Surviving A Heart Attack? Stroke? There’s An App For That
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
❝Stopped.❞
~ The last words of Dr. Joseph Henry Green, President of the Royal College of Surgeons, who had been taking his own pulse
Sometimes, self-diagnosis isn’t so clear as that, though, especially when it comes to life-threatening issues with the heart and brain (i.e. things we can’t readily look at, and diagnose with the same ease we might diagnose a broken arm or such). Indeed, many people have a heart attack or stroke and, upon finding that they are not dead, conclude “I guess I’m fine after all” and continue about their day
Unfortunately, it’s often the case that in fact they still needed medical attention within the hour (literally: the hour after a heart attack or stroke is called “the golden hour” by doctors in the field, as medical treatments are most effective then, and less likely to help so much afterwards).
As a result, a lot of people die because they didn’t seek medical attention because they dismissed their own experience once the immediate symptoms abated.
About The “Emergency Call for Heart Attack and Stroke” (ECHAS) App
This is a smartphone app that can be used at home to identify the signs of heart attacks and strokes, including:
- A virtual exam using questions similar to those asked in ERs.
- A finger-tapping test to detect one-sided body weakness.
- A risk score to advise whether to call 911, a hotline, or a doctor.
In a moderate-size (n=202) study, it successfully detected strokes in under 2 minutes and heart attacks in 1 minute, and when we say “successfully”, it was 100% accurate in identifying patients who were later admitted to the hospital. Obviously, we cannot say about the patients who didn’t go to hospital, because there was (consequently) no further data for them, but we can conclude:
- there were no false positives (that’s the “100% accurate in identifying patients who were later admitted to the hospital” part)
- while we can’t say for sure there were no false negatives, it is promising that there were no reports of “app said patient was fine, patient then deteriorated/died”, which would have been picked up. So, it looks promisingly like there were no false negatives either.
In terms of ease of use, it was rated by the study participants as very easy to use, making it suitable for people without medical training, and for that matter, people without medical training in the middle of a medical crisis who thus might not be at their best when using it.
You can read the study paper in full, here: Assessment of the Sensitivity of a Smartphone App to Assist Patients in the Identification of Stroke and Myocardial Infarction: Cross-Sectional Study
Sounds great; where can I get it?
At time of writing, it’s not publicly available just yet, but the researchers want to trial it on a much larger scale, so we’ll keep an eye out for invitations to that trial (probably in a huge, crowdsourced data way, like ZOE and 1 Million Nights and such) and advise you to do so, too.
In all likelihood, it’ll appear soon for iPhone and Android in their respective app stores.
In the meantime, you might want to check out:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Studies of Parkinson’s disease have long overlooked Pacific populations – our work shows why that must change

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A form of Parkinson’s disease caused by mutations in a gene known as PINK1 has long been labelled rare. But our research shows it’s anything but – at least for some populations.
Our meta-analysis revealed that people in specific Polynesian communities have a much higher rate of PINK1-linked Parkinson’s than expected. This finding reshapes not only our understanding of who is most at risk, but also how soon symptoms may appear and what that might mean for treatment and testing.
Parkinson’s disease is often thought of as a single condition. In reality, it is better understood as a group of syndromes caused by different factors – genetic, environmental or a combination of both.
These varying causes lead to differences in disease patterns, progression and subsequent diagnosis. Recognising this distinction is crucial as it paves the way for targeted interventions and may even help prevent the disease altogether.

Shutterstock/sfam_photo Why we focus on PINK1-linked Parkinson’s
We became interested in this gene after a 2021 study highlighted five people of Samoan and Tongan descent living in New Zealand who shared the same PINK1 mutation.
Previously, this mutation had been spotted only in a few more distant places –Malaysia, Guam and the Philippines. The fact it appeared in people from Samoan and Tongan backgrounds suggested a historical connection dating back to early Polynesian migrations.
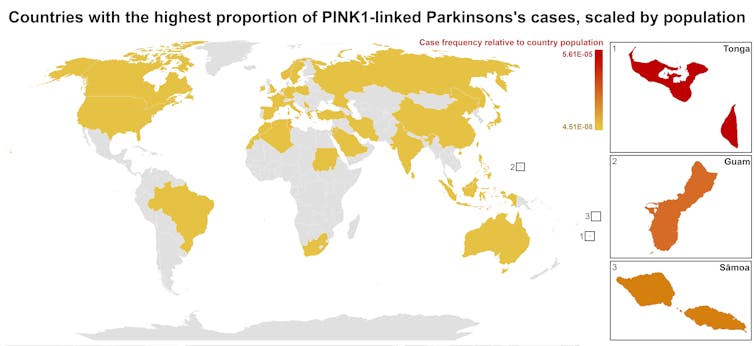
One person in 1,300 West Polynesians carries this mutation. This is a frequency well above what scientists usually classify as rare (below one in 2,200). This discovery means we may be overlooking entire communities in Parkinson’s research if we continue to assume PINK1-linked cases are uncommon.
This world map shows people in some Polynesian communities have a much higher rate of PINK1-linked Parkinson’s than the global population. Eden Yin, CC BY-SA Traditional understanding says PINK1-linked Parkinson’s is both rare and typically strikes younger people, mostly in their 30s or 40s, if they inherit two faulty copies of the gene. In other words, it’s considered a recessive condition, needing two matching puzzle pieces before the disease can unfold.
Our work challenges this view. We show that even one defective PINK1 gene can cause Parkinson’s at an average age of 43, much earlier than the typical onset after 65. That’s a significant departure from the standard belief that only people with two defective gene copies are at risk.
Why this matters for people with the disease
It’s not just genetics that challenge long-held views. Historically, PINK1-linked Parkinson’s was thought to lack some of the classic features of the disease, such as toxic clumps of alpha-synuclein protein.
In typical Parkinson’s, alpha-synuclein builds up in the brain, forming sticky clumps known as Lewy bodies. Our results, contrary to prior beliefs, show that alpha-synuclein pathology is present in 87.5% of PINK1 cases. This finding opens up a promising new avenue for future treatment development.
The biggest concern is early onset. PINK1-linked Parkinson’s can begin as early as 11 years old, although a more common starting point is around the mid-30s. This early onset means living longer with the disease, which can profoundly affect education, work opportunities and family life.
Current treatments (such as levodopa, a precursor of dopamine) help manage symptoms, but they’re not designed to address the root cause. If we know someone has a PINK1 mutation, scientists and clinicians can explore therapies for specific genetic pathways, potentially delivering relief beyond symptom management.
Sex differences add a layer of complexity
In Parkinson’s, generally, men are at higher risk and tend to develop symptoms earlier. However, our findings suggest the opposite pattern for PINK1-linked cases. Particularly, women with two defective copies of the gene experience onset earlier than men.
This highlights the need to consider sex-related factors in Parkinson’s research. Overlooking them risks missing key elements of the disease.
Genetic testing could be a game-changer for PINK1-linked Parkinson’s. Because it often appears earlier, doctors may not recognise it immediately, especially if they are more familiar with the common, later-onset form of Parkinson’s.
Early genetic testing could lead to a faster, more accurate diagnosis, allowing treatment to begin when interventions are most effective. It would help families understand how the disease is inherited, enabling relatives to get tested.
In some cases, where appropriate and culturally acceptable, embryo screening may be considered to prevent the passing of the faulty gene.
Knowing you have a PINK1 mutation could also make finding the right treatment more efficient. Instead of a lengthy trial-and-error process with different medications, doctors could use emerging therapies designed to target the underlying PINK1 mutation rather than relying on general Parkinson’s treatments meant for the broader population.
Addressing research gaps
These findings underscore how crucial it is to include diverse populations in health research.
Many communities, such as those in Samoa, Tonga and other Pacific nations, have had little to no involvement in global Parkinson’s genetics studies. This has created gaps in knowledge and real-world consequences for people who may not receive timely or accurate diagnoses.
Researchers, funding bodies and policymakers must prioritise projects beyond the usual focus on European or industrialised countries to ensure research findings and treatments are relevant to all affected populations.
To better diagnose and treat Parkinson’s, we need a more inclusive approach. Recognising that PINK1-linked Parkinson’s is not as rare as previously thought – and that genetics, sex differences and cultural factors all play a role – allows us to improve care for everyone.
By expanding genetic testing, refining treatments and ensuring research reflects the full spectrum of Parkinson’s, we can move closer to more precise diagnoses, targeted therapies and better support systems for all.
Victor Dieriks, Research Fellow in Health Sciences, University of Auckland, Waipapa Taumata Rau and Eden Paige Yin, PhD candidate in Health Sciences, University of Auckland, Waipapa Taumata Rau
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Nori vs Wakame – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing nori to wakame, we picked the nori.
Why?
It was close, and both of these seaweed options are great!
In terms of macros, nori has more protein while wakame has more carbs; they’re about equal on fiber. While the difference in protein and carbs isn’t big, out of the two we’ll prioritize protein, and thus say nori gets a notional win here—but as it’s so close, one could just as easily call it a tie.
In the category of vitamins both are very rich in many minerals, but nori has more of vitamins A, B1, B2, B6, B12*, and C, while wakame has more of vitamins B5, B9, K, and choline. Thus, a 6:4 victory for nori.
*Yes, nori is one of those rare vegan foods that naturally contain vitamin B12; it’s because of the composition of the algae that this seaweed is made of, which includes some beneficial B12-making bacteria. Meanwhile, wakame is “just” a kelp, so it doesn’t have B12.
When it comes to minerals, nori has more potassium and zinc, while wakame has more calcium and magnesium. They’re equal on other minerals, except: it’s worth noting that wakame is moderately high in sodium, while nori has very little sodium. So, either a tie-breaking win for nori, or just a tie.
Adding up the sections gives nori the overall win; it’s only the margin of the win that’s reasonably debatable. Still, enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
- A Deeper Dive Into Seaweed
- Spirulina vs Nori – Which is Healthier? ← guess which won!
- 21% Stronger Bones in a Year at 62? Yes, It’s Possible (No Calcium Supplements Needed!) ← nori and wakame both feature (very favorably) in this case study
Enjoy!
Share This Post
-
10 Minoxidil Hacks For The Best Hair Growth
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Shereene Idriss advises:
Keep your hair on…
Ok, we would note that tips 1 and 2 seem to be the same (but honestly, it’s a big myth to bust so it bears saying twice), and tips 4 and 10 are more advice about its limitations than actual tips, but we include them all here so that you know we didn’t short-change you!
Number 3 is great advice in particular, as is number 6 if it applies to you; a lot of people don’t think of it:
- Choose between 2% and 5% minoxidil, regardless of gender—5% is more effective and often more cost-efficient.
- Women can safely use the 5% minoxidil strength; avoid the “pink tax” of products marketed specifically to women at a higher price for a lower concentration.
- Consistency matters more than intensity—use minoxidil several times a week if daily application isn’t realistic, and think of results long-term.
- Expect initial shedding between weeks 2–6; this is temporary and normal—results typically start showing after 3 months.
- Apply minoxidil precisely to target areas to avoid unwanted hair growth on the face or body, and wash your hands after use.
- You can use minoxidil with a spoolie brush to regrow thinning eyebrows—just clean the area after application.
- Microneedling the scalp before applying minoxidil can improve absorption and results, but only if done gently and hygienically.
- Minoxidil is toxic to dogs and cats—store it safely, wash your hands after use, and keep it away from your animals at all times.
- If topical minoxidil causes irritation, oral minoxidil (prescription only) may be an alternative—just be aware of possible systemic side effects like unwanted body hair.
- Minoxidil is not a cure but a maintenance treatment—once you stop, hair loss will likely resume, so combine it with other strategies if needed.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
What’s The Difference Between Minoxidil For Men vs For Women?
Take care!
Share This Post


Related Posts
-
Cashew Nuts vs Macadamia Nuts – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cashews to macadamias, we picked the cashews.
Why?
In terms of macros, cashews have more than 2x the protein, while macadamias have nearly 2x the fat. The fats are mostly monounsaturated, so it’s still healthy in moderation, but still, we’re going to prize the protein over it and call this category a nominal win for cashews.
When it comes to vitamins, things are fairly even; cashews have more of vitamins B5, B6, B9, and E, while macadamias have more of vitamins B1, B2, B3, and C.
In the category of minerals, cashews take the clear lead; cashews have more copper, iron, magnesium, phosphorus, potassium, selenium, and zinc, while macadamias have more calcium and manganese.
In short, enjoy both (as macadamias have their benefits too), but cashews win in total nutrient density.
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Taking prescription opioids for too long can be harmful. Here’s how to cut back and stop
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Opioids, such as oxycodone, morphine, codeine, tramadol and fentanyl, are commonly prescribed to manage pain. You might be given a prescription when experiencing pain, or after surgery or an injury.
But while opioids may relieve pain in the short term, they provide little to no lasting improvement in pain or function beyond a few weeks for people whose pain isn’t caused by cancer.
Opioids can also cause side effects such as nausea, constipation and drowsiness, as well as serious risks such as dependence and overdose.
Over the past decade, Australia has introduced initiatives to reduce opioid use and related harm. This includes new guidelines that recommend reducing the dose or stopping opioids when the risks of continuing outweigh the benefits.
Many people can reduce or stop opioids without their pain worsening. Some people even experience less pain. However, for some people, reducing or stopping opioids can result in worse pain, mental health crises and even suicide.
Our new research, published today in the New England Journal of Medicine, explains how to safely reduce and stop taking prescription opioids.
Maskot/Getty Images How do you know when it’s time to stop? Then what?
Determining whether it is appropriate to reduce or stop opioids depends on several factors unique to each person. These include:
- why opioids were prescribed
- how long they’ve been used
- what other treatments you’ve tried
- how the medication affects your pain, function and quality of life
- your life circumstances.
If it’s appropriate to trial reducing or stopping opioids, guidelines from Australia, the United Kingdom and the United States emphasise the following principles:
1) Shared decision-making
Shared decision-making is where health-care professionals and patients work together to set goals, weigh risks and benefits, and make informed choices.
This means collaboratively designing an opioid reduction plan that reflects the person’s needs, preferences and circumstances, rather than imposing a one-size-fits-all approach.
Research shows shared decision-making may lead to better outcomes, and patients value this process.
2) Reduce gradually
Stopping opioids suddenly can cause withdrawal symptoms such as anxiety, insomnia, and stomach upset. Rapid dose reductions can also increase the risk of overdose, mental distress and suicide.
To avoid these risks, opioids should be reduced gradually over weeks, months or even longer. The process should be flexible, allowing for pauses or adjustments to the reduction plan if needed.
When someone takes lower doses of opioids over time, their body’s tolerance decreases. If they return to a higher dose, there is a risk of overdose. For this reason, health-care professionals may recommend having naloxone available. This is a medication that can reverse an opioid overdose.
3) Set up other supports
Supportive strategies should be used before, during and after reducing opioids. These can include:
- physical therapies such as physiotherapy
- psychological approaches such as mindfulness
- non-opioid medications
- mental health support from health-care professionals, friends and family
- education about pain self-management.
The evidence supporting specific interventions is often limited or uncertain. Choosing a strategy will depend on your individual preferences and access. The best approach is likely a combination of several different supports.
4) See your health-care provider for ongoing monitoring
Regular monitoring from a health-care professional is recommended during and after opioid reduction to assess pain, function, withdrawal symptoms and wellbeing.
This can help to ensure that any issues are identified early and are addressed.
If someone experiences a clear decline in their quality of life, for example, it may be necessary to pause or stop the taper and revisit it later, provide extra supports or implement strategies to manage withdrawal symptoms.
We need a health system that supports this process
Making opioid reduction safer and more effective requires putting these principles into practice. But many patients and health-care professionals still face challenges when doing so.
It’s best practice to access a team-based pain management program with support from a doctor, physiotherapist and psychologist, among other providers, to manage pain and reduce the use of opioids. But access to these services remains limited in many parts of Australia.
Not everyone has access to team-based pain management. Hispanolistic/Getty Images Consumer organisations and professional bodies have called for greater access to team-based pain services so more people, especially those living in rural and under-served areas, can access support.
Australian health-care professionals have also requested more education and training in pain management, prescribing and opioid reduction, as well as stronger evidence about what works, for whom and why. This is so they’re better able to tailor their care to each person’s needs.
Other strategies such as reducing the amount of opioids prescribed – including after surgery – have also been proposed to help prevent long-term opioid use and the need for reduction plans later on.
Aili Langford, Pharmacist, Lecturer, NHMRC Emerging Leadership Fellow, Sydney Pharmacy School, The University of Sydney, University of Sydney and Christine Lin, Professor, Institute for Musculoskeletal Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Black Forest Chia Pudding
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This pudding tastes so decadent, it’s hard to believe it’s so healthy, but it is! Not only is it delicious, it’s also packed with nutrients including protein, carbohydrates, healthy fats (including omega-3s), fiber, vitamins, minerals, and assorted antioxidant polyphenols. Perfect dessert or breakfast!
You will need
- 1½ cups pitted fresh or thawed-from-frozen cherries
- ½ cup mashed banana
- 3 tbsp unsweetened cocoa powder
- 2 tbsp chia seeds, ground
- Optional: 2 pitted dates, soaked in hot water for 10 minutes and then drained (include these if you prefer a sweeter pudding)
- Garnish: a few almonds, and/or berries, and/or cherries and/or cacao nibs
Method
(we suggest you read everything at least once before doing anything)
1) Blend the ingredients except for the chia seeds and the garnish, with ½ cup of water, until completely smooth
2) Divide into two small bowls or glass jars
3) Add 1 tbsp ground chia seeds to each, and stir until evenly distributed
4) Add the garnish and refrigerate overnight or at least for some hours. There’s plenty of wiggle-room here, so make it at your convenience and serve at your leisure.
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Cherries’ Very Healthy Wealth Of Benefits!
- If You’re Not Taking Chia, You’re Missing Out
- Cacao vs Carob – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: