Science of Yoga – by Ann Swanson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are a lot of yoga books out there to say “bend this way, hold this that way” and so forth, but few that really explain what is going on, how, and why. And understanding those things is of course key to motivation and adherence. So that’s what this book provides!
The book is divided into sections, and in the first part we have a tour of human anatomy and physiology. This may seem almost unrelated to yoga, but is valuable necessary-knowledge to get the most out of the next section:
The next few parts are given over to yoga asanas (stretches, positions, poses, call them what you will in English) and now we are given a clear idea of what it is doing: we get to understand exactly what’s being stretched, what blood flow is being increased and how, what organs are being settled into their correct place, and many other such things.
Importantly, this means we also understand why certain things are the way they are, and why they can’t be done in some other slightly different but perhaps superficially easier way.
The style of the book is like a school textbook, really, but without patronizing the reader. The illustrations, of which there are many, are simple enough to be clear while being detailed enough to be informative.
Bottom line: if you’re ever doing yoga at home and wondering if you should cut a certain corner, this is the book that will tell you why you shouldn’t.
Click here to check out Science of Yoga, and optimize your practice!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Mythbusting Moldy Food

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most Food Should Not Be Fuzzy
In yesterday’s newsletter, we asked you for your policy when it comes to mold on food (aside from intentional mold, e.g. blue cheese etc), and the responses were interesting:
- About 49% said “throw the whole thing away no matter what it is; it is dangerous”
- About 24% said “cut the mold off and eat the rest of whatever it is”
- The remainder were divided equally between “eat it all; keep the immune system on its toes” and “cut the mold off bread, but moldy animal products are dangerous”
So what does the science say?
Some molds are safe to eat: True or False?
True! We don’t think this is contentious so we’ll not spend much time on it, but just for the sake of being methodical: foods that are supposed to have mold on, including many kinds of cheese and even some kinds of cured meat (salami is an example; that powdery coating is mold).
We could give a big list of safe and unsafe molds, but that would be a list of names and let’s face it, they don’t introduce themselves by name.
However! The litmus test of “is it safe to eat” is:
Did you acquire it with this mold already in place and exactly as expected and advertised?
- If so, it is safe to eat (unless you have an allergy or such)
- If not, it is almost certainly not safe to eat
(more on why, later)
The “sniff test” is a good way to tell if moldy food is bad: True or False?
False. Very false. Because of how the sense of smell works.
You may feel like smell is a way of knowing about something at a distance, but the only way you can smell something is if particles of it are physically connecting with your olfactory receptors inside you. Yes, that has unfortunate implications about bathroom smells, but for now, let’s keep our attention in the kitchen.
If you sniff a moldy item of food, you will now have its mold spores inside your respiratory system. You absolutely do not want them there.
If we cut off the mold, the rest is safe to eat: True or False?
True or False, depending on what it is:
- Hard vegetables (e.g carrots, cabbage), and hard cheeses (e.g. Gruyère, Gouda) – cut off with an inch margin, and it should be safe
- Soft vegetables (e.g. tomatoes, and any vegetables that were hard but are now soft after cooking) – discard entirely; it is unsafe
- Anything else – discard entirely; it is unsafe
The reason for this is because in the case of the hard products mentioned, the mycelium roots of the mold cannot penetrate far.
In the case of the soft products mentioned, the surface mold is “the tip of the iceberg”, and the mycelium roots, which you will not usually be able to see, will penetrate the rest of it.
“Anything else” seems like quite a sweeping statement, but fruits, soft cheeses, yogurt, liquids, jams and jellies, cooked grains and pasta, meats, and yes, bread, are all things where the roots can penetrate deeply and easily. Regardless of you only being able to see a small amount, the whole thing is probably moldy.
The USDA has a handy downloadable factsheet:
Molds On Food: Are They Dangerous?
Eating a little mold is good for the immune system: True or False?
False, generally. There are of course countless types of mold, but not only are many of them pathogenic (mycotoxins), but also, a food that has mold will usually also have pathogenic bacteria along with the mold.
See for example: Occurrence, Toxicity, and Analysis of Major Mycotoxins in Food
Food poisoning will never make you healthier.
But penicillin is safe to eat: True or False?
False, and also penicillin is not the mold on your bread (or other foods).
Penicillin, an antibiotic* molecule, is produced by some species of Penicillium sp., a mold. There are hundreds of known species of Penicillium sp., and most of them are toxic, usually in multiple ways. Take for example:
Penicillium roqueforti PR toxin gene cluster characterization
*it is also not healthy to consume antibiotics unless it is seriously necessary. Antibiotics will wipe out most of your gut’s “good bacteria”, leaving you vulnerable. People have died from C. diff infections for this reason. So obviously, if you really need to take antibiotics, take them as directed, but if not, don’t.
See also: Four Ways Antibiotics Can Kill You
One last thing…
It may be that someone reading this is thinking “I’ve eaten plenty of mold, and I’m fine”. Or perhaps someone you tell about this will say that.
But there are two reasons this logic is flawed:
- Survivorship bias (like people who smoke and live to 102; we just didn’t hear from the 99.9% of people who smoke and die early)
- Being unaware of illness is not being absent of illness. Anyone who’s had an alarming diagnosis of something that started a while ago will know this, of course. It’s also possible to be “low-level ill” often and get used to it as a baseline for health. It doesn’t mean it’s not harmful for you.
Stay safe!
Share This Post
-

How Regularity Of Sleep Can Be Even More Important Than Duration
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A recent, large (n=72,269) 8-year prospective* observational study of adults aged 40-79 has found an association between irregular sleep and major cardiovascular events.
*this means they started the study at a given point, and measured what happened for the next eight years—as opposed to a retrospective study, which would look at what had happened during the previous 8 years.
As to what qualifies as major cardiovascular events, they counted:
- Heart attack
- Cardiac arrest
- Stroke
- Cardiovascular death (any)
Irregular sleep, meanwhile, was defined per a bell curve of participants. Based on a sleep regularity index (SRI) score, those with a score of 87 or more were on the “regular” side of the curve, and those with a score of 72 or lower were on the “irregular” side of the curve.
What they found is that irregular sleep is associated with major cardiovascular events, regardless of the actual amount of sleep that people got. So in other words, you could be sleeping 9 hours per day, but if it’s a different 9 hours each day, your cardiovascular risk will still be higher.
How much higher?
- For those in the middle of the curve (so, moderate irregularity), it was 8% higher than those on the “regular” side.
- For those on the “irregular” side of the curve, it was 26% higher than those on the “regular” side.
All of the above is after taking into account confounding variables such as age, physical activity levels, discretionary screen time, fruit, vegetable, and coffee intake, alcohol consumption, smoking, mental health issues, medication use, and shift work. Which is quite something, given that shift work is a very common reason for irregular sleep schedules in a lot of people.
Limitations
While, as noted above, they did their best to account for a lot of things, this was an observational study, not an interventional study or a randomized controlled trial, and as such, it cannot truly establish cause and effect.
For example, an observational study in the 90s found that the sport most strongly associated with longevity was polo. For any unfamiliar, it’s a game played on horseback with mallets and balls. Why was this game so much better than, say, swimming? And the answer is most likely that polo is played almost entirely by very rich people. It wasn’t the sport that enhanced longevity—it was the wealth.
So similarly here, it could be for example that people who are predisposed to heart conditions, are prone to having irregular schedules. We won’t know for sure until we have interventional studies (and we probably can’t get RCTs for this, for practical reasons).
Still, it seems likely that the association is indeed causal, in which case, having a regular sleep schedule if at all possible seems like a very good way to look after one’s health.
You can read more about the study here:
Irregular sleep may elevate risk of major cardiovascular events
Practical take-away
This study strongly suggests that sleep regularity is even more important than sleep duration.
This means that there is extra reason to not sleep in past one’s normal getting-up time, even if one had a less restful night.
That’s the end of sleep that’s the most important in practical terms, too, because we can control our getting-up time, whereas we can’t really control our going-to-sleep time, because it’s perfectly possible to just lie there awake.
So, controlling the getting-up time is really the key to the whole thing. See also:
Calculate (And Enjoy) The Perfect Night’s Sleep
And for scope, you might enjoy reading:
Morning Larks vs Night Owls: How Much Can We Control Our Sleep Schedule?
Enjoy!
Share This Post
-

Curing Hiccups And Headaches At Home With Actual Science
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Quick fixes for bodily annoyances
Do you ever find yourself desperately trying to cure hiccups, and advice on the Internet is like “breathe in through your ears while drinking vinegar upside-down through your nose”?
If so, you’re not alone. So, today we’re going to look at some science-based approaches to dealing with common bodily annoyances.
Hiccups
Unfortunately, most popular advices simply don’t work, and the only near-guaranteed way to cure these is with anti-convulsive medications whose side-effects may be worse than the hiccups.
However, before you head to the pharmacy, there is one breathing exercise that has a very simple scientific underpinning: 4:4 breathing. If you’re unfamiliar, it’s just:
- Breathe slowly in through your nose to a count of four
- Hold your breath for a count of four
- Breathe slowly out through your nose to a count of four
- Hold your breath for a count of four
…and repeat. The slower the better. At first, your hiccups will interrupt this, but just “keep calm and carry on”.
The reason this can work is that breathing is an autonomic function (e.g., it happens without us thinking about it) that, unlike most other autonomic functions, we can all control directly. By taking control of one, others will tend to fall into line with it.
For example, it is normal that your heart rate will tend to slow or quicken as your breathing slows or quickens, respectively.
Your hiccups? Autonomic function. Actually a very, very old evolutionary left-over trait, that’s only useful for protecting lungs while breathing underwater. In other words, it’s the bodily function thinks you’re a fish (or a tadpole-like amphibious creature) in the process of developing lungs. Unfortunately, because hiccuping doesn’t harm our chances of passing on our genes, it never got naturally de-selected so we still have it.
Anyway, the bottom line is: take control of your breathing in the aspects you can directly control, and the aspects you can’t directly control will fall into line. You may need to give it some minutes, don’t give up too quickly.
Headaches
If you ever get a headache and you don’t have painkillers or perhaps they’re not helping or you have another reason for not wanting to take them, there’s “one quick trick” that can cure most headaches in seconds.
First, the limitation: this will only cure headaches that have been caused by increased localized blood pressure in the forehead. However, that’s more than half of most common headaches.
Next, how it works…
We’re mentioning this first, because understanding how it works will give you more confidence in using it.
Your body has a wonderful homeostatic system, which is the system by which your body maintains its “Goldilocks zones” of not too hot or cold, not to acidine or alkaline, not too hydrated or dehydrated, blood pressure not too high or too low, etc. Sometimes, however, it can get confused, and needs a nudge back to where it should be.
One of the ways it maintains blood pressure is biofeedback from receptors in blood vessel walls, called baroreceptors. They are what it sounds like; they measure blood pressure internally.
In certain places, there are clusters of baroreceptors in one place. And if we press on that one place, the body will think “Oh no! Super high blood pressure in this bit!” and reduce the blood pressure immediately.
This is called the baroreflex, and that’s what you need to cure a hypertensive headache.
So, what to do:
With your thumb, carefully feel the upper inside corner of your eye socket. So, at the top, and about ¼ of the way out from the bridge of your nose. You should feel a groove. No, not like the Emperor’s New, but, an actual groove in your eye socket. That’s the supraorbital notch (or foramen), and it allows the supraorbital artery, veins, and nerve to run through.
Press it firmly (you can do both sides at once, assuming you have two thumbs) for about three seconds, and then massage it gently. Repeat as necessary, but it shouldn’t take more than about three goes to have cured the headache.
As a bonus, this is a great party trick for curing other people’s headaches, when the need arises!
Share This Post
Related Posts
-

Turmeric (Curcumin) Dos and Don’ts With Dr. Kim
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Turmeric is a fabulous spice, most well-known for its anti-inflammatory powers; its antioxidant effects benefit all of the body, including the brain. While it fights seemingly everything from arthritis to atherosclerosis to Alzheimer’s and more, it also boosts brain-derived neurotrophic factor, looks after your cardiovascular health, holds back diabetes, reduces the risk of cancer, fights depression, slows aging, and basically does everything short of making you sing well too.
Dr. Leonid Kim goes over the scientific evidence for these, and also talks about some of the practicalities of taking turmeric, and safety considerations.
For the most part, turmeric is very safe even at high doses (up to 8g at least); indeed, at smaller doses (e.g. 500mg) it largely does the same job as non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, with fewer problems.
It also does the job of several antidiabetic medications, by increasing uptake of glucose (thus reducing blood sugar levels) while simultaneously decreasing the glucose secretion from the liver. It does this by regulating the AMPK signalling pathway, just like metformin—while again, being safer.
Dr. Kim also looks at the (good!) evidence for turmeric in managing PCOS and undoing NAFLD; so far, so good.
Dosage: he bids us pay attention whether we’re taking it as turmeric itself or as curcumin standardized extract. The latter is the active compound, and in principle more powerful, but in practice it can get metabolized too quickly and easily—before it can have its desired effect. So, turmeric itself is a very good choice.
Absorption: since we do want it to be absorbed well, though, he does recommend taking it with piperine (as in black pepper).
You may be thinking: isn’t this going to cause the same problem you were just talking about, and cause it to be metabolized too quickly? And the answer is: no! How piperine works is almost the opposite; it protects the curcumin in the turmeric from our digestive enzymes, and thus allows them to get absorbed without being broken down too quickly—thus increasing the bioavailability by slowing the process down.
Lipophilia: no, that’s not a disease (or a fetish), rather it means that curcumin is soluble in fats, so we should take it near in time to a meal that contains at least a tablespoon of oil in total (so if you’re cooking a curry with your turmeric, this need is covered already, for example).
Supplement provenance: he recommends picking a supplement that’s been tested by a reputable 3rd party, as otherwise turmeric can be quite prone to impurities (which can include lead and arsenic, so, not great).
Contraindications: for some people, curcumin can cause gastrointestinal issues (less likely if taking with meals), and also, it can interact with blood-thinners. While taking aspirin or curcumin alone might help avoid circulatory problems, taking both could increase the bleeding risk for some people, for example. Similarly, if taking curcumin and metformin while diabetic, one must watch out for the combination being too effective at lowering blood sugar levels, and thus causing hypoglycemia instead. Similar deal with blood pressure medications.
There’s more in the video though (yes really; we know we wrote a lot but it’s information-dense), so do check it out:
Click Here If The Embedded Video Doesn’t Load Automatically
Want to know more?
You can also check out our related articles:
Why Curcumin (Turmeric) Is Worth Its Weight In Gold
Black Pepper’s Impressive Anti-Cancer Arsenal (And More)Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is Ant Oil Just “Snake Oil”?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We Tested Out “Ant Egg Oil”
Did you know?! There’s a special protein found only in the eggs of a particular species of ant found in Turkey, that can painlessly and permanently stop (not just slow!) hair regrowth in places you’d rather not have hair.
Neither did we, and when we heard about it, we did our usual research, and discovered a startling secret.
…there probably isn’t.
We decided to dig deeper, and the plot (unlike the hair in question) thickens:
We could not find any science for or against (or even generally about) the use of ant egg oil to prevent hair regrowth. Not a peep. What we did find though was a cosmetic chemist who did an analysis of the oil as sold, and found its main ingredient appears to be furan-2-carbaldehyde, or Furfural, to its friends.
Surprise! There’s also no science that we could find about the effect of Furfural (we love the name, though! Fur for all!) on hair, except that it’s bad for rodents (and their hair) if they eat a lot of it. So please don’t eat it. Especially if you’re a mouse.
And yet, many ostensibly real reviews out in the wild claim it works wonders. So, we took the investigative reporting approach and tried it ourselves.
That’s right, a plucky member of our team tried it, and she reports:
❝ At first glance, it seems like olive oil. There’s something else though, adding a darker colour and a slight bitterness to the smell.
After waxing, I applied a little every few days. When the hair eventually regrew (and it did), it grew back thinner, and removing the new hairs was a strangely easy experience, like pulling hairs out of soft soap instead of out of skin. It didn’t hurt at all, either.
I had more of the oil, so I kept going with the treatment, and twelve weeks later there are very few hairs regrowing at all; probably there will be none left soon. Whatever’s in this, be it from ant eggs or wheat bran or something else entirely, it worked for me!❞
So in short: it remains a mystery for now! If you try it, let us know how it went for you.
Here’s the “interesting” website that sells it, though you may find it for less on eBay or similar. (Note, we aren’t earning any commissions from these links. We just wanted to make it easier for you to dive deeper).
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Who Screens The Sunscreens?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We Screen The Sunscreens!

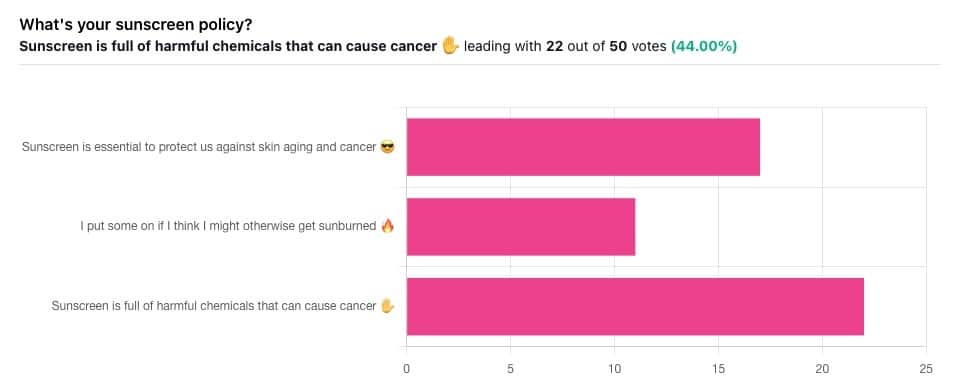
Yesterday, we asked you what your sunscreen policy was, and got a spread of answers. Apparently this one was quite polarizing!
One subscriber who voted for “Sunscreen is essential to protect us against skin aging and cancer” wrote:
❝My mom died of complications from melanoma, so we are vigilant about sun and sunscreen. We are a family of campers and hikers and gardeners—outdoors in all seasons—and we never burn❞
Our condolences with regard to your mom! Life is so precious, and when something like that happens, it tends to stick with us. We’re glad you and your family are taking care of yourselves.
Of the subscribers who voted for “I put some on if I think I might otherwise get sunburned”, about half wrote to express uncertainties:
- uncertainty about how safe it is, and
- uncertainty about how helpful it is
…so we’re going to tackle those questions in a moment. But what of those who voted for “Sunscreen is full of harmful chemicals that can cause cancer”?
Of those, only one wrote a message, which was to say one has to be very careful of what is in the formula.
Let’s take a look, then…
Sunscreen is full of harmful chemicals that can cause cancer: True or False?
False—according to current best science. Research is ongoing!
There are four main chemicals (found in most sunscreens) that people tend to worry about:
- Abobenzone
- Oxybenzone
- Octocrylene
- Ecamsule
Now, these two sound like four brands of rocket fuel, but then, dihydrogen monoxide (DHMO), which is also found in most sunscreens, sounds like a deadly toxin too. That’s water, by the way.
But what of these four chemicals? Well, as we say, research is ongoing, but we found a study that measured all four, to see how much got into the blood, and what adverse effects, if any, this caused.
We’ll skip to their conclusion:
❝In this preliminary study involving healthy volunteers, application of 4 commercially available sunscreens under maximal use conditions resulted in plasma concentrations that exceeded the threshold established by the FDA for potentially waiving some nonclinical toxicology studies for sunscreens. The systemic absorption of sunscreen ingredients supports the need for further studies to determine the clinical significance of these findings. These results do not indicate that individuals should refrain from the use of sunscreen.❞
Now, “exceeded the threshold established by the FDA for potentially waiving some nonclinical toxicology studies for sunscreens” sounds alarming, so why did they close with the words “These results do not indicate that individuals should refrain from the use of sunscreen”?
Let’s skip back up to a line from the results:
❝The most common adverse event was rash, which developed in 1 participant with each sunscreen.❞
This was most probably due to the oxybenzone, which can cause allergic skin reactions in some people.
Let us take a moment to remember the most common adverse event that occurs from not wearing sunscreen: sunburn!
You can read the full study here:
None of those ingredients have been found to be carcinogenic, even at the maximal blood plasma concentrations studied, from applications 4x/day to 75% of the body.
UVA rays, on the other hand, are absolutely very much known to cause cancer, and the effect is cumulative.
Sunscreen is essential to protect us against skin aging and cancer: True or False?
True, unequivocally, unless we live indoors and/or otherwise never go about under sunlight.
“But our ancestors—” lived under the same sun we do, and either used sunscreen or got advanced skin aging and cancer.
Sunscreen of times past ranged from mud to mineral lotions, but it’s pretty much always existed. Even non-human animals that have skin and don’t have fur or feathers, tend to take mud-baths in sunny parts of the world.
If you’d like to avoid oxybenzone and other chemicals, though, you might have your reasons. Maybe you’re allergic, or maybe you read that it’s a potential endocrine disruptor with estrogen-like and anti-androgenic properties that you don’t want.
There are other options, to include physical blockers containing zinc and titanium dioxide, which are generally recognized as safe and effective ingredients.
If you’re interested, you can even make your own sunscreen that blocks both UVA and UVB rays (UVA is what causes skin cancer; UVB is “milder” and is what causes sunburn):
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: