Reflexology: What The Science Says
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How Does Reflexology Work, Really?
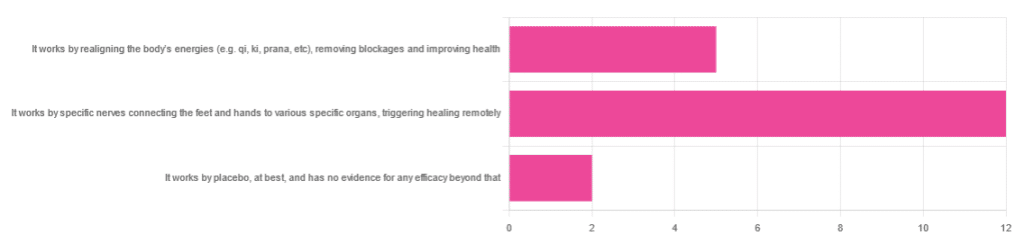
In Wednesday’s newsletter, we asked you for your opinion of reflexology, and got the above-depicted, below-described set of responses:
- About 63% said “It works by specific nerves connecting the feet and hands to various specific organs, triggering healing remotely”
- About 26% said “It works by realigning the body’s energies (e.g. qi, ki, prana, etc), removing blockages and improving health“
- About 11% said “It works by placebo, at best, and has no evidence for any efficacy beyond that”
So, what does the science say?
It works by realigning the body’s energies (e.g. qi, ki, prana, etc), removing blockages and improving health: True or False?
False, or since we can’t prove a negative: there is no reliable scientific evidence for this.
Further, there is no reliable scientific evidence for the existence of qi, ki, prana, soma, mana, or whatever we want to call it.
To save doubling up, we did discuss this in some more detail, exploring the notion of qi as bioelectrical energy, including a look at some unreliable clinical evidence for it (a study that used shoddy methodology, but it’s important to understand what they did wrong, to watch out for such), when we looked at [the legitimately very healthful practice of] qigong, a couple of weeks ago:
Qigong: A Breath Of Fresh Air?
As for reflexology specifically: in terms of blockages of qi causing disease (and thus being a putative therapeutic mechanism of action for attenuating disease), it’s an interesting hypothesis but in terms of scientific merit, it was pre-emptively supplanted by germ theory and other similarly observable-and-measurable phenomena.
We say “pre-emptively”, because despite orientalist marketing, unless we want to count some ancient pictures of people getting a foot massage and say it is reflexology, there is no record of reflexology being a thing before 1913 (and that was in the US, by a laryngologist working with a spiritualist to produce a book that they published in 1917).
It works by specific nerves connecting the feet and hands to various specific organs, triggering healing remotely: True or False?
False, or since we can’t prove a negative: there is no reliable scientific evidence for this.
A very large independent review of available scientific literature found the current medical consensus on reflexology is that:
- Reflexology is effective for: anxiety (but short lasting), edema, mild insomnia, quality of sleep, and relieving pain (short term: 2–3 hours)
- Reflexology is not effective for: inflammatory bowel disease, fertility treatment, neuropathy and polyneuropathy, acute low back pain, sub acute low back pain, chronic low back pain, radicular pain syndromes (including sciatica), post-operative low back pain, spinal stenosis, spinal fractures, sacroiliitis, spondylolisthesis, complex regional pain syndrome, trigger points / myofascial pain, chronic persistent pain, chronic low back pain, depression, work related injuries of the hip and pelvis
Source: Reflexology – a scientific literary review compilation
(the above is a fascinating read, by the way, and its 50 pages go into a lot more detail than we have room to here)
Now, those items that they found it effective for, looks suspiciously like a short list of things that placebo is often good for, and/or any relaxing activity.
Another review was not so generous:
❝The best evidence available to date does not demonstrate convincingly that reflexology is an effective treatment for any medical condition❞
~ Dr. Edzard Ernst (MD, PhD, FMedSci)
Source: Is reflexology an effective intervention? A systematic review of randomised controlled trials
In short, from the available scientific literature, we can surmise:
- Some researchers have found it to have some usefulness against chiefly psychosomatic conditions
- Other researchers have found the evidence for even that much to be uncompelling
It works by placebo, at best, and has no evidence for any efficacy beyond that: True or False?
Mostly True; of course reflexology runs into similar problems as acupuncture when it comes to testing against placebo:
How Does One Test Acupuncture Against Placebo Anyway?
…but not quite as bad, since it is easier to give a random foot massage while pretending it is a clinical treatment, than to fake putting needles into key locations.
However, as the paper we cited just above (in answer to the previous True/False question) shows, reflexology does not appear to meaningfully outperform placebo—which points to the possibility that it does work by placebo, and is just a placebo treatment on the high end of placebo (because the placebo effect is real, does work, isn’t “nothing”, and some placebos work better than others).
For more on the fascinating science and useful (applicable in daily life!) practicalities of how placebo does work, check out:
How To Leverage Placebo Effect For Yourself
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Unprocess Your Life – by Rob Hobson

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Rob Hobson is not a doctor, but he is a nutritionist with half the alphabet after his name (BSc, PGDip, MSc, AFN, SENR) and decades of experience in the field.
The book covers, in jargon-free fashion, the science of ultra-processed foods, and why for example that pack of frozen chicken nuggets are bad but a pack of tofu (which obviously also took some processing, because it didn’t grow on the plant like that) isn’t.
This kind of explanation puts to rest a lot of the “does this count?” queries that a reader might have when giving the shopping list a once-over.
He also covers practical considerations such as kitchen equipment that’s worth investing in if you don’t already have it, and an “unprocessed pantry” shopping list.
The recipes (yes, there are recipes, nearly a hundred of them) are not plant-based by default, but there is a section of vegan and vegetarian recipes. Given that the theme of the book is replacing ultra-processed foods, it doesn’t mean a life of abstemiousness—there are recipes for all manner of things from hot sauce to cakes. Just, healthier unprocessed ones! There are classically healthy recipes too, of course.
Bottom line: if you’ve been wishing for a while that you could get rid of those processed products that are just so convenient that you haven’t got around to replacing them with healthier options, this book can indeed help you do just that.
Click here to check out Unprocess Your Life, and unprocess your life!
Share This Post
-

8 Signs Of Hypothyroidism Beyond Tiredness & Weight Gain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to hypothyroidism, most people know to look out for tiredness and weight gain, and possibly menstrual disturbances in those who menstruate. But those symptoms could be caused by very many things, so what more specific signs and symptoms of hypothyroidism should we look out for?
Dr. James O’Donovan shows us in this short video:
The lesser-known signs
Dr. O’Donovan discusses:
- Asteatotic eczema (also called: eczema craquelé): dry, cracked skin with a “crazy paving” appearance, leading to fissures. It’s common on the lower legs, back, torso, and arms, especially in older patients and especially in winter.
- Cold peripheries with pale, dry, coarse skin: cold hands and feet, along with dryness due to decreased sweating; these invariably come together, though the exact link is unclear.
- Yellowish hue to the skin (carotenoderma): yellow-orange discoloration from elevated beta-carotene levels. This can easily be mistaken for jaundice and also occurs in diabetes, liver, and kidney diseases.
- Thin, brittle hair: the hair on one’s head may become dry, coarse, and fall out in handfuls.
- Loss of hair on the outer third of eyebrows: thinning or disappearance of hair in this very specific area.
- Slow-growing, rigid, brittle nails: slowed nail growth due to decreased cell turnover rate. Ridges may form as keratin cells accumulate.
- Myxedema: puffy face, eyelids, legs, and feet caused by tissue swelling from cutaneous deposition.
- Delayed wound healing: is what it sounds like; a slower healing process.
10almonds note: this video, like much of medical literature as well, does focus on what things are like for white people. Black people with hypothyroidism are more likely to see a lightening of hair pigmentation, and, in contrast, hyperpigmentation of the skin, usually in patches. We couldn’t find data for other ethnicities or skintones, but it does seem that most of the signs and symptoms (unrelated to pigmentation) should be the same for most people.
Meanwhile, for more on the above 8 signs, with visuals, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The Three Rs To Boost Thyroid-Related Energy Levels
Take care!
Share This Post
-
Apples vs Dates – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apples to dates, we picked the dates.
Why?
Both have their strengths, but ultimatley, it wasn’t close:
In terms of macros, dates have more fiber and carbs, for an approximately equal glycemic index. Thus, we say dates win this category as the more nutritionally dense option.
In the category of vitamins, apples have more of vitamins A, C, and E, while dates have more of vitamins B1, B2, B3, B5, B6, B7, B9, K, and choline. A clear win for dates.
When it comes to minerals, it’s even more one-sided: apples are not richer in any minerals, while dates have a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. An overwhelming win for dates.
Of course, enjoy either or both (diversity is good), but if you want the most nutrients per bite, it’s dates.
Want to learn more?
You might like to read:
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
Enjoy!
Share This Post
Related Posts
-
Neurologists Debunk 11 Brain Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Neuroscientists Dr. Santoshi Billakota and Dr. Brad Kamitaki debunk 11 myths about the brain. How many did you know?
From the top
Without further ado, the myths are…
- “We only use 10% of our brains”: False! We use most parts of our brain at different times, depending on the activity. PET/MRI scans show widespread usage.
- “The bigger the brain, the smarter the creature”: False! While there’s often a correlation, intelligence depends on brain complexity and development of specific regions, not overall size. For this reason get, for example, some corvids that are more intelligent than some dogs.
- “IQ tests are an accurate measure of intelligence”: False! IQ tests measure limited aspects of intelligence and are influenced by external factors like test conditions and education.
- “Video games rot your brain”: False! Video games can improve problem-solving, strategy, and team-building skills when played in moderation.
- “Memory gets worse as you age”: Partly false. While episodic memory may decline, semantic and procedural memory often improve with age.
- “Left-brained people are logical, and right-brained people are creative”: False! Both hemispheres work together, and personality or skills are influenced by environment and experiences, not brain hemispheres.
- “You can’t prevent a stroke”: False! Strokes can often be prevented by managing risk factors like blood pressure, cholesterol, and lifestyle choices.
- “Eating fish makes you smarter”: False! Eating fish, especially those rich in omega-3s, can support brain health but won’t increase intelligence.
- “You can always trust your senses”: False! Senses can be deceptive and influenced by emotions, memories, or neurological conditions.
- “Different sexes have different brains”: False! Structurally, brains are the same regardless of chromosomal sex; differences arise from environmental (including hormonal) and experiential factors—and even there, there’s more than enough overlap that we are far from categorizable as sexually dimorphic.
- “If you have a seizure, you have epilepsy”: False! A seizure can occur from various causes, but epilepsy is defined by recurrent unprovoked seizures and requires specific diagnosis and treatment.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The Dopamine Myth ← a bonus 12th myth!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Why You Don’t Need 8 Glasses Of Water Per Day
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The idea that you need to drink eight glasses of water daily is a myth. For most people most of the time, this practice will not make your skin brighter, improve mental clarity, or boost energy levels. All that will happen as a result of drinking beyond your thirst, is that you’ll pee more.
A self-regulating system
Our kidneys regulate hydration by monitoring blood volume and salt levels. When blood becomes slightly saltier or its volume drops, such as through sweating, the kidneys absorb more water into the bloodstream. If needed, the body triggers thirst signals to encourage fluid intake.
In most cases, you can rely on your body’s natural thirst cues to manage hydration. Thirst is a reliable indicator of when you need to drink water, making constant monitoring of water intake unnecessary for most people.
There are some exceptions, though! Some people, such as those with kidney stones, especially older adults, or those with specific medical considerations and resultant advice from your doctor, may need to pay closer attention to their water intake.
Nor does hydration have to be a matter of “drinking water”: many foods and drinks, such as fruit, coffee, soups, etc, contribute to your daily water intake and (because the body processes it more slowly) are often more hydrating than plain water (which can just pass straight through if you take more than a certain amount at once). If you listen to your body’s thirst signals, there’s no need to rigidly count eight glasses of water each day.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Hydration Mythbusting ← this also covers why urine color is not as good a guide as your thirst
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Origin of Everyday Moods – by Dr. Robert Thayer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First of all, what does this title mean by “everyday moods”? By this the author is referring to the kinds of moods we have just as a matter of the general wear-and-tear of everyday life—not the kind that come from major mood disorders and/or serious trauma.
The latter kinds of mood take less explaining, in any case. Dr. Thayer, therefore, spends his time on the less obvious ones—which in turn are the ones that affect most of the most, every day.
Critical to Dr. Thayer’s approach is the mapping of moods by four main quadrants:
- High energy, high tension
- High energy, low tension
- Low energy, high tension
- Low energy, low tension
…though this can be further divided into 25 sectors, if we rate each variable on a scale of 0–4. But for the first treatment, it suffices to look at whether energy and tension are high or low, respectively, and which we’d like to have more or less of.
Then (here be science) how to go about achieving that in the most efficient, evidence-based ways. So, it’s not just a theoretical book; it has great practical value too.
The style of the book is accessible, and walks a fine line between pop-science and hard science, which makes it a great book for laypersons and academics alike.
Bottom line: if you’d like the cheat codes to improve your moods and lessen the impact of bad ones, this is the book for you.
Click here to check out The Origin of Everyday Moods, and manage yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: