Saturated Fats & Lymphedema
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to lymphedema, what’s better than compression than compression garments and lymphatic drainage?
If you guessed “saturated fats”, then here is where we must disappoint you, because no, it’s rather the opposite—a diet low in saturated fats will ease lymphedema symptoms, while a diet high in saturated fats can bring on or worsen lymphedema.
But first, what is lymphedema?
More than one way to lymphedema
Lymphedema’s name literally means “lymphatic swelling”, and that’s exactly what it is.
First, know that lymphedema can be divided into primary and secondary lymphedema:
- Primary lymphedema = if you have a congenital genetic mutation that results in a malformed, and thus dysfunctional, lymphatic system
- Secondary lymphedema = you originally had a nicely working lymphatic system, which was then damaged by something else
The former is definitionally congenital.
Note: it’s not beyond the realm of possibility that such a genetic mutation could be acquired later by something that affects the genes (retrovirus, genotoxic substances, radiation, cancer, etc), but if this occurs, it would still be definitionally secondary lymphedema, because it occurred as a result of something damaging an initially normal, functional lymphatic system.
Secondary lymphedema usually comes about as a result of such things as cancer treatment, infection, or injury, including the typical progress of untreated lipedema.
Lipedema occurs mostly in women, mostly in times of hormonal change, with increasing risk as time goes by (so for example, puberty yields a lower risk than pregnancy, which yields a lower risk than menopause).
Lipedema’s name literally means “fat swelling”, and can easily be mistaken for obesity or, in its earlier stages, just pain old cellulite.
Rather than derail this article by going more deeply into lipedema, we’ll drop a link to our previous article on such: Watch Out For Lipedema
FABP4: a protein that’s sometimes not so fab after all
FABP4 is short for “fatty-acid-binding protein 4”.
You can probably guess what its job is.
Now, while this is a job that does need to be done, people with lymphedema (either kind) have nearly 3x as much of this protein, and inhibiting it (with a chemical inhibitor) results in a 50% reduction in lymphedema.
If you don’t have such chemical inhibitors in your kitchen, don’t worry, because a dietary intervention achieves very similar results—at least, in animal experiments so far, but in this case it’s highly unlikely that the results won’t translate to human patients, it’s just that that science has yet to be done, to be sure.
Specifically, per the most recent research by Dr. Karina Gomes et al., switching to a diet high in saturated fats brought on or worsened lymphedema (as mentioned up top), and/but importantly, switching to a diet low in saturated fats reversed these effects.
You can read this study in full, here: Saturated fatty acids induce lipotoxicity in lymphatic endothelial cells contributing to secondary lymphedema development
Want to learn more?
Check out:
- Nutrition To Combat Lymphedema & Lipedema ← this is a bit older, so it doesn’t mention the saturated fat connection, but has some other good pointers
- Can Saturated Fats Be Healthy? ← yes, albeit in very small portions, and only certain kinds, and certainly not butter, cream, or fatty meat (fish have their place, though!)
- Butter vs Plant Oils: What The Latest Evidence Shows ← this was a topic of some debate in the US earlier this year (2025, at time of writing), but the science quite clear
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Tretinoin: Because Prevention Is Better Than Cure

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The skin is an important organ to keep young and healthy, because a lot follows from it:
Protect, preserve, prevent
Jennifer Myers (now 43) began prescription retinoids not for beautifying but to treat a terrible case of cystic acne, starting with Duac and Benzaclin, then Tazorac, then Renova, then Retin-A Micro, then Retin-A cream and gel, eventually landing on Atralin, which transformed her skin. Quite a journey!
As you might imagine, the acne was physically painful and emotionally damaging during her late teens and early 20s, and the long search for something that worked required patience, distress tolerance, and persistence.
She wants to make clear that while she inherited her facial features, she did not inherit clear skin; quite to the contrary, she inherited severe acne from her mother—and her clear, smooth complexion today is earned through decades of consistency.
Consequently, she finds it frustrating that the skincare market overwhelms people into buying “shiny” new products; she encourages ignoring trends and sticking to what already works for at least 12 weeks, ideally one to two years, before judging results, because meaningful changes from tretinoin take months; in her case, it took a full year before she had the “new face” she maintains today, and many people quit too early because they expect overnight transformation.
In terms of what it will and won’t do: it improves skin turnover (which is its main mechanism of action), boosts collagen, smooths texture, brightens skin, and delays premature visible signs of aging, but it does not erase wrinkles, eliminate pores, or reverse established structural changes.
Aside from that, she attributes part of her result to diet, avoiding sugar, not smoking, and of course protecting against UV exposure.
Why is she telling us this? She wants to model what healthy, non-modified, naturally aging skin in one’s 40s can look like—she does not aim to look younger than she is, only to look like a well-cared-for 43-year-old woman.
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Undo The Sun’s Damage To Your Skin ← because while prevention is much better than cure, tretinoin can help with this, too
Take care!
Share This Post
-

How We Age: The Science of Longevity – by Dr. Coleen Murphy
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author is not a glossy “name brand” and has nothing to sell (besides her book). This shows, because it’s clearly not a book that was rushed out as a marketing ploy. Indeed, she begins with the words:
❝This book took me several years to write and is largely based on information I gathered while teaching my class, “Molecular Mechanisms of Longevity: The Genetics, Genomics, and Cell Biology of Aging,” at Princeton University.❞
~ Dr. Coleen Murphy
Thus, as you may imagine, it’s a thorough book, thoughtful, with conscientious attention to detail. As a reader, you are essentially getting the knowledge of a Princeton genomics class.
She covers what’s going on in our genes, in our cells, and in our bodies, when we age; why some animals don’t, and what things affect that. She talks biomarkers of aging and the industry gold standard “Health-Related Quality of Life” metrics. We learn about insulin signalling and FOXO targets; the role of caloric restriction or intermittent fasting, topics such as molecular homeostasis in the regulation of longevity (hello senolytics and chaperone-mediated autophagy), the microbiome and epigenetics, as well as mitochondrial management, cell replacement (including induced pluripotent stem cells), and even DNA repair. And yes, a lot about cognitive aging and how to slow it too.
The style is academic and/but perfectly readable; she explains everything as we go. We’ll note, though, that it’s not dry academic—her personality comes through throughout, in a good way that makes it a pleasant read as well as an informative one.
Bottom line: if you’d like a much deeper understanding of the mechanics of aging than we have room to get into in our articles at 10almonds, this book is a highly recommendable perfect opportunity.
Click here to check out How We Age, and learn about the science of longevity!
PS: we’ve reviewed a few books about the science of aging/longevity recently, and they’ve each been good, but if you’re going to get only one, we recommend this one, as in this reviewer’s opinion, it’s the best 😎
Share This Post
-
Melatonin Supplementation & Your Heart
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We previously wrote about about melatonin:
❝Melatonin is a hormone normally made in our pineal gland. It helps regulate our circadian rhythm, by making us sleepy.
It has other roles too—it has a part to play in regulating immune function, something that also waxes and wanes as a typical day goes by.
Additionally, since melatonin and cortisol are antagonistic to each other, a sudden increase in either will decrease the other. Our brain takes advantage of this, by giving us a cortisol spike in the morning to help us wake up.
As a supplement, it’s generally enjoyed with the intention of inducing healthy, natural, restorative sleep.❞
Read in full: Melatonin: A Safe, Natural Sleep Aid? ← our research review article that does cover the pros and cons, and yes, there are indeed downsides too, including some contraindications e.g. melatonin helps regulate immune function, so that’s something to bear in mind if you’re on immunosuppressants or otherwise have an autoimmune disorder. It can also interfere with blood pressure medications and blood thinners, and may make epilepsy meds less effective.
The new news
Researchers (Dr. Ekenedilichukwu Nnadi et al.) looked at 130,828 adults (of whom, mostly women, average age 56) with insomnia, and found an important association with regard to long-term melatonin use.
Specifically: in adults with chronic insomnia, documented melatonin use for ≥12 months was linked with 90% higher 5-year risk of incident heart failure versus matched non-users (4.6% vs 2.7%), plus 3.5x higher risk of heart-failure hospitalization and 81% higher all-cause mortality.
There are some limitations: this was an observational study, based on electronic health records (TriNetX), and doesn’t outright prove causation.
For example, OTC users might have been misclassified as non-users, dosing and adherence weren’t known, and further data-confounding from variations in insomnia severity, mental health, or other meds is plausible too.
Still, the association is strong, so that seems like cause for concern, when likely nobody will die from not supplementing with melatonin.
The principle here is, like in the Hippocratic oath, “first, do no harm”.
In other words: if not taking the meds is definitely safe, and taking the meds may be unsafe, then erring on the side of not taking them is likely the best option.
See also: Are You Taking PIMs? Getting Off The Overmedication Train ← “PIMs” is the medical shorthand for “potentially inappropriate medications”
And, for that matter, The Common Meds That Make You More Likely To Die From A Fall ← when, statistically speaking, after a certain age, a fall is much more likely to kill you than taking longer to get to sleep
If you have been using melatonin most nights for months, consider tapering your dose downwards and switching to things like CBT-I and more focused sleep-hygiene strategies, for example:
- How to Fall Asleep Faster: CBT-Insomnia Treatment
- Don’t Do These Things If You’re Over 50 (And Want Better Sleep) ← this about common mistakes, including one involving melatonin supplementation
Of course, do discuss any long-term use with your doctor/pharmacist—especially if you have cardiovascular risk or symptoms (e.g. breathlessness, ankle swelling, unusual fatigue).
If you’d like to read the AHA’s press release for the study we talked about (it has a lot more details than we have room for here), then here you go:
Want to try some?
Since the above is only about chronic long-term use, perhaps you’d still like some for short term use, ideally after consulting with your doctor and/or pharmacist.
If that’s the case, then as ever, we don’t sell it (or anything else), but for your convenience, here is an example product on Amazon.
Enjoy!
Share This Post


Related Posts
-
Is owning a dog good for your health?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australia loves dogs. We have one of the highest rates of pet ownership in the world, and one in two households has at least one dog.
But are they good for our health?
Mental health is the second-most common reason cited for getting a dog, after companionship. And many of us say we “feel healthier” for having a dog – and let them sleep in our bedroom.
Here’s what it means for our physical and mental health to share our homes (and doonas) with our canine companions.

Pogodina Natalia/Shutterstock Are there physical health benefits to having a dog?
Having a dog is linked to lower risk of death over the long term. In 2019, a systematic review gathered evidence published over 70 years, involving nearly four million individual medical cases. It found people who owned a dog had a 24% lower risk of dying from any cause compared to those who did not own a dog.
Having a dog may help lower your blood pressure through more physical activity. Barnabas Davoti/Pexels Dog ownership was linked to increased physical activity. This lowered blood pressure and helped reduce the risk of stroke and heart disease.
The review found for those with previous heart-related medical issues (such as heart attack), living with a dog reduced their subsequent risk of dying by 35%, compared to people with the same history but no dog.
Another recent UK study found adult dog owners were almost four times as likely to meet daily physical activity targets as non-owners. Children in households with a dog were also more active and engaged in more unstructured play, compared to children whose family didn’t have a dog.
Exposure to dirt and microbes carried in from outdoors may also strengthen immune systems and lead to less use of antibiotics in young children who grow up with dogs.
Children in households with a dog were often more active. Maryshot/Shutterstock Health risks
However, dogs can also pose risks to our physical health. One of the most common health issues for pet owners is allergies.
Dogs’ saliva, urine and dander (the skin cells they shed) can trigger allergic reactions resulting in a range of symptoms, from itchy eyes and runny nose to breathing difficulties.
A recent meta-analysis pooled data from nearly two million children. Findings suggested early exposure to dogs may increase the risk of developing asthma (although not quite as much as having a cat does). The child’s age, how much contact they have with the dog and their individual risk all play a part.
Slips, trips and falls are another risk – more people fall over due to dogs than cats.
Having a dog can also expose you to bites and scratches which may become infected and pose a risk for those with compromised immune systems. And they can introduce zoonotic diseases into your home, including ring worm and Campylobacter, a disease that causes diarrhoea.
For those sharing the bed there is an elevated the risk of allergies and picking up ringworm. It may result in lost sleep, as dogs move around at night.
On the other hand some owners report feeling more secure while co-sleeping with their dogs, with the emotional benefit outweighing the possibility of sleep disturbance or waking up with flea bites.
Proper veterinary care and hygiene practices are essential to minimise these risks.
Many of us don’t just share a home with a dog – we let them sleep in our beds. Claudia Mañas/Unsplash What about mental health?
Many people know the benefits of having a dog are not only physical.
As companions, dogs can provide significant emotional support helping to alleviate symptoms of anxiety, depression and post-traumatic stress. Their presence may offer comfort and a sense of purpose to individuals facing mental health challenges.
Loneliness is a significant and growing public health issue in Australia.
In the dog park and your neighbourhood, dogs can make it easier to strike up conversations with strangers and make new friends. These social interactions can help build a sense of community belonging and reduce feelings of social isolation.
For older adults, dog walking can be a valuable loneliness intervention that encourages social interaction with neighbours, while also combating declining physical activity.
However, if you’re experiencing chronic loneliness, it may be hard to engage with other people during walks. An Australian study found simply getting a dog was linked to decreased loneliness. People reported an improved mood – possibly due to the benefits of strengthening bonds with their dog.
Walking a dog can make it easier to talk to people in your neighbourhood. KPegg/Shutterstock What are the drawbacks?
While dogs can bring immense joy and numerous health benefits, there are also downsides and challenges. The responsibility of caring for a dog, especially one with behavioural issues or health problems, can be overwhelming and create financial stress.
Dogs have shorter lifespans than humans, and the loss of a beloved companion can lead to depression or exacerbate existing mental health conditions.
Lifestyle compatibility and housing conditions also play a significant role in whether having a dog is a good fit.
The so-called pet effect suggests that pets, often dogs, improve human physical and mental health in all situations and for all people. The reality is more nuanced. For some, having a pet may be more stressful than beneficial.
Importantly, the animals that share our homes are not just “tools” for human health. Owners and dogs can mutually benefit when the welfare and wellbeing of both are maintained.
Tania Signal, Professor of Psychology, School of Health, Medical and Applied Sciences, CQUniversity Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Apricot vs Avocado – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apricot to avocado, we picked the avocado.
Why?
Both are great, but…
In terms of macros,apricot has slightly more carbs, while avocado has more than 30x the fat (famously healthy fats, including a good ratio of omega-3 and omega-6), and more than 3x the fiber. So, an easy win for avocado here.
In the category of vitamins, apricot has 13x the vitamin A, while avocado has several times more of vitamins B1, B2, B3, B5, B6, B7, B9, E, K, and choline, winning.
Looking at minerals, apricot is not higher in any minerals, while avocado has more copper, iron, magnesium, manganese, phosphorus, selenium, and zinc; another clear win for avocado.
In other matters, apricot has some specific anticancer properties that avocado can’t boast, so apricot does win one point here.
Adding up the sections makes for an overwhelming overall win for avocado, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Top 8 Fruits That Prevent & Kill Cancer
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Brain As A Work-In-Progress
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
And The Brain Goes Marching On!

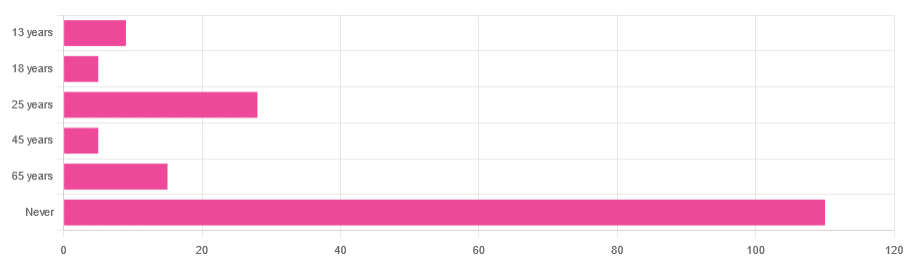
In Tuesday’s newsletter, we asked you “when does the human brain stop developing?” and got the above-depicted, below-described, set of responses:
- About 64% of people said “Never”
- About 16% of people said “25 years”
- About 9% of people said “65 years”
- About 5% of people said “13 years”
- About 3% of people said “18 years”
- About 3% of people said “45 years”
Some thoughts, before we get into the science:
An alternative wording for the original question was “when does the human brain finish developing”; the meaning is the same but the feeling is slightly different:
- “When does the human brain stop developing?” focuses attention on the idea of cessation, and will skew responses to later ages
- When does the human brain finish developing?” focuses on attention on a kind of “is it done yet?” and will skew responses to earlier ages
Ultimately, since we had to chose one word or another, we picked the shortest one, but it would have been interesting if we could have done an A/B test, and asked half one way, and half the other way!
Why we picked those ages
We picked those ages as poll options for reasons people might be drawn to them:
- 13 years: in English-speaking cultures, an important milestone of entering adolescence (note that the concept of a “teenager” is not precisely universal as most languages do not have “-teen” numbers in the same way; the concept of “adolescent” may thus be tied to other milestones)
- 18 years: age of legal majority in N. America and many other places
- 25 years: age popularly believed to be when the brain is finished developing, due to a study that we’ll talk about shortly (we guess that’s why there’s a spike in our results for this, too!)
- 45 years: age where many midlife hormonal changes occur, and many professionals are considered to have peaked in competence and start looking towards retirement
- 65 years: age considered “senior” in much of N. America and many other places, as well as the cut-off and/or starting point for a lot of medical research
Notice, therefore, how a lot of things are coming from places they really shouldn’t. For example, because there are many studies saying “n% of people over 65 get Alzheimer’s” or “n% of people over 65 get age-related cognitive decline”, etc, 65 becomes the age where we start expecting this—because of an arbitrary human choice of where to draw the cut-off for the study enrollment!
Similarly, we may look at common ages of legal majority, or retirement pensions, and assume “well it must be for a good reason”, and dear reader, those reasons are more often economically motivated than they are biologically reasoned.
So, what does the science say?
Our brains are never finished developing: True or False?
True! If we define “finished developing” as “we cease doing neurogenesis and neuroplasticity is no longer in effect”.
Glossary:
- Neurogenesis: the process of creating new brain cells
- Neuroplasticity: the process of the brain adapting to changes by essentially rebuilding itself to suit our perceived current needs
We say “perceived” because sometimes neuroplasticity can do very unhelpful things to us (e.g: psychological trauma, or even just bad habits), but on a biological level, it is always doing its best to serve our overall success as an organism.
For a long time it was thought that we don’t do neurogenesis at all as adults, but this was found to be untrue:
How To Grow New Brain Cells (At Any Age)
Summary of conclusions of the above: we’re all growing new brain cells at every age, even if we be in our 80s and with Alzheimer’s disease, but there are things we can do to enhance our neurogenic potential along the way.
Neuroplasticity will always be somewhat enhanced by neurogenesis (after all, new neurons get given jobs to do), and we reviewed a great book about the marvels of neuroplasticity including in older age:
Our brains are still developing up to the age of 25: True or False?
True! And then it keeps on developing after that, too. Now this is abundantly obvious considering what we just talked about, but see what a difference the phrasing makes? Now it makes it sound like it stops at 25, which this statement doesn’t claim at all—it only speaks for the time up to that age.
A lot of the popular press about “the brain isn’t fully mature until the age of 25” stems from a 2006 study that found:
❝For instance, frontal gray matter volume peaks at about age 11.0 years in girls and 12.1 years in boys, whereas temporal gray matter volume peaks at about age at 16.7 years in girls and 16.2 years in boys. The dorsal lateral prefrontal cortex, important for controlling impulses, is among the latest brain regions to mature without reaching adult dimensions until the early 20s.❞
Source: Structural Magnetic Resonance Imaging of the Adolescent Brain
There are several things to note here:
- The above statement is talking about the physical size of the brain growing
- Nowhere does he say “and stops developing at 25”
However… The study only looked at brains up to the age of 25. After that, they stopped looking, because the study was about “the adolescent brain” so there has to be a cut-off somewhere, and that was the cut-off they chose.
This is the equivalent of saying “it didn’t stop raining until four o’clock” when the reality is that four o’clock is simply when you gave up on checking.
The study didn’t misrepresent this, by the way, but the popular press did!
Another 2012 study looked at various metrics of brain development, and found:
- Synapse overproduction into the teens
- Cortex pruning into the late 20s
- Prefrontal pruning into middle age at least (they stopped looking)
- Myelination beyond middle age (they stopped looking)
Source: Experience and the developing prefrontal cortex ← check out figure 1, and make sure you’re looking at the human data not the rat data
So how’s the most recent research looking?
Here’s a 2022 study that looked at 123,984 brain scans spanning the age range from mid-gestation to 100 postnatal years, and as you can see from its own figure 1… Most (if not all) brain-things keep growing for life, even though most slow down at some point, they don’t stop:
Brain charts for the human lifespan ← check out figure 1; don’t get too excited about the ventricular volume column as that is basically “brain that isn’t being a brain”. Do get excited about the rest, though!
Want to know how not to get caught out by science being misrepresented by the popular press? Check out:
How Science News Outlets Can Lie To You (Yes, Even If They Cite Studies!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: