Midwives Blame California Rules for Hampering Birth Centers Amid Maternity Care Crisis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Jessie Mazar squeezed the grab handle in her husband’s pickup and groaned as contractions struck her during the 90-minute drive from her home in rural northeastern California to the closest hospital with a maternity unit.
She could have reached Plumas District Hospital, in Quincy, in just seven minutes. But it no longer delivers babies.
Local officials have a plan for a birth center in Quincy, where midwives could deliver babies with backup from on-call doctors and a standby perinatal unit at the hospital, but state health officials have yet to approve it.
That left Mazar to brave the long, winding road — one sometimes blocked by snow, floods, or forest fires — to have her baby. Women across California are facing similar ordeals as hospitals increasingly close money-losing maternity units, especially in rural areas.
Midwife-operated birth centers offer an alternative for women with low-risk pregnancies and can play a crucial role in filling the gap left by hospitals’ retreat from obstetrics, maternal health advocates say.
Declining birth rates, staffing shortages, and financial pressures have led 56 California hospitals — about 1 in 6 — to shutter maternity units over the past dozen years.
But midwives say California’s regulatory regime around birth centers is unnecessarily preventing new centers from opening and leading some existing facilities to close. Obtaining a license can take as long as four years.
“All they’ve essentially done is made it more dangerous to have a baby,” said Sacramento midwife Bethany Sasaki. “People have to drive two hours now because a birth center can’t open, so it’s more dangerous. People are going to be having babies in cars on the side of the road.”
Last month, state Assembly member Mia Bonta introduced legislation to streamline the regulatory process and fix what she calls “a broken system” for licensing birth centers.
“We know that alternative birth centers lead to often better outcomes, lower-risk births, more opportunity for children to be born healthy, and also to lower maternal mortality and morbidity,” she said.
The proposed bill would remove various bureaucratic requirements, though many details have yet to be finalized. Bonta introduced the bill in its current form as a jumping-off point for discussions about how to expedite licensing.
“It’s a starting place,” said Sandra Poole, health policy advocate for the Western Center on Law & Poverty, a co-sponsor of the legislation.
For now, birth centers struggle with a gantlet of rules, only some clearly connected to patient safety. Over the past decade, the number of licensed birth centers in California dropped from 12 to five, according to Bonta.
Plumas County officials are trying to address one key issue: how far a birth center can be from a hospital with a round-the-clock obstetrics unit. State regulations say it can be no more than a 30-minute drive, a distance set when many more hospitals had maternity units.
The first-of-its-kind “Plumas model” aims to take advantage of flexibility provisions in the law to address the obstacle in a way that could potentially be replicated elsewhere in the state.
But the hospital’s application for a birth center and a perinatal unit has been “languishing” with the California Department of Public Health, which is “looking for cover from the legislature,” said Robert Moore, chief medical officer of Partnership HealthPlan of California, a Medi-Cal managed-care plan serving most of Northern California. Asked about the application, a CDPH spokesperson said only that it was under review.
The goal should be for all women to be within an hour’s drive of a hospital with an obstetrics unit, Moore said. Data shows the complication rate goes up after an hour and even higher after two hours, he said, while the benefit is less compelling between 30 and 60 minutes.
Numerous other regulations have made it difficult for birth centers to keep their doors open.
Since August, birth centers in Sacramento and Monterey have had to stop operating because their heating ducts failed to meet licensing requirements. The facilities fall under the same state Department of Health Care Access and Information regulations as primary care clinics, though birth centers see healthy families, not sick ones, and don’t need hospital-grade ventilation, said midwife Caroline Cusenza.
She had spent $50,000 remodeling the Monterey Birth & Wellness Center to include state-required items, such as nursing and hand-washing stations and a housekeeping closet. In the end, a requirement for galvanized steel heating vents, which would have required opening the ceiling at an unaffordable cost, prompted her heart-wrenching decision to close.
“We’re turning women away in tears,” said Sasaki, who owned Midtown Birth Center in Sacramento. She bought the building for $760,000 and spent $250,000 remodeling it in a way she believed met all licensing requirements. But regulators would not license it unless the heating system was redone. Sasaki estimated it would have cost an additional $50,000 to bring it into compliance — too much to keep operating.
She blamed her closure on “regulatory dysfunction.”
Legislation signed by Gov. Gavin Newsom last year could ease onerous building codes such as those governing Sasaki’s and Cusenza’s heating systems, said Poole, the health policy advocate.
The state has taken two to four years to issue birth center licenses, according to a brief by the Osher Center for Integrative Health at the University of California-San Francisco. The state Department of Public Health “works tirelessly to ensure health facilities are able to be properly licensed and follow all applicable requirements within our authority before and during their operation,” spokesperson Mark Smith said.
Bonta, an Oakland Democrat who chairs the Assembly’s health committee, said she would consider increasing the allowable drive time between a birth center and a hospital maternity unit as part of her new legislation.
The state last updated birth center regulations more than a decade ago, before hospitals’ mass exodus from obstetrics. “The hurdle is the time and distance standards without compromising safety,” Poole said. “But where there’s nothing right now, we would say a birth center is certainly a better alternative to not having any maternal care.”
Moore noted that midwife-led births in homes and birth centers are the mainstay of obstetric care in Europe, where the infant mortality rate is considerably lower than in the U.S. More than 98% of American babies are born in hospitals.
Babies delivered by midwives are more likely to be born vaginally, less likely to require intensive care, and more likely to breastfeed, the California Maternal Quality Care Collaborative has found. Midwife-led births also lead to fewer infant emergency room visits, hospitalizations, and neonatal deaths. And they cost far less: Birth centers generally charge one-quarter or less of the average cost of about $36,000 for a vaginal birth in a California hospital.
If they catered only to private-pay clients, Cusenza and Sasaki could have continued operating without licenses. They must be licensed, however, to receive payments from Medi-Cal and some private insurance companies, which they needed to remain in business. Medi-Cal, the state’s Medicaid health insurance program, which covers low-income residents, paid for about 40% of the state’s births in 2022.
Bonta has heard reports from midwives that the key to getting licensed is hunting down the right state health department advocate. “I don’t believe that we should be building resources based on the model of ‘Where’s Waldo?’ in finding a champion inside CDPH,” she said.
Lori Link, director of midwifery at Plumas District Hospital, believes the Plumas model can turn what’s become a maternity desert into an oasis. Jessie Mazar, whose son was born in September without complications at a Truckee hospital, would welcome the opportunity to deliver her planned second child in Quincy.
“That would be convenient,” she said. “We’re not holding our breath.”
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Food for Life – by Dr. Tim Spector

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book is, as the author puts it, “an eater’s guide to food and nutrition”. Rather than telling us what to eat or not eat, he provides an overview of what the latest science has to say about various foods, and leaves us to make our own informed decisions.
He also stands firmly by the “personalized nutrition” idea that he introduced in his previous book which we reviewed the other day, and gives advice on what tests we might like to perform.
The writing style is accessible, without shying away from reference to hard science. Dr. Spector provides lots of information about key chemicals, genes, gut bacteria, and more—as well as simply providing a very enjoyable read along the way.
Bottom line: if you’d like a much better idea of what food is (and isn’t) doing what, this book is an invaluable resource.
Click here to check out Food for Life, and make the best decisions for you!
Share This Post
-

Carrot vs Kale – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing carrot to kale, we picked the kale.
Why?
These are both known as carotene-containing heavyweights, but kale emerges victorious:
In terms of macros, carrot has more carbs while kale has more protein and fiber. An easy win there for kale.
When it comes to vitamins, both are great! But, carrots contain more of vitamins A, B5, and choline, whereas kale contains more of vitamins B1, B2, B3, B6, B9, C, E, and K. And while carrot’s strongest point is vitamin A, a cup of carrots contains around 10x the recommended daily dose of vitamin A, whereas a cup of kale contains “only” 6x the recommended daily dose of vitamin A. So, did we really need the extra in carrots? Probably not. In any case, kale already won on overall vitamin coverage, by a long way.
In the category of minerals, kale again sweeps. On the one hand, carrots contain more sodium. On the other hand, kale contains a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Not a tricky choice!
But don’t be fooled: carrots really are a nutritional powerhouse and a great food. Kale is just better—nutritionally speaking, in any case. If you’re making a carrot cake, please don’t try substituting kale; it will not work 😉
Want to learn more?
You might like to read:
Take care!
Share This Post
-

Good Energy – by Dr. Casey Means
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For a book with a title like “Good Energy” and chapters such as “Bad Energy Is the Root of Disease”, this is actually a very science-based book (and there are a flock of well-known doctors saying so in the “praise for” section, too).
The premise is simple: most of our health is a matter of what our metabolism is (or isn’t) doing, and it’s not just a case of “doing more” or “doing less”. Indeed, a lot of “our” energy is expended doing bad things (such as chronic inflammation, to give an obvious example).
Dr. Means outlines about a dozen things many people do wrong, and about a dozen things we can do right, to get our body’s energy system working for us, rather than against us.
The style here is pop-science throughout, and in the category of criticism, the bibliography is offloaded to her website (we prefer to have things in our hands). However, the information here is good, clearly-presented, and usefully actionable.
Bottom line: if you ever find yourself feeling run-down and like your body is using your resources against you rather than for you, this is the book to get you out of that slump!
Click here to check out Good Energy, and get your metabolism working for you!
Share This Post
Related Posts
-
Breast Milk’s Benefits That Are (So Far) Not Replicable
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Simply The Breast 🎶

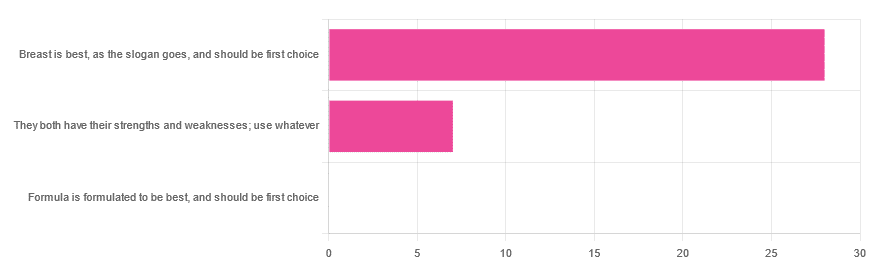
In Wednesday’s newsletter, we asked you for your opinion on breast vs formula milk (for babies!), and got the above-depicted, below-described, set of responses:
- 80% said “Breast is best, as the slogan goes, and should be first choice”
- 20% said “They both have their strengths and weaknesses; use whatever”
- 0% said “Formula is formulated to be best, and should be first choice”
That’s the first time we’ve ever had a possible poll option come back with zero votes whatsoever! It seems this topic is relatively uncontentious amongst our readership, so we’ll keep things brief today, but there is still a little mythbusting to be done.
So, what does the science say?
[Breast milk should be the first choice] at least for the few few weeks and months for the benefit of baby’s health as breast milk has protective factors formula does not: True or False?
True! The wording here was taken from one of our readers’ responses, by the way (thank you, Robin). There are a good number of those protective factors, the most well-known of which is passing on immune cells and cell-like things; in other words, immune-related information being passed from parent* to child.
*usually the mother, though in principle it could be someone else and in practice sometimes it is; the only real requirements are that the other person be healthy, lactating, and willing.
As for immune benefits, see for example:
Perspectives on Immunoglobulins in Colostrum and Milk
And for that matter, also:
(Colostrum is simply the milk that is produced for a short period after giving birth; the composition of milk will tend to change later)
In any case, immunoglobulin A is a very important component in breast milk (colostrum and later), as well as lactoferrin (has an important antimicrobial effect and is good for the newborn’s gut), and a plethora of cytokines:
As for that about the gut, lactoferrin isn’t the only breast milk component that benefits this, by far, and there’s a lot that can’t be replicated yet:
Human Breast Milk and the Gastrointestinal Innate Immune System
As long as your infant/child is nutritiously fed, it shouldn’t matter if it comes from breast or formula: True or False?
False! Formula milk will not convey those immune benefits.
This doesn’t mean that formula-feeding is neglectful; as several people who commented mentioned*, there are many reasons a person may not be able to breastfeed, and they certainly should not be shamed for that.
*(including the reader whose words we borrowed for this True/False item; the words we quoted above were prefaced with: “Not everyone is able to breastfeed for many different reasons”)
But, while formula milk is a very good second choice, and absolutely a respectable choice if breast milk isn’t an option (or an acceptable option) for whatever reason, it still does not convey all the health benefits of breast milk—yet! The day may come when they’ll find a way to replicate the immune benefits, but today is not that day.
They both have their strengths and weaknesses: True or False?
True! But formula’s strengths are only in the category of convenience and sometimes necessity—formula conveys no health benefits that breast milk could not do better, if available.
For many babies, formula means they get to eat, when without it they would starve due to non-availability of breast milk. That’s a pretty important role!
Note also: this is a health science publication, not a philosophical publication, but we’d be remiss not to mention one thing; let’s bring it in under the umbrella of sociology:
The right to bodily autonomy continues to be the right to bodily autonomy even if somebody else wants/needs something from your body.
Therefore, while there are indeed many good reasons for not being able to breastfeed, or even just not being safely* able to breastfeed, it is at the very least this writer’s opinion that nobody should be pressed to give their reason for not breastfeeding; “no” is already a sufficient answer.
*Writer’s example re safety: when I was born, my mother was on such drugs that it would have been a very bad idea for her to breastfeed me. There are plenty of other possible reasons why it might be unsafe for someone one way or another, but “on drugs that have a clear ‘do not take while pregnant or nursing’ warning” is a relatively common one.
All that said, for those who are willing and safely able, the science is clear: breast is best.
Want to read more?
The World Health Organization has a wealth of information (including explanations of its recommendations of, where possible, exclusive breastfeeding for the first 6 months, ideally continuing some breastfeeding for the first 2 years), here:
World Health Organization | Breastfeeding
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Food for Thought – by Lorraine Perretta
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What are “brain foods”? If you think for a moment, you can probably list a few. What this book does is better.
As well as providing the promised 50 recipes (which themselves are varied, good, and easy), Perretta explains the science of very many brain-healthy ingredients. Not just that, but also the science of a lot of brain-unhealthy ingredients. In the latter case, probably things you already knew to stay away from, but still, it’s a good reminder of one more reason why.
Nor does she merely sort things into brain-healthy (or brain-unhealthy, or brain-neutral), but rather she gives lists of “this for memory” and “this against depression” and “this for cognition” and “this against stress” and so forth.
Perhaps the greatest value of this book is in that; her clear explanations with science that’s simplified but not dumbed down. The recipes are definitely great too, though!
Bottom line: if you’d like to eat more for brain health, this book will give you many ways of doing so
Click here to check out Food for Thought, and upgrade your recipes!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Who Initiates Sex & Why It Matters
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In an ideal world, it wouldn’t matter any more than who first says “let’s get something to eat” when hungry. But in reality, it can cause serious problems on both sides:
Fear and loathing?
The person who initiates gets the special prize of an n% chance of experiencing rejection, and then what? Try again, and again, and risk seeming pushy? Or leave the ball in the other person’s court, where it may then go untouched for the next few months, because (in the most positive scenario) they were waiting for you to initiate at a better time for them?
The person who does not initiate, and/but does not want sex at that time, gets the special prize of either making their partner feel unwanted, insecure, and perhaps unloved, or else grudgingly consenting to sex that’s going to be no fun while your heart’s not in it, and thus create the same end result plus you had an extra bad experience?
So, that sucks all around:
- Initiating touch (sex or cuddling) can feel like a test of being wanted, whereupon a lack of initiation or response may be misinterpreted as a lack of love or appreciation.
- Meanwhile, non-reciprocation might stem from exhaustion or unrelated issues. For many, it’s a physiological lottery.
10almonds note: not discussed in this video, but for many couples, problems can also arise because one partner or another just isn’t showing up with the expected physical signs of physiological arousal, so even if they say (and mean!) an enthusiastic “yes”, their body’s signs get misread as a “not really, though”, resulting in one partner feeling rejected, and both feeling inadequate—on account of something that was completely unrelated to how the person actually felt about the prospect of sex*.
*Sometimes, physiological arousal will simply not accompany psychological arousal, no matter how sincere the latter. And on the flipside, sometimes the signs of physiological arousal will just show up without psychological arousal. The human body is just like that sometimes. We all must listen to our partners’ words, not their genitals!
The solution to this problem is thus the same as the solution to the rest of the problem that is discussed in the video, and it’s: good communication.
That can be easier said than done, of course—not everyone is at their most eloquent in such situations! Which is why it can be important to have those conversations first outside of the bedroom when the stakes are low/non-existent.
Even with the best communication, a more general, overarching non-reciprocity (real or perceived) of sexual desire can cause bitterness, resentment, and can ultimately be relationship-ending if a resolution that’s acceptable to everyone involved is not found.
Ultimately, the work as a couple must begin from within as individuals—addressing self-worth issues to better navigate love and intimacy.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Relationships: When To Stick It Out & When To Call It Quits
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: