Two Things You Can Do To Improve Stroke Survival Chances
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Andrew’s Stroke Survival Guide
This is Dr. Nadine Andrew. She’s a Senior Research Fellow in the Department of Medicine at Monash University. She’s the Research Data Lead for the National Center of Healthy Aging. She is lead investigator on the NHMRC-funded PRECISE project… The most comprehensive stroke data linkage study to date! In short, she knows her stuff.
We’ve talked before about how sample size is important when it comes to scientific studies. It’s frustrating; sometimes we see what looks like a great study until we notice it has a sample size of 17 or something.
Dr. Andrew didn’t mess around in this regard, and the 12,386 participants in her Australian study of stroke patients provided a huge amount of data!
With a 95% confidence interval because of the huge dataset, she found that there was one factor that reduced mortality by 26%.
And the difference was…
Whether or not patients had a chronic disease management plan set up with their GP (General Practitioner, or “family doctor”, in US terms), after their initial stroke treatment.
45% of patients had this; the other 55% did not, so again the sample size was big for both groups.
Why this is important:
After a stroke, often a patient is discharged as early as it seems safe to do so, and there’s a common view that “it just takes time” and “now we wait”. After all, no medical technology we currently have can outright repair that damage—the body must repair itself! Medications—while critical*—can only support that and help avoid recurrence.
*How critical? VERY critical. Critical critical. Dr. Andrew found, some years previously, that greater levels of medication adherence (ie, taking the correct dose on time and not missing any) significantly improved survival outcomes. No surprise, right? But what may surprise is that this held true even for patients with near-perfect adherence. In other words: miss a dose at your peril. It’s that important.
But, as Dr. Andrew’s critical research shows, that’s no reason to simply prescribe ongoing meds and otherwise cut a patient loose… or, if you or a loved one are the patient, to allow yourself/them to be left without a doctor’s ongoing active support in the form of a chronic disease management plan.
What does a chronic disease management plan look like?
First, what it’s not:
- “Yes yes, I’m here if you need me, just make an appointment if something changes”
- “Let’s pencil in a check-up in three months”
- Etc
What it actually looks like:
It looks like a plan. A personal care plan, built around that person’s individual needs, risks, liabilities… and potential complications.
Because who amongst us, especially at the age where strokes are more likely, has an uncomplicated medical record? There will always be comorbidities and confounding factors, so a one-size-fits-all plan will not do.
Dr. Andrew’s work took place in Australia, so she had the Australian healthcare system in mind… We know many of our subscribers are from North America and other places. But read this, and you’ll see how this could go just as much for the US or Canada:
❝The evidence shows the importance of Medicare financially supporting primary care physicians to provide structured chronic disease management after a stroke.
We also provide a strong case for the ongoing provision of these plans within a universal healthcare system. Strategies to improve uptake at the GP level could include greater financial incentives and mandates, education for patients and healthcare professionals.❞
See her groundbreaking study for yourself here!
The Bottom Line:
If you or a loved one has a stroke, be prepared to make sure you get a chronic health management plan in place. Note that if it’s you who has the stroke, you might forget this or be unable to advocate for yourself. So, we recommend to discuss this with a partner or close friend sooner rather than later!
“But I’m quite young and healthy and a stroke is very unlikely for me”
Good for you! And the median age of Dr. Andrew’s gargantuan study was 70 years. But:
- do you have older relatives? Be aware for them, too.
- strokes can happen earlier in life too! You don’t want to be an interesting statistic.
Some stroke-related quick facts:
Stroke is the No. 5 cause of death and a leading cause of disability in the U.S.
Stroke can happen to anyone—any age, any time—and everyone needs to know the warning signs.
On average, 1.9 million brain cells die every minute that a stroke goes untreated.
Stroke is an EMERGENCY. Call 911 immediately.
Early treatment leads to higher survival rates and lower disability rates. Calling 911 lets first responders start treatment on someone experiencing stroke symptoms before arriving at the hospital.
Source: https://www.stroke.org/en/about-stroke
What are the warning signs for stroke?
Use the letters F.A.S.T. to spot a stroke and act quickly:
- F = Face Drooping—does one side of the face droop or is it numb? Ask the person to smile. Is the person’s smile uneven?
- A = Arm Weakness—is one arm weak or numb? Ask the person to raise both arms. Does one arm drift downward?
- S = Speech Difficulty—is speech slurred?
- T = Time to call 911
Source: https://www.stroke.org/en/about-stroke/stroke-symptoms
Last but not least, while we’re sharing resources:
Download the PDF Checklist: 8 Ways To Help Prevent a Second Stroke
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why You Can’t Just “Get Over” Trauma

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Time does not, in fact, heal all wounds. Sometimes they even compound themselves over time. Dr. Tracey Marks explains the damage that trauma does—the physiological presentation of “the axe forgets but the tree remembers”—and how to heal from that actual damage.
The science of healing
Trauma affects the mind and body (largely because the brain is, of course, both—and affects pretty much everything else), which can ripple out into all areas of life.
On the physical level, brain areas affected by trauma include:
- Amygdalae: becomes hyperactive, keeping a person in a heightened state of vigilance.
- Hippocampi: can shrink, causing fragmented or missing memories.
- Prefrontal cortex: reduces in activity, impairing decision-making and emotional regulation.
Trauma also activates the body’s fight or flight response, releasing stress hormones like cortisol and adrenaline. These are great things to have a pinch, but having them elevated all the time is equivalent to only ever driving your car at top speed—the only question becomes whether you’ll crash and burn before you break down.
However, there is hope! Neuroplasticity (the brain’s ability to rewire itself) can make trauma recovery possible through various interventions.
Evidence-based therapies for trauma include:
- Eye Movement Desensitization and Reprocessing (EMDR): this can help reprocess traumatic memories and reduce emotional intensity.
- Trauma-focused Cognitive Behavioral Therapy (CBT): this can help change unhelpful thought patterns and includes exposure therapy.
- Somatic therapies: these focus on the body and nervous system to release stored tension.
In this latter category, embodiment is key to trauma recovery—this may sound “wishy-washy”, but the evidence shows that reconnecting with the body does help manage emotional stress responses. Mind-body practices like mindfulness, yoga, and breathwork help cultivate embodiment and reduce trauma-related stress.
In short: you can’t just “get over” it, but with the right support and interventions, it’s possible to rewire the brain and body toward resilience and healing.
For more on all of this from Dr. Marks, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- PTSD, But, Well…. Complex.
- Undoing The Damage Of Life’s Hard Knocks
- A Surprisingly Powerful Tool: Eye Movement Desensitization & Reprocessing
Take care!
Share This Post
-
Basil vs Cilantro – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing basil to cilantro, we picked the cilantro.
Why?
Both have their strong merits, but there can be only one winner when all’s said and done:
First, you may be thinking: these are just herbs; we don’t eat enough of these for the nutritional values to be relevant!
And to this we say: there’s nothing stopping you :p Herbs are full of flavor and goodness and there is really no reason to deny yourself. On this note, check out the sabzi khordan (traditional Levantine herb platter), linked below. You’ll start thinking about herbs in new ways, and you can thank us later!
So, onwards to the comparisons…
In terms of macros, the only relevant distinguishing factor is that cilantro has nearly 2x the fiber, so that’s a win in this category of cilantro.
In the category of vitamins, basil has more of vitamins B6, B7, B9, and K, while cilantro has more of vitamins A, B1, B2, B3, B5, C, and E, winning this round too.
Looking at minerals, however, basil has more calcium, copper, iron, magnesium, manganese, phosphorus, and zinc, while cilantro has more potassium and selenium, yielding an 8:1 win to basil in this category.
In other considerations, both are equally good sources of polyphenols, so that’s a tie in this round.
Adding up the sections makes for a clear overall win for cilantro, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
- Holy Basil: What Does (And Doesn’t) It Do? ← this is not culinary basil, but it’s an interesting read nevertheless
- 21 Most Beneficial Polyphenols & What Foods Have Them
- Invigorating Sabzi Khordan (A Traditional Levantine Platter Of Herbs & Accompaniments)
Enjoy!
Share This Post
-

Why STIs Are On The Rise In Older Adults
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Three Little Words
Sexually Transmitted Infections (STIs) are often thought of as something that predominantly plagues younger people… The truth, however, is different:
❝Rising divorce rates, forgoing condoms as there is no risk of pregnancy, the availability of drugs for sexual dysfunction, the large number of older adults living together in retirement communities, and the increased use of dating apps are likely to have contributed to the growing incidence of STIs in the over-50s.
These data likely underestimate the true extent of the problem as limited access to sexual health services for the over 50s, and trying to avoid the stigma and embarrassment both on the part of older people and healthcare professionals, is leading to this age group not seeking help for STIs.❞
Read more: Managing The Rise In STIs Among Older Adults
That said, there is a gender gap when it comes to the increased risk, for example:
❝A retrospective study from the USA involving 420,790 couples aged 67 to 99 years, found that widowhood was associated with an increased risk of STIs in older men, but not women❞
~ US Dept of Health & Human Services
Source: CDC: | Sexually Transmitted Disease Surveillance
Is abstinence the best preventative, then?
It is inarguably the most effective, but not necessarily the best for everyone.
This is because for most adults, a healthy sex life is an important part of overall wellbeing.
See also: Mythbusting The Big O
Even in this case there is a gender gap in:
- the level of importance placed on frequency of sexual interactions
- what act(s) of sexuality are held to be most important:
❝Among sexually active men, frequent (≥2 times a month) sexual intercourse (P < .001) and frequent kissing, petting, or fondling (P < .001) were associated with greater enjoyment of life.
Among sexually active women, frequent kissing, petting, or fondling was also associated with greater enjoyment of life (P < .001), but there was no significant association with frequent intercourse (P = .101).
Concerns about one’s sex life and problems with sexual function were strongly associated with lower levels of enjoyment of life in men and to a lesser extent in women.❞
Source: Sexual Activity is Associated with Greater Enjoyment of Life in Older Adults
If you have the time to go into it much more deeply, this paper from the Journal of Gerontology is much more comprehensive, looking also at related lifestyle factors, religious/political backgrounds, views on monogamy or non-monogamy (of various kinds), hormonal considerations, the impact of dementia or other long-term disabilities that may affect things, widowhood, and many other elements:
The National Social Life, Health, and Aging Project: An Introduction
What’s the best preventative, then?
Regular health screening for yourself and your partner(s) is an important key to preventative health when it comes to STIs.
You can Google search for a local STI clinic, and worry not, they are invariably discreet and are well-used to everybody coming in. They’re just glad you’re being responsible about things. It’s also not their job to judge your sexual activities, even if it’s something you might have reason to wish to be secretive about, try to be honest there.
Secondly, most of the usual advice about safe sex still goes, even when there’s no risk of pregnancy. For example, if there’s at least one penis involved, then condoms remain the #1 barrier to all manner of potential infections (we know, almost nobody likes condoms, but sometimes the truth isn’t what we want to hear).
Lastly, if there’s at least one vagina involved, then please for the love of all that is holey, do not put anything there that could cause a yeast infection.
What can cause a yeast infection? Pretty much anything with sugar, which includes but is not limited to:
- Most kinds of food that Cosmo-style “liven things up in the bedroom” advice columns might suggest using (including fruit, honey, chocolate sauce, whipped cream, etc)
- Hands that are not clean (watch out for bacteria too)
- A mouth that has recently been eating or drinking anything with sugar in it, and that includes many kinds of alcohol, as well as milk or hot drinks that had milk in
Yeast infections are not nearly so serious as the STIs the other measures are there to avoid, but they’re not fun either, so some sensible policies in that regard are always good!
On a related note, see also: How To Avoid UTIs
Recap on the single most important part of this article:
At all ages, it remains a good health practice—unless one is absolutely celibate—to regularly get oneself and one’s partner(s) checked for STIs.
Take care!
Share This Post

Related Posts
-
How Vitamin D May Help Protect Against Diabetes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
…and other items from this week’s health science news:
D vs D
Vitamin D may help protect you from diabetes… Or it may not. The science is clear on this!
In other words: the data (with a large amount of data analysis and a RCT with 2,098 people with prediabetes) is clear about the effect in general, and what that science says, is that whether or not it helps you as an individual, will depend on your genes.
Specifically:
- Participants with the AA variation of the vitamin D receptor gene showed no meaningful response when taking 4,000 IU of vitamin D daily compared with a placebo.
- Participants with AC or CC in the the vitamin D receptor gene had a 19% lower risk of developing diabetes when taking 4,000 IU of vitamin D daily compared with a placebo.
Why the genetic variation matters: vitamin D must bind to the vitamin D receptor to work in your body, and differences in this receptor—particularly in insulin-producing cells in your pancreas—will affect how well vitamin D helps regulate blood sugar.
So, this one’s a case for personalized prevention, where a simple genetic test could identify who is likely to benefit from higher vitamin D intake.
Read in full: Vitamin D may help prevent diabetes
Related: The Real Benefit Of Genetic Testing
Relighting the brain’s fire for happiness
Researchers (Dr. Alice Meuret et al.) have found that a therapy that directly targets lost pleasure (anhedonia*) improves depression and anxiety more than standard treatments that mainly reduce negative emotions.
*It’s not just about pleasure in the sense most might speak of such, though; anhedonia is the reduced or absent ability to feel positive emotions in general. It affects nearly all people with depression, and is strongly linked to worse outcomes, relapse, and suicidal risk.
The problem with standard therapies: most treatments focus on reducing sadness, fear, or distress, but largely ignore rebuilding positive emotions—even though patients often see that as their main goal.
Positive Affect Treatment (PAT), in contrast, is a 15-session psychotherapy designed to restore joy, motivation, meaning, and reward sensitivity. Specifically, it targets the brain’s reward system by encouraging engagement in meaningful activities, shifting attention towards positive experiences, and practising gratitude, savoring, and compassion-based exercises.
As for how well it works: the RCT of 98 adults with severe anhedonia, depression, and anxiety compared PAT to a conventional therapy focused on negative emotions. The results? PAT produced greater overall clinical improvement, including reductions in both depression and anxiety, even though it never directly targeted negative emotions.
Read in full: Targeting lost pleasure lifts depression and anxiety more than standard therapy, new study finds
Related: Behavioral Activation Against Depression & Anxiety
Allergy season feeling different this year?
Due to climate change, pollen seasons are starting earlier, lasting longer, and even overlapping. because of warmer temperatures and higher CO₂, which keeps your immune system in overdrive for longer and leads to more intense symptoms.
Air pollution (which is getting steadily worse in the US and likely many other places too) can also alter pollen particles, making them more irritating to your airways and increasing inflammation.
Children’s symptoms are easy to miss: kids may show allergies through mouth breathing, fatigue, irritability, sleep issues, ear infections, or dark circles under your eyes rather than clearly describing symptoms.
A very common mistake (regardless of age), is starting treatment too late, and/or using medication only when symptoms become onerous, but by this time, your immune system has already been overworked, and taking anti-allergy meds now won’t mean the already-in-progress war in your body suddenly stops instantly.
So instead, you might consider starting allergy medication before symptoms peak, and then taking it consistently for a few weeks (even if the symptoms stop, because that is what the meds are for!), to prevent your immune response from ramping up.
Read in full: Are you managing your allergies the wrong way?
Related: Antihistamines’ Generation Gap
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What Happens If Your Estrogen Gets Too High?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For most women especially of a certain age, the more common problem is too little estrogen. However, the body is weird and wonderful; sometimes the opposite can occur. Also, when it comes to hormone replacement therapy (HRT), more often people are undermedicated rather than overmedicated, but it’s worth knowing these signs even if only for reassurance purposes (i.e. if they are not present).
Too much of a good thing?
Good levels (mid-cycle if you have a cycle; stable medicated levels if medicated) are 45–750 pg/mL which is 170–2,750 pmol/L.
Gentlemen, your levels should be more like 8–35 pg/mL, which is 30–130 pmol/L.
So, unless you’re much higher than those levels, you should normally be fine. Also, if you get a blood test and it comes back with numbers very different than it normally gives, do examine if you changed anything that might explain it (e.g. biotin supplementation above a certain level can give false E2 readings), but also see if you can get a second blood test done, to see if there was simply a technical fault with the first (e.g. contaminated sample).
Signs to watch out for:
- skin pigment changes: generalized or localized hyperpigmentation, darkening of nipples and genitalia, linea nigra, darkened or new moles, and melasma (patchy discoloration on face and chest)
- vascular skin signs: estrogen increases blood flow and vessel formation, causing red palms (palmar erythema), spider angiomas (red spots with radiating lines), and telangiectasias (broken capillaries, especially on face)
- vascular symptoms beyond skin: Reynaud’s phenomenon (color changes in fingers due to vessel constriction) is sometimes associated with high estrogen levels
- stretch marks (striae): estrogen may influence stretch mark development by altering collagen structure; they can also occur with rapid weight gain, muscle growth, obesity, or fluid buildup from liver disease, so this is by no means a reliable sign
- acne and sebum: high estrogen can reduce sebum production and may improve acne in some individuals, especially with oral contraceptive use
- hair changes in women: estrogen prolongs hair growth phase (anagen), causing thicker scalp hair and sometimes increased body and facial hair during pregnancy or while using hormone therapy
- hair changes in men: men with high estrogen (by male standards) may experiencing a thinning of body hair; they might also experience breast development (gynecomastia) and testicular atrophy
For more on all of these plus some helpful visuals, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Signs Of Low Estrogen In Women: What Your Skin, Hair, & Nails Are Trying To Tell You
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
You can train your nose – and 4 other surprising facts about your sense of smell
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Would you give up your sense of smell to keep your hair? What about your phone?
A 2022 US study compared smell to other senses (sight and hearing) and personally prized commodities (including money, a pet or hair) to see what people valued more.
The researchers found smell was viewed as much less important than sight and hearing, and valued less than many commodities. For example, half the women surveyed said they’d choose to keep their hair over sense of smell.
Smell often goes under the radar as one of the least valued senses. But it is one of the first sensory systems vertebrates developed and is linked to your mental health, memory and more.
Here are five fascinating facts about your olfactory system.

DimaBerlin/Shutterstock 1. Smell is linked to memory and emotion
Why can the waft of fresh baking trigger joyful childhood memories? And why might a certain perfume jolt you back to a painful breakup?
Smell is directly linked to both your memory and emotions. This connection was first established by American psychologist Donald Laird in 1935 (although French novelist Marcel Proust had already made it famous in his reverie about the scent of madeleines baking.)
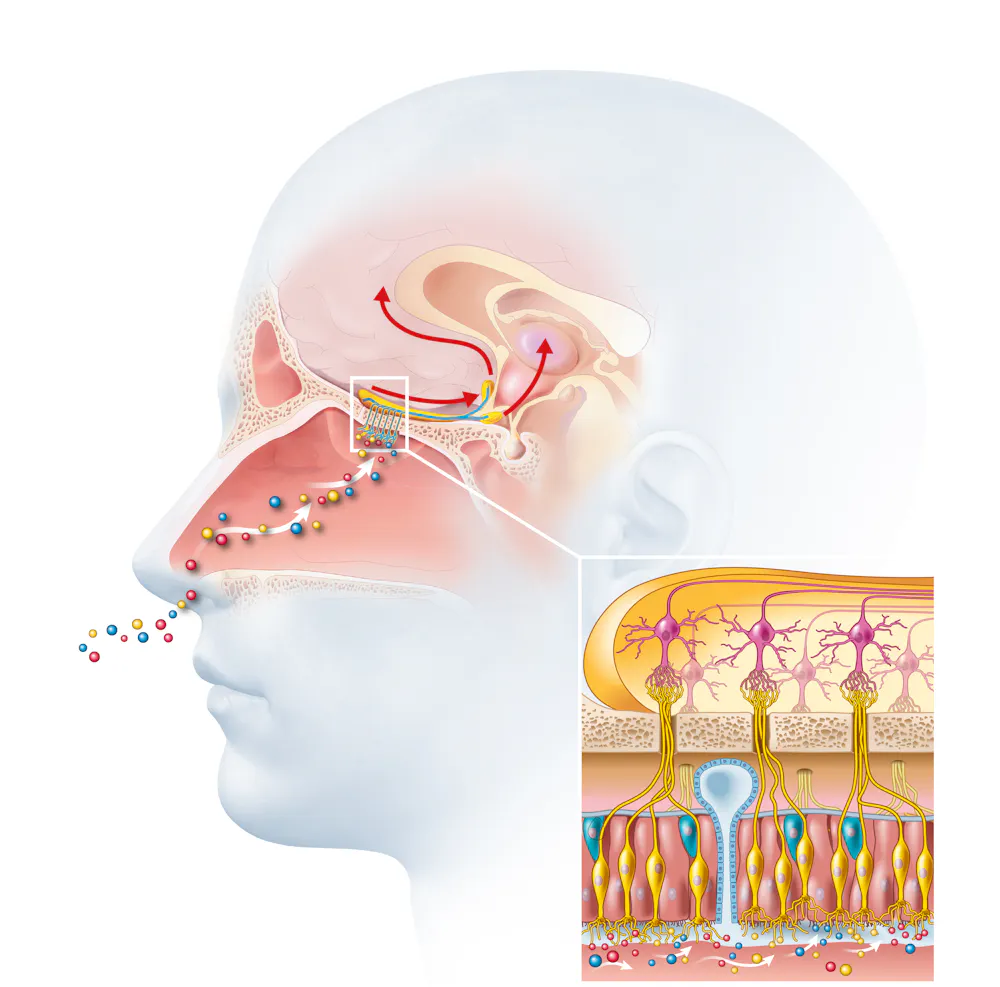
Odours are first captured by special olfactory nerve cells inside your nose. These cells extend upwards from the roof of your nose towards the smell-processing centre of your brain, called the olfactory bulb.
Smells are first detected by nerve cells in the nose. Axel_Kock/Shutterstock From the olfactory bulb they form direct connection with the brain’s limbic system. This includes the amygdala, where emotions are generated, and the hippocampus, where memories are created.
Other senses – such as sight and hearing – aren’t directly connected to the lymbic system.
One 2004 study used functional magnetic resonance imaging to demonstrate odours trigger a much stronger emotional and memory response in the brain than a visual cue.
2. Your sense of smell constantly regenerates
You can lose your ability to smell due to injury or infection – for example during and after a COVID infection. This is known as olfactory dysfunction. In most cases it’s temporary, returning to normal within a few weeks.
This is because every few months your olfactory nerve cells die and are replaced by new cells.
We’re not entirely sure how this occurs, but it likely involves your nose’s stem cells, the olfactory bulb and other cells in the olfactory nerves.
Other areas of your nervous system – including your brain and spinal cord – cannot regenerate and repair after an injury.
Constant regeneration may be a protective mechanism, as the olfactory nerves are vulnerable to damage caused by the external environment, including toxins (such as cigarette smoke), chemicals and pathogens (such as the flu virus).
But following a COVID infection some people might continue to experience a loss of smell. Studies suggest the virus and a long-term immune response damages the cells that allow the olfactory system to regenerate.
3. Smell is linked to mental health
Around 5% of the global population suffer from anosmia – total loss of smell. An estimated 15-20% suffer partial loss, known as hyposmia.
Given smell loss is often a primary and long-term symptom of COVID, these numbers are likely to be higher since the pandemic.
Yet in Australia, the prevalence of olfactory dysfunction remains surprisingly understudied.
Losing your sense of smell is shown to impact your personal and social relationships. For example, it can mean you miss out on shared eating experiences, or cause changes in sexual desire and behaviour.
In older people, declining ability to smell is associated with a higher risk of depression and even death, although we still don’t know why.
Losing your sense of smell can have a major impact on mental health. Halfpoint/Shutterstock 4. Loss of smell can help identify neurodegenerative diseases
Partial or full loss of smell is often an early indicator for a range of neurodegenerative diseases, including Alzheimer’s and Parkinson’s diseases.
Patients frequently report losing their sense of smell years before any symptoms show in body or brain function. However many people are not aware they are losing their sense of smell.
There are ways you can determine if you have smell loss and to what extent. You may be able to visit a formal smell testing centre or do a self-test at home, which assesses your ability to identify household items like coffee, wine or soap.
5. You can train your nose back into smelling
“Smell training” is emerging as a promising experimental treatment option for olfactory dysfunction. For people experiencing smell loss after COVID, it’s been show to improve the ability to detect and differentiate odours.
Smell training (or “olfactory training”) was first tested in 2009 in a German psychology study. It involves sniffing robust odours — such as floral, citrus, aromatic or fruity scents — at least twice a day for 10—20 seconds at a time, usually over a 3—6 month period.
Participants are asked to focus on the memory of the smell while sniffing and recall information about the odour and its intensity. This is believed to help reorganise the nerve connections in the brain, although the exact mechanism behind it is unclear.
Some studies recommend using a single set of scents, while others recommend switching to a new set of odours after a certain amount of time. However both methods show significant improvement in smelling.
This training has also been shown to alleviate depressive symptoms and improve cognitive decline both in older adults and those suffering from dementia.
Just like physiotherapy after a physical injury, olfactory training is thought to act like rehabilitation for your sense of smell. It retrains the nerves in your nose and the connections it forms within the brain, allowing you to correctly detect, process and interpret odours.
Lynn Nazareth, Research Scientist in Olfactory Biology, CSIRO
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: