Self-Compassion – by Dr. Kristin Neff
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of people struggle with self-esteem, and depending on one’s surrounding culture, it can even seem socially obligatory to be constantly valuing oneself highly (or else, who else will if we do not?). But, as Dr. Neff points out, there’s an inherent problem with reinforcing for oneself even a positive message like “I am smart, strong, and capable!” because sometimes all of us have moments of being stupid, weak, and incapable (occasionally all three at once!), which places us in a position of having to choose between self-deceit and self-deprecation, neither of which are good.
Instead, Dr. Neff advocates for self-compassion, for treating oneself as one (hopefully) would a loved one—seeing their/our mistakes, weaknesses, failures, and loving them/ourself anyway.
She does not, however, argue that we should accept just anything from ourselves uncritically, but rather, we identify our mistakes, learn, grow, and progress. So not “I should have known better!”, nor even “How was I supposed to know?!”, but rather, “Now I have learned a thing”.
The style of the book is quite personal, as though having a heart-to-heart over a hot drink perhaps, but the format is organized and progresses naturally from one idea to the next, taking the reader to where we need to be.
Bottom line: if you have trouble with self-esteem (as most people do), then that’s a trap that there is a way out of, and it doesn’t require being perfect or lowering one’s standards, just being kinder to oneself along the way—and this book can help inculcate that.
Click here to check out Self-Compassion, and indeed be kind to yourself!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Vagus Nerve’s Power for Weight Loss

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Arun Dhir is a university lecturer, a gastrointestinal surgeon, an author, and a yoga and meditation instructor, and he has this to say:
Gut feelings
The vagus nerve is the 10th cranial nerve, also known as “vagus” (“the wanderer”), because it travels from the brain to many other body parts, including the ears, throat, heart, respiratory system, gut, pancreas, liver, and reproductive system. It’s no surprise then, that it plays a key role in brain-gut communication and metabolism regulation.
The vagus nerve is part of the parasympathetic nervous system, responsible for rest, digestion, and counteracting the stress response. Most signals through the vagus nerve travel from the gut to the brain, though there is communication in both directions.
You may be beginning to see how this works and its implications for weight management: the vagus nerve senses metabolites from the liver, pancreas, and small intestine, and regulates insulin production by stimulating beta cells in the pancreas, which is important for avoiding/managing insulin resistance and metabolic syndrome in general.
Dr. Dhir cites a study in which vagus nerve stimulation (originally used for treating epilepsy and depression) was shown to cause unintentional weight loss (6-11%) in patients, revealing a link to weight management. Of course, that is quite a specific sample, so more research is needed to say for sure, but because the principle is very sound and the mechanism of action is clear, it’s not being viewed as a controversial conclusion.
As for how get these benefits, here are seven ways:
- Cold water on the face: submerge your face in cold water in the morning while holding water in your mouth, or cover your face with a cold wet washcloth (while holding your breath please; no need to waterboard yourself!), which activates the “mammalian dive response” in which your body activates the parasympathetic nervous system in order to remain calm and thus survive for longer underwater
- Alternate hot and cold showers: switch between hot and cold water during showers for 10-second intervals; this creates eustress and activates the process of hormesis, improving your overall stress management and reducing any chronic stress response you may otherwise have going on
- Humming and gargling: the vibrations in the throat stimulate the nearby vagus nerve
- Deep breathing (pranayama): yoga breathing exercises, especially combined with somatic exercises such as the sun salutation, can stimulate the vagus nerve
- Intermittent fasting: helps recalibrate the metabolism and indirectly improves vagus nerve function
- Massage and acupressure: stimulates lymphatic channels and the vagus nerve
- Long walks in nature (“forest bathing”): helps trigger relaxation in general
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The Vagus Nerve (And How You Can Make Use Of It)
Take care!
Share This Post
-
Oats vs Rye – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing oats to rye, we picked the oats.
Why?
It was close!
In terms of macros, oats have a little more protein and rye has a little more fiber, and we’ll call this first round a tie on the strength of those.
In the category of vitamins, oats have more of vitamins B1, B7, and B9, while rye has more of vitamins B2, B3, and B6—another tie!
Looking at minerals, this time we have something to set one ahead of the other: oats have more calcium, copper, iron, magnesium, manganese, phosphorus, selenium, and zinc, while rye has just a little more potassium. An easy win for oats in this round.
Adding up the sections makes for an overall win for oats, but both are great, so by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
The Best Kind Of Fiber For Overall Health? ← it’s β-glucan, the kind find abundantly in oats!
Enjoy!
Share This Post
-
Having an x-ray to diagnose knee arthritis might make you more likely to consider potentially unnecessary surgery
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Osteoarthritis is a leading cause of chronic pain and disability, affecting more than two million Australians.
Routine x-rays aren’t recommended to diagnose the condition. Instead, GPs can make a diagnosis based on symptoms and medical history.
Yet nearly half of new patients with knee osteoarthritis who visit a GP in Australia are referred for imaging. Osteoarthritis imaging costs the health system A$104.7 million each year.
Our new study shows using x-rays to diagnose knee osteoarthritis can affect how a person thinks about their knee pain – and can prompt them to consider potentially unnecessary knee replacement surgery.

pikselstock/Shutterstock What happens when you get osteoarthritis?
Osteoarthritis arises from joint changes and the joint working extra hard to repair itself. It affects the entire joint, including the bones, cartilage, ligaments and muscles.
It is most common in older adults, people with a high body weight and those with a history of knee injury.
Many people with knee osteoarthritis experience persistent pain and have difficulties with everyday activities such as walking and climbing stairs.
How is it treated?
In 2021–22, more than 53,000 Australians had knee replacement surgery for osteoarthritis.
Hospital services for osteoarthritis, primarily driven by joint replacement surgery, cost $3.7 billion in 2020–21.
While joint replacement surgery is often viewed as inevitable for osteoarthritis, it should only be considered for those with severe symptoms who have already tried appropriate non-surgical treatments. Surgery carries the risk of serious adverse events, such as blood clot or infection, and not everyone makes a full recovery.
Most people with knee osteoarthritis can manage it effectively with:
- education and self-management
- exercise and physical activity
- weight management (if necessary)
- medicines for pain relief (such as paracetamol and non-steroidal anti-inflammatory drugs).
Debunking a common misconception
A common misconception is that osteoarthritis is caused by “wear and tear”.
However, research shows the extent of structural changes seen in a joint on an x-ray does not reflect the level of pain or disability a person experiences, nor does it predict how symptoms will change.
Some people with minimal joint changes have very bad symptoms, while others with more joint changes have only mild symptoms. This is why routine x-rays aren’t recommended for diagnosing knee osteoarthritis or guiding treatment decisions.
Instead, guidelines recommend a “clinical diagnosis” based on a person’s age (being 45 years or over) and symptoms: experiencing joint pain with activity and, in the morning, having no joint-stiffness or stiffness that lasts less than 30 minutes.
Despite this, many health professionals in Australia continue to use x-rays to diagnose knee osteoarthritis. And many people with osteoarthritis still expect or want them.
What did our study investigate?
Our study aimed to find out if using x-rays to diagnose knee osteoarthritis affects a person’s beliefs about osteoarthritis management, compared to a getting a clinical diagnosis without x-rays.
We recruited 617 people from across Australia and randomly assigned them to watch one of three videos. Each video showed a hypothetical consultation with a general practitioner about knee pain.
People with knee osteoarthritis can have difficulties getting down stairs. beeboys/Shutterstock One group received a clinical diagnosis of knee osteoarthritis based on age and symptoms, without being sent for an x-ray.
The other two groups had x-rays to determine their diagnosis (the doctor showed one group their x-ray images and not the other).
After watching their assigned video, participants completed a survey about their beliefs about osteoarthritis management.
What did we find?
People who received an x-ray-based diagnosis and were shown their x-ray images had a 36% higher perceived need for knee replacement surgery than those who received a clinical diagnosis (without x-ray).
They also believed exercise and physical activity could be more harmful to their joint, were more worried about their condition worsening, and were more fearful of movement.
Interestingly, people were slightly more satisfied with an x-ray-based diagnosis than a clinical diagnosis.
This may reflect the common misconception that osteoarthritis is caused by “wear and tear” and an assumption that the “damage” inside the joint needs to be seen to guide treatment.
What does this mean for people with osteoarthritis?
Our findings show why it’s important to avoid unnecessary x-rays when diagnosing knee osteoarthritis.
While changing clinical practice can be challenging, reducing unnecessary x-rays could help ease patient anxiety, prevent unnecessary concern about joint damage, and reduce demand for costly and potentially unnecessary joint replacement surgery.
It could also help reduce exposure to medical radiation and lower health-care costs.
Previous research in osteoarthritis, as well as back and shoulder pain, similarly shows that when health professionals focus on joint “wear and tear” it can make patients more anxious about their condition and concerned about damaging their joints.
If you have knee osteoarthritis, know that routine x-rays aren’t needed for diagnosis or to determine the best treatment for you. Getting an x-ray can make you more concerned and more open to surgery. But there are a range of non-surgical options that could reduce pain, improve mobility and are less invasive.
Belinda Lawford, Senior Research Fellow in Physiotherapy, The University of Melbourne; Kim Bennell, Professor of Physiotherapy, The University of Melbourne; Rana Hinman, Professor in Physiotherapy, The University of Melbourne, and Travis Haber, Postdoctoral Research Fellow in Physiotherapy, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-

This salt alternative could help reduce blood pressure. So why are so few people using it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One in three Australian adults has high blood pressure (hypertension). Excess salt (sodium) increases the risk of high blood pressure so everyone with hypertension is advised to reduce salt in their diet.
But despite decades of strong recommendations we have failed to get Australians to cut their intake. It’s hard for people to change the way they cook, season their food differently, pick low-salt foods off the supermarket shelves and accept a less salty taste.
Now there is a simple and effective solution: potassium-enriched salt. It can be used just like regular salt and most people don’t notice any important difference in taste.
Switching to potassium-enriched salt is feasible in a way that cutting salt intake is not. Our new research concludes clinical guidelines for hypertension should give patients clear recommendations to switch.
What is potassium-enriched salt?
Potassium-enriched salts replace some of the sodium chloride that makes up regular salt with potassium chloride. They’re also called low-sodium salt, potassium salt, heart salt, mineral salt, or sodium-reduced salt.
Potassium chloride looks the same as sodium chloride and tastes very similar.
Potassium-enriched salt works to lower blood pressure not only because it reduces sodium intake but also because it increases potassium intake. Insufficient potassium, which mostly comes from fruit and vegetables, is another big cause of high blood pressure.
What is the evidence?
We have strong evidence from a randomised trial of 20,995 people that switching to potassium-enriched salt lowers blood pressure and reduces the risks of stroke, heart attacks and early death. The participants had a history of stroke or were 60 years of age or older and had high blood pressure.
An overview of 21 other studies suggests much of the world’s population could benefit from potassium-enriched salt.
The World Health Organisation’s 2023 global report on hypertension highlighted potassium-enriched salt as an “affordable strategy” to reduce blood pressure and prevent cardiovascular events such as strokes.
What should clinical guidelines say?
We teamed up with researchers from the United States, Australia, Japan, South Africa and India to review 32 clinical guidelines for managing high blood pressure across the world. Our findings are published today in the American Heart Association’s journal, Hypertension.
We found current guidelines don’t give clear and consistent advice on using potassium-enriched salt.
While many guidelines recommend increasing dietary potassium intake, and all refer to reducing sodium intake, only two guidelines – the Chinese and European – recommend using potassium-enriched salt.
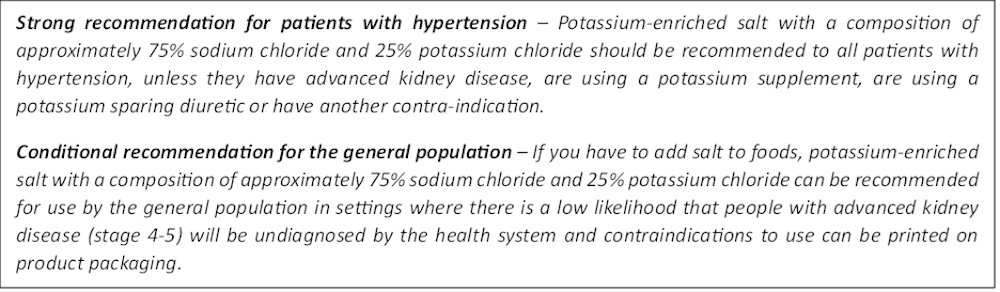
To help guidelines reflect the latest evidence, we suggested specific wording which could be adopted in Australia and around the world:
Recommended wording for guidance about the use of potassium-enriched salt in clinical management guidelines. Why do so few people use it?
Most people are unaware of how much salt they eat or the health issues it can cause. Few people know a simple switch to potassium-enriched salt can help lower blood pressure and reduce the risk of a stroke and heart disease.
Limited availability is another challenge. Several Australian retailers stock potassium-enriched salt but there is usually only one brand available, and it is often on the bottom shelf or in a special food aisle.
Potassium-enriched salts also cost more than regular salt, though it’s still low cost compared to most other foods, and not as expensive as many fancy salts now available.
It looks and tastes like normal salt.
Jimmy Dean/UnsplashA 2021 review found potassium-enriched salts were marketed in only 47 countries and those were mostly high-income countries. Prices ranged from the same as regular salt to almost 15 times greater.
Even though generally more expensive, potassium-enriched salt has the potential to be highly cost effective for disease prevention.
Preventing harm
A frequently raised concern about using potassium-enriched salt is the risk of high blood potassium levels (hyperkalemia) in the approximately 2% of the population with serious kidney disease.
People with serious kidney disease are already advised to avoid regular salt and to avoid foods high in potassium.
No harm from potassium-enriched salt has been recorded in any trial done to date, but all studies were done in a clinical setting with specific guidance for people with kidney disease.
Our current priority is to get people being managed for hypertension to use potassium-enriched salt because health-care providers can advise against its use in people at risk of hyperkalemia.
In some countries, potassium-enriched salt is recommended to the entire community because the potential benefits are so large. A modelling study showed almost half a million strokes and heart attacks would be averted every year in China if the population switched to potassium-enriched salt.
What will happen next?
In 2022, the health minister launched the National Hypertension Taskforce, which aims to improve blood pressure control rates from 32% to 70% by 2030 in Australia.
Potassium-enriched salt can play a key role in achieving this. We are working with the taskforce to update Australian hypertension management guidelines, and to promote the new guidelines to health professionals.
In parallel, we need potassium-enriched salt to be more accessible. We are engaging stakeholders to increase the availability of these products nationwide.
The world has already changed its salt supply once: from regular salt to iodised salt. Iodisation efforts began in the 1920s and took the best part of 100 years to achieve traction. Salt iodisation is a key public health achievement of the last century preventing goitre (a condition where your thyroid gland grows larger) and enhancing educational outcomes for millions of the poorest children in the world, as iodine is essential for normal growth and brain development.
The next switch to iodised and potassium-enriched salt offers at least the same potential for global health gains. But we need to make it happen in a fraction of the time.

Xiaoyue Xu (Luna), Scientia Lecturer, UNSW Sydney; Alta Schutte, SHARP Professor of Cardiovascular Medicine, UNSW Sydney, and Bruce Neal, Executive Director, George Institute Australia, George Institute for Global Health
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Why is pain so exhausting?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One of the most common feelings associated with persisting pain is fatigue and this fatigue can become overwhelming. People with chronic pain can report being drained of energy and motivation to engage with others or the world around them.
In fact, a study from the United Kingdom on people with long-term health conditions found pain and fatigue are the two biggest barriers to an active and meaningful life.
But why is long-term pain so exhausting? One clue is the nature of pain and its powerful effect on our thoughts and behaviours.
simona pilolla 2/Shutterstock Short-term pain can protect you
Modern ways of thinking about pain emphasise its protective effect – the way it grabs your attention and compels you to change your behaviour to keep a body part safe.
Try this. Slowly pinch your skin. As you increase the pressure, you’ll notice the feeling changes until, at some point, it becomes painful. It is the pain that stops you squeezing harder, right? In this way, pain protects us.
When we are injured, tissue damage or inflammation makes our pain system become more sensitive. This pain stops us from mechanically loading the damaged tissue while it heals. For instance, the pain of a broken leg or a cut under our foot means we avoid walking on it.
The concept that “pain protects us and promotes healing” is one of the most important things people who were in chronic pain tell us they learned that helped them recover.
But long-term pain can overprotect you
In the short term, pain does a terrific job of protecting us and the longer our pain system is active, the more protective it becomes.
But persistent pain can overprotect us and prevent recovery. People in pain have called this “pain system hypersensitivity”. Think of this as your pain system being on red alert. And this is where exhaustion comes in.
When pain becomes a daily experience, triggered or amplified by a widening range of activities, contexts and cues, it becomes a constant drain on one’s resources. Going about life with pain requires substantial and constant effort, and this makes us fatigued.
About 80% of us are lucky enough to not know what it is like to have pain, day in day out, for months or years. But take a moment to imagine what it would be like.
Imagine having to concentrate hard, to muster energy and use distraction techniques, just to go about your everyday tasks, let alone to complete work, caring or other duties.
Whenever you are in pain, you are faced with a choice of whether, and how, to act on it. Constantly making this choice requires thought, effort and strategy.
Mentioning your pain, or explaining its impact on each moment, task or activity, is also tiring and difficult to get across when no-one else can see or feel your pain. For those who do listen, it can become tedious, draining or worrying.
Concentrating hard, mustering energy and using distraction techniques can make everyday life exhausting. PRPicturesProduction/Shutterstock No wonder pain is exhausting
In chronic pain, it’s not just the pain system on red alert. Increased inflammation throughout the body (the immune system on red alert), disrupted output of the hormone cortisol (the endocrine system on red alert), and stiff and guarded movements (the motor system on red alert) also go hand in hand with chronic pain.
Each of these adds to fatigue and exhaustion. So learning how to manage and resolve chronic pain often includes learning how to best manage the over-activation of these systems.
Loss of sleep is also a factor in both fatigue and pain. Pain causes disruptions to sleep, and loss of sleep contributes to pain.
In other words, chronic pain is seldom “just” pain. No wonder being in long-term pain can become all-consuming and exhausting.
What actually works?
People with chronic pain are stigmatised, dismissed and misunderstood, which can lead to them not getting the care they need. Ongoing pain may prevent people working, limit their socialising and impact their relationships. This can lead to a descending spiral of social, personal and economic disadvantage.
So we need better access to evidence-based care, with high-quality education for people with chronic pain.
There is good news here though. Modern care for chronic pain, which is grounded in first gaining a modern understanding of the underlying biology of chronic pain, helps.
The key seems to be recognising, and accepting, that a hypersensitive pain system is a key player in chronic pain. This makes a quick fix highly unlikely but a program of gradual change – perhaps over months or even years – promising.
Understanding how pain works, how persisting pain becomes overprotective, how our brains and bodies adapt to training, and then learning new skills and strategies to gradually retrain both brain and body, offers scientifically based hope; there’s strong supportive evidence from clinical trials.
Every bit of support helps
The best treatments we have for chronic pain take effort, patience, persistence, courage and often a good coach. All that is a pretty overwhelming proposition for someone already exhausted.
So, if you are in the 80% of the population without chronic pain, spare a thought for what’s required and support your colleague, friend, partner, child or parent as they take on the journey.
More information about chronic pain is available from Pain Revolution.
Michael Henry, Physiotherapist and PhD candidate, Body in Mind Research Group, University of South Australia and Lorimer Moseley, Professor of Clinical Neurosciences and Foundation Chair in Physiotherapy, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How autoimmune encephalitis disrupts thinking, memory and everyday life
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have you ever found yourself searching for a word you should know, forgetting what you were just doing, or feeling mentally foggy for no obvious reason?
These everyday lapses are common and are most often a normal part of life, or a sign we might be tired or stressed. But for some people, they could be early signs of a rare condition called autoimmune encephalitis. This is when the body’s own immune system mistakenly attacks the brain and causes inflammation and swelling.
It can happen suddenly and at any age. Sometimes it follows a viral infection, but in many cases, the exact cause is unknown.
Autoimmune encephalitis is rare, affecting up to roughly 14 people in 100,000 each year. However, as awareness and testing improve, doctors are realising it’s more common than once thought.
So, what are the signs of autoimmune encephalitis, and how is it treated?
Natalia Lebedinskaia/Getty What does it do to the brain?
Autoimmune encephalitis causes inflammation that disrupts normal brain function, affecting how people think, remember and process information.
The inflammation often begins in the limbic system – the part of the brain that regulates emotions and forms memories. From there, inflammation can spread along connected brain networks, disrupting attention, language and planning.
Symptoms can range from striking changes – such as seizures, personality changes and hallucinations – to subtler difficulties, including confusion, forgetfulness, trouble focusing and feeling mentally slower.
These changes may come and go, or seem like stress or fatigue. Over time, they can make everyday life significantly more difficult.
As symptoms are not always visible, they are easily overlooked, resulting in delays or misdiagnosis.
MRI scans may reveal signs of swelling or inflammation, but many people have normal results in the disease’s early stages.
PET scans, which are able to measure changes in brain activity or microscopic inflammation, can sometimes detect these changes sooner.
The toll on everyday life and relationships
A 2023 Australian study of 50 people with autoimmune encephalitis found those with the disease often struggle with:
- concentration and attention
- short-term memory
- processing speed (how quickly they can take in and respond to information)
- planning, organising and decision-making (known as executive function).
This can make daily tasks such as following a conversation, writing an email or managing a schedule feel exhausting. Some people say they feel like a completely different person after becoming ill – more anxious, less confident and mentally foggy.
Nearly a third of people with this condition don’t return to work or study because of ongoing difficulties with thinking and emotions. Others may return, but need modified duties or extra time to complete tasks.
Cognitive problems can also affect relationships. Family and friends may not always understand what’s changed, especially if the person “looks fine”.
This disconnect can lead to frustration and isolation. Caregivers often carry the emotional load while trying to navigate a condition that’s still not widely understood.
It’s often misdiagnosed
One of the biggest challenges with autoimmune encephalitis is how often it’s misdiagnosed.
Its cognitive symptoms are commonly mistaken for depression, anxiety, chronic fatigue or early dementia.
There isn’t one single test that confirms autoimmune encephalitis. Many people will have multiple appointments and tests before doctors can determine exactly what’s happening. These might include:
- blood and spinal fluid tests to look for signs of inflammation or specific antibodies that target the brain
- MRI and PET brain scans to detect inflammation or changes in brain activity
- an electroencephalogram (EEG) to identify abnormal electrical activity or seizure patterns
- cognitive tests to assess thinking, attention, memory and problem-solving.
In some cases, the diagnosis is made based on symptoms and supportive findings even before antibody results are available – which can take time.
How is it treated?
Delays in diagnosis can cause further brain injury, as inflammation keeps progressing. So early treatment is key to reduce inflammation, reverse symptoms and help prevent long-term effects.
Treatment often combines:
- medications, such as steroids to reduce inflammation or immunoglobulin to calm the immune response
- anti-seizure medications, if the person experiences seizures
- cognitive rehabilitation, such as cognitive exercises, to help with thinking and memory
- psychological support, such as cognitive behavioural therapy, to deal with emotional changes.
Researchers are also developing better ways to assess and track symptoms, including self-report questionnaires and formal cognitive testing. These are essential for personalising treatment and measuring progress.
Recovery looks different for everyone
Many people can make a full recovery – especially when treatment starts early – but not everyone does. Some people with autoimmune encephalitis may recover quickly, while others take months or years to feel like themselves again.
Support makes a huge difference. People are more likely to recover well and rebuild confidence and independence when they have flexible school or work arrangements, access to therapy, and a support system that understands what they’re going through.
Living with a condition that affects your thinking can create a great sense of frustration. Because it’s not always visible to others, it can lead to isolation or self-doubt.
So mental health care is also vital. Counselling or peer support groups can provide much-needed emotional support and practical tips.
The takeaway
Autoimmune encephalitis is rare and its symptoms can overlap with many other, far more common conditions.
If you’re worried about yourself or a loved one, it’s best to speak first with your GP. They can arrange blood tests and refer you to a neurologist for further assessment if needed.
Katherine Y. Ko, Postdoctoral Research Fellow in Neuroscience, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: