However, the similarity ends there. The UK outbreak strain is known as ST485, while the Dunedin cases were caused by different strains. They differ from the UK strain as well as from each other, suggesting more than one chain of transmission was involved.
The Bexsero vaccine is used to protect people against bacterial meningitis caused by group B strains. It was designed to recognise components in the outer membrane and on the surface of the bacteria.
The strain that caused the UK outbreak is likely covered by the Bexero vaccine because it matches exactly one of the protein antigen sequences used in the vaccine.
But genomic sequencing of the bacteria responsible for one of the Dunedin cases is still pending, while the other case did not yield a bacterial culture.
Students and staff queue to receive antibiotics at the UK University of Kent after an outbreak of meningitis caused the deaths of two people. Carl Court/Getty Images The importance of genome sequencing
Although meningococcal disease can appear as scattered and apparently unrelated cases, these can occasionally build into larger outbreaks.
Strain typing and genome sequencing can help to determine if an apparent outbreak is due to the emergence of a particular strain or a cluster of cases that are genetically unrelated.
Both scenarios can occur if cases share a common risk factor, such as increased close contact and mixing in educational settings such as schools and universities.
Past genomic surveillance in New Zealand has shown the emergence of outbreak strains and helped identify likely resistance to antibiotics. For example, a W group strain variant caused rising numbers of meningococcal disease between 2016 and 2019 in New Zealand and an outbreak in Northland in 2018.
Genome sequencing showed this strain was different from the W strain causing disease in Europe at the time, and the specific 2015 variant also has increased resistance to penicillin.
Healthy people can be carriers
Despite its ability to cause severe disease, the bacterium causing meningococcal disease is often found in people’s throat, without causing symptoms.
About 5% to 30% of the global population are carriers, and most don’t experience any symptoms or disease. We don’t yet fully understand the factors that determine whether disease develops.
Genome sequencing has shown that some highly virulent strains which are associated with outbreaks are rarely identified in samples from healthy carriers. But as yet, attempts to find genomic explanations for differences in bacteria found in outbreaks and healthy carriers remain inconclusive.
The likelihood whether people carry the bacterium is age dependent. It is low in younger children and older people, but high in teenagers and young adults.
The high carriage rate in young adults makes university students a high-risk group for developing the disease. Crowded living conditions also contribute to the high carriage rate, exacerbating the risk.
In New Zealand, both the Bexsero (against group B) and MenQuadfi (against ACWY) vaccines are available to young people moving into boarding school or university halls the first time. In contrast, only one vaccine (against ACWY) is currently funded for university students in England.
Both vaccines are needed to have maximum protection. Conjugate ACWY vaccines may reduce carriage and therefore transmission. Bexsero does not reduce carriage but protects against development of the disease.
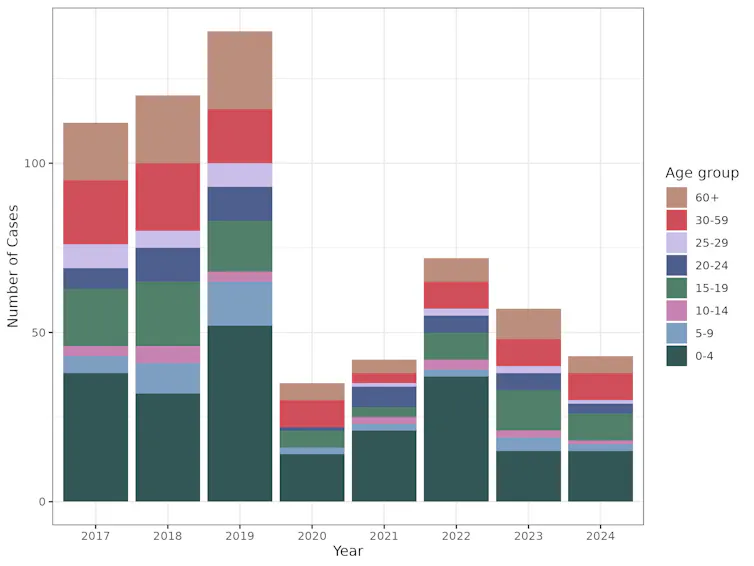
Impact of COVID measures on transmission
Lockdowns and border controls introduced during the COVID pandemic reduced transmission of the SARS-CoV2 virus. But they also had a major effect on other diseases, including influenza and other respiratory viruses.
Cases of meningococcal disease were also dramatically reduced during the COVID response, most likely due to reduced contact between individuals and because fewer infected people entered the country.
This graph shows the drop in cases of meningococcal disease, across all age groups, during the period of COVID lockdowns. Data extracted from the PHF Science notifiable disease dashboard for meningococcal disease, CC BY-SA The rebound in cases following relaxation of these strict measures was expected.
This highlights how important it is to be aware of the risks associated with large gatherings, particularly of young people, and the need to vaccinate with the Bexsero vaccine as part of the immunisation schedule as well as MenQuadfi for high-risk groups.
Una Ren, Senior Scientist in Genomics, New Zealand Institute for Public Health and Forensic Science; Nigel French, Distinguished Professor of Infectious Disease Epidemiology and Public Health, Te Kunenga ki Pūrehuroa – Massey University, and Sarah Hannah, Doctoral Candidate in Epidemiology, Te Kunenga ki Pūrehuroa – Massey University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why does alcohol make my poo go weird?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As we enter the festive season it’s a good time to think about what all those celebratory alcoholic drinks can do to your gut.
Alcohol can interfere with the time it takes for food to go through your gut (also known as the “transit time”). In particular, it can affect the muscles of the stomach and the small bowel (also known as the small intestine).
So, how and why does alcohol make your poos goes weird? Here’s what you need to know.
Diarrhoea and the ‘transit time’
Alcohol’s effect on stomach transit time depends on the alcohol concentration.
In general, alcoholic beverages such as whisky and vodka with high alcohol concentrations (above 15%) slow down the movement of food in the stomach.
Beverages with comparatively low alcohol concentrations (such as wine and beer) speed up the movement of food in the stomach.
These changes in gut transit explain why some people can get a sensation of fullness and abdominal discomfort when they drink vodka or whisky.
How long someone has been drinking a lot of alcohol can affect small bowel transit.
We know from experiments with rats that chronic use of alcohol accelerates the transit of food through the stomach and small bowel.
This shortened transit time through the small bowel also happens when humans drink a lot of alcohol, and is linked to diarrhoea.
Alcohol can also reduce the absorption of carbohydrates, proteins and fats in the duodenum (the first part of the small bowel).
Alcohol can lead to reduced absorption of xylose (a type of sugar). This means diarrhoea is more likely to occur in drinkers who also consume a lot of sugary foods such as sweets and sweetened juices.
Chronic alcohol use is also linked to:
- lactose intolerance
- overgrowth of small bowel bacteria and
- reduced absorption of fats from the pancreas not producing enough digestive enzymes.
This means chronic alcohol use may lead to diarrhoea and loose stools.
How might a night of heavy drinking affect your poos?
When rats are exposed to high doses of alcohol over a short period of time, it results in small bowel transit delay.
This suggests acute alcohol intake (such as an episode of binge drinking) is more likely to lead to constipation than diarrhoea.
This is backed up by recent research studying the effects of alcohol in 507 university students.
These students had their stools collected and analysed, and were asked to fill out a stool form questionnaire known as the Bristol Stool Chart.
The research found a heavy drinking episode was associated with harder, firm bowel motions.
In particular, those who consumed more alcohol had more Type 1 stools, which are separate hard lumps that look or feel a bit like nuts.
The researchers believed this acute alcohol intake results in small bowel transit delay; the food stayed for longer in the intestines, meaning more water was absorbed from the stool back into the body. This led to drier, harder stools.
Interestingly, the researchers also found there was more of a type of bacteria known as “Actinobacteria” in heavy drinkers than in non-drinkers.
This suggests bacteria may have a role to play in stool consistency.
But binge drinking doesn’t always lead to constipation. Binge drinking in patients with irritable bowel syndrom (IBS), for example, clearly leads to diarrhoea, nausea and abdominal pain.
What can I do about all this?
If you’re suffering from unwanted bowel motion changes after drinking, the most effective way to address this is to limit your alcohol intake.
Some alcoholic beverages may affect your bowel motions more than others. If you notice a pattern of troubling poos after drinking certain drinks, it may be sensible to cut back on those beverages.
If you tend to get diarrhoea after drinking, avoid mixing alcohol with caffeinated drinks. Caffeine is known to stimulate contractions of the colon and so could worsen diarrhoea.
If constipation after drinking is the problem, then staying hydrated is important. Drinking plenty of water before drinking alcohol (and having water in between drinks and after the party is over) can help reduce dehydration and constipation.
You should also eat before drinking alcohol, particularly protein and fibre-rich foods.
Food in the stomach can slow the absorption of alcohol and may help protect against the negative effects of alcohol on the gut lining.
Is it anything to worry about?
Changes in bowel motions after drinking are usually short term and, for the most part, resolve themselves pretty efficiently.
But if symptoms such as diarrhoea persist beyond a couple of days after stopping alcohol, it may signify other concerning issues such as an underlying gut disorder like inflammatory bowel disease.
Researchers have also linked alcohol consumption to the development of irritable bowel syndrome.
If problems persist or if there are alarming symptoms such as blood in your stool, seek medical advice from a general practitioner.
Vincent Ho, Associate Professor and clinical academic gastroenterologist, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: