How does cancer spread to other parts of the body?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
All cancers begin in a single organ or tissue, such as the lungs or skin. When these cancers are confined in their original organ or tissue, they are generally more treatable.
But a cancer that spreads is much more dangerous, as the organs it spreads to may be vital organs. A skin cancer, for example, might spread to the brain.
This new growth makes the cancer much more challenging to treat, as it can be difficult to find all the new tumours. If a cancer can invade different organs or tissues, it can quickly become lethal.
When cancer spreads in this way, it’s called metastasis. Metastasis is responsible for the majority (67%) of cancer deaths.
Cells are supposed to stick to surrounding tissue
Our bodies are made up of trillions of tiny cells. To keep us healthy, our bodies are constantly replacing old or damaged cells.
Each cell has a specific job and a set of instructions (DNA) that tells it what to do. However, sometimes DNA can get damaged.
This damage might change the instructions. A cell might now multiply uncontrollably, or lose a property known as adherence. This refers to how sticky a cell is, and how well it can cling to other surrounding cells and stay where it’s supposed to be.
If a cancer cell loses its adherence, it can break off from the original tumour and travel through the bloodstream or lymphatic system to almost anywhere. This is how metastasis happens.
Many of these travelling cancer cells will die, but some will settle in a new location and begin to form new cancers.
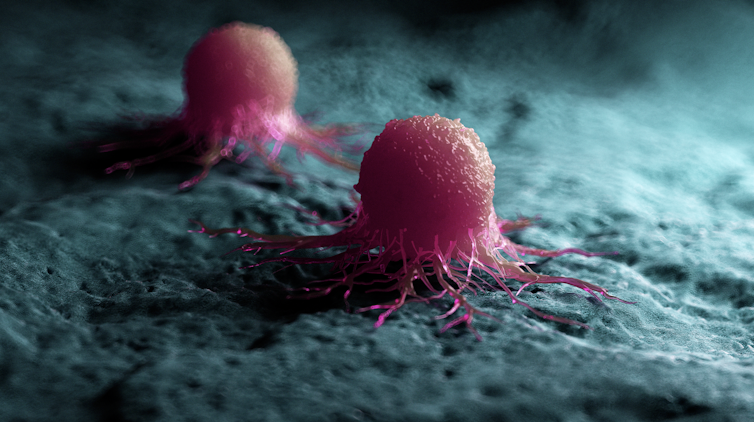
Scipro/Shutterstock
Particular cancers are more likely to metastasise to particular organs that help support their growth. Breast cancers commonly metastasise to the bones, liver, and lungs, while skin cancers like melanomas are more likely to end up in the brain and heart.
Unlike cancers which form in solid organs or tissues, blood cancers like leukaemia already move freely through the bloodstream, but can escape to settle in other organs like the liver or brain.
When do cancers metastasise?
The longer a cancer grows, the more likely it is to metastasise. If not caught early, a patient’s cancer may have metastasised even before it’s initially diagnosed.
Metastasis can also occur after cancer treatment. This happens when cancer cells are dormant during treatment – drugs may not “see” those cells. These invisible cells can remain hidden in the body, only to wake up and begin growing into a new cancer months or even years later.
For patients who already have cancer metastases at diagnosis, identifying the location of the original tumour – called the “primary site” – is important. A cancer that began in the breast but has spread to the liver will probably still behave like a breast cancer, and so will respond best to an anti-breast cancer therapy, and not anti-liver cancer therapy.
As metastases can sometimes grow faster than the original tumour, it’s not always easy to tell which tumour came first. These cancers are called “cancers of unknown primary” and are the 11th most commonly diagnosed cancers in Australia.
One way to improve the treatment of metastatic cancer is to improve our ways of detecting and identifying cancers, to ensure patients receive the most effective drugs for their cancer type.
What increases the chances of metastasis and how can it be prevented?
If left untreated, most cancers will eventually acquire the ability to metastasise.
While there are currently no interventions that specifically prevent metastasis, cancer patients who have their tumours surgically removed may also be given chemotherapy (or other drugs) to try and weed out any hidden cancer cells still floating around.
The best way to prevent metastasis is to diagnose and treat cancers early. Cancer screening initiatives such as Australia’s cervical, bowel, and breast cancer screening programs are excellent ways to detect cancers early and reduce the chances of metastasis.

Peakstock/Shutterstock
New screening programs to detect cancers early are being researched for many types of cancer. Some of these are simple: CT scans of the body to look for any potential tumours, such as in England’s new lung cancer screening program.
Using artificial intelligence (AI) to help examine patient scans is also possible, which might identify new patterns that suggest a cancer is present, and improve cancer detection from these programs.
More advanced screening methods are also in development. The United States government’s Cancer Moonshot program is currently funding research into blood tests that could detect many types of cancer at early stages.
One day there might even be a RAT-type test for cancer, like there is for COVID.
Will we be able to prevent metastasis in the future?
Understanding how metastasis occurs allows us to figure out new ways to prevent it. One idea is to target dormant cancer cells and prevent them from waking up.
Directly preventing metastasis with drugs is not yet possible. But there is hope that as research efforts continue to improve cancer therapies, they will also be more effective at treating metastatic cancers.
For now, early detection is the best way to ensure a patient can beat their cancer.![]()
Sarah Diepstraten, Senior Research Officer, Blood Cells and Blood Cancer Division, Walter and Eliza Hall Institute and John (Eddie) La Marca, Senior Resarch Officer, Walter and Eliza Hall Institute
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Blueberries vs Banana – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing blueberries to banana, we picked the banana.
Why?
Surprise, that which is more expensive is not always commensurately more healthy! A lot of the price difference between bananas and blueberries comes down to:
- ease of transport (unripe bananas can be transported quite easily without too much risk of bruising; unripe blueberries can’t even be usefully picked)
- shelf-life (unripe bananas will take their time to ripen; the already-ripe blueberries will often go bad very quickly)
For this reason, frozen blueberries are a great option for budget-friendly berries. But, onto the comparisons:
In terms of macros, bananas have slightly more protein, carbs, and fiber, and the slightly lower glycemic index. Really, both are good, but by the numbers, bananas win.
When it comes to vitamins, blueberries have more of vitamins B1, C, E, and K, while bananas have more of vitamins A, B2, B3, B5, B6, B9, and choline. Another win for bananas, though of course we could quibble which vitamins are most likely to be not found in sufficient abundance in the rest of one’s diet, but as it is, we just compared the nutrients head-to-head without trying to guess the rest of someone’s diet.
In the category of minerals, blueberries have more calcium and manganese, while bananas have more copper, magnesium, phosphorus, potassium, and selenium. Another win for bananas.
As for polyphenols, this is where blueberries shine, with a lot more than bananas (difficult to calculate exactly due to variations, but, in the order of hundreds of times more). A win for blueberries this time.
Adding up the section gives us an overall win for bananas, but by all means enjoy either or both; perhaps even together!
Want to learn more?
You might like to read:
Blueberry & Banana Collagen Baked Oats ← You will love this recipe! And… Good news for vegans/vegetarians: while we include an optional tablespoon of collagen powder in this recipe, the whole recipe is already geared around collagen synthesis, so it’s very collagen-boosting even with just the plants, providing collagen’s building blocks of protein, zinc, and vitamins C and D (your miraculous body will use these to assemble the collagen inside you).
Enjoy!
Share This Post
-

A Tale Of Two Cinnamons
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cinnamon’s Health Benefits (But Watch Out!)
Cinnamon is enjoyed for its sweet and punchy flavor. It also has important health properties!
Let’s take a look at the science…
A Tale Of Two Cinnamons
In your local supermarket, there is likely “cinnamon” and if you’re lucky, also “sweet cinnamon”. The difference between these is critical to understand before we continue:
“Cinnamon” = Cinnamomum cassia or Cinnamomum aromaticum. This is cheapest and most readily available. It has a relatively high cinnamaldehyde content, and a high coumarin content.
“Sweet cinnamon” Cinnamomum verum or Cinnamomum zeylanicum. It has a lower cinnamaldehyde content, and/but a much lower (almost undetectable) coumarin content.
You may be wondering: what’s with the “or” in both of those cases? Each simply has two botanical names in use. It’s inconvenient and confusing, but that’s how it is.
Great! What’s cinnamaldehyde and what’s coumarin?
Cinnamaldehyde is what gives cinnamon its “spice” aspect; it’s strong and fragrant. It also gives cinnamon most of its health benefits.
As a quick aside: it’s also used as the flavoring element in cinnamon flavored vapes, and in that form, it can cause health problems. So do eat it, but we recommend not to vape it.
Coumarin is toxic in large quantities.
The recommended safe amount is 0.1mg/kg, so you could easily go over this with a couple of teaspoons of cassia cinnamon:
Toxicology and risk assessment of coumarin: focus on human data
…while in Sweet/True/Ceylon cinnamon, those levels are almost undetectable:
Medicinal properties of ‘true’ cinnamon (Cinnamomum zeylanicum): a systematic review
If you have a cinnamon sensitivity, it is likely, but not necessarily, tied to the coumarin content rather than the cinnamaldehyde content.
Summary of this section before moving on:
“Cinnamon”, or cassia cinnamon, has about 50% stronger health benefits than “Sweet Cinnamon”, also called Ceylon cinnamon.
“Cinnamon”, or cassia cinnamon, has about 250% stronger health risks than “Sweet Cinnamon”, also called Ceylon cinnamon.
The mathematics here is quite simple; sweet cinnamon is the preferred way to go.
The Health Benefits
We spent a lot of time/space today looking at the differences. We think this was not only worth it, but necessary. However, that leaves us with less time/space for discussing the actual benefits. We’ll summarize, with links to supporting science:
“Those three things that almost always go together”:
Heart and blood benefits:
- Reduces triglyceride levels
- Reduces high blood pressure
- Reduces insulin insensitivity
- Reduces fasting blood sugar levels
Neuroprotective benefits:
The science does need more testing in these latter two, though.
Where to get it?
You may be able to find sweet cinnamon in your local supermarket, or if you prefer capsule form, here’s an example product on Amazon
Enjoy!
Share This Post
-

Never Too Old?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Age Limits On Exercise?
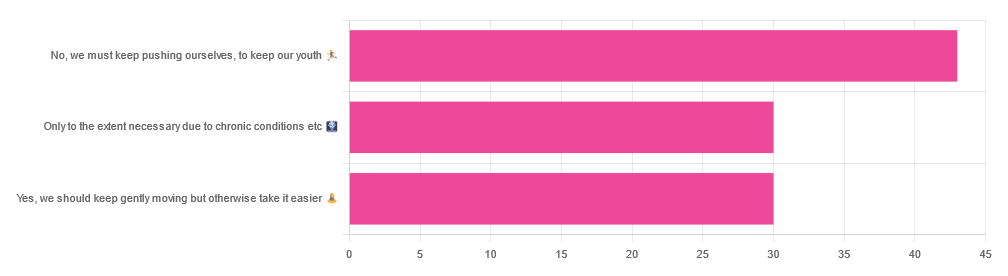
In Tuesday’s newsletter, we asked you your opinion on whether we should exercise less as we get older, and got the above-depicted, below-described, set of responses:

- About 42% said “No, we must keep pushing ourselves, to keep our youth“
- About 29% said “Only to the extent necessary due to chronic conditions etc”
- About 29% said “Yes, we should keep gently moving but otherwise take it easier”
One subscriber who voted for “No, we must keep pushing ourselves, to keep our youth“ wrote to add:
❝I’m 71 and I push myself. I’m not as fast or strong as I used to be but, I feel great when I push myself instead of going through the motions. I listen to my body!❞
~ 10almonds subscriber
One subscriber who voted for “Only to the extent necessary due to chronic conditions etc” wrote to add:
❝It’s never too late to get stronger. Important to keep your strength and balance. I am a Silver Sneakers instructor and I see first hand how helpful regular exercise is for seniors.❞
~ 10almonds subscriber
One subscriber who voted to say “Yes, we should keep gently moving but otherwise take it easier” wrote to add:
❝Keep moving but be considerate and respectful of your aging body. It’s a time to find balance in life and not put yourself into a positon to damage youself by competing with decades younger folks (unless you want to) – it will take much longer to bounce back.❞
~ 10almonds subscriber
These will be important, because we’ll come back to them at the end.
So what does the science say?
Endurance exercise is for young people only: True or False?
False! With proper training, age is no barrier to serious endurance exercise.
Here’s a study that looked at marathon-runners of various ages, and found that…
- the majority of middle-aged and elderly athletes have training histories of less than seven years of running
- there are virtually no relevant running time differences (p<0.01) per age in marathon finishers from 20 to 55 years
- after 55 years, running times did increase on average, but not consistently (i.e. there were still older runners with comparable times to the younger age bracket)
The researchers took this as evidence of aging being indeed a biological process that can be sped up or slowed down by various lifestyle factors.
See also:
Age & Aging: What Can (And Can’t) We Do About It?
this covers the many aspects of biological aging (it’s not one number, but many!) and how our various different biological ages are often not in sync with each other, and how we can optimize each of them that can be optimized
Resistance training is for young people only: True or False?
False! In fact, it’s not only possible for older people, but is also associated with a reduction in all-cause mortality.
Specifically, those who reported strength-training at least once per week enjoyed longer lives than those who did not.
You may be thinking “is this just the horse-riding thing again, where correlation is not causation and it’s just that healthier people (for other reasons) were able to do strength-training more, rather than the other way around?“
…which is a good think to think of, so well-spotted if you were thinking that!
But in this case no; the benefits remained when other things were controlled for:
❝Adjusted for demographic variables, health behaviors and health conditions, a statistically significant effect on mortality remained.
Although the effects on cardiac and cancer mortality were no longer statistically significant, the data still pointed to a benefit.
Importantly, after the physical activity level was controlled for, people who reported strength exercises appeared to see a greater mortality benefit than those who reported physical activity alone.❞
See the study: Is strength training associated with mortality benefits? A 15 year cohort study of US older adults
And a pop-sci article about it: Strength training helps older adults live longer
Closing thoughts
As it happens… All three of the subscribers we quoted all had excellent points!
Because in this case it’s less a matter of “should”, and more a selection of options:
- We (most of us, at least) can gain/regain/maintain the kind of strength and fitness associated with much younger people, and we need not be afraid of exercising accordingly (assuming having worked up to such, not just going straight from couch to marathon, say).
- We must nevertheless be mindful of chronic conditions or even passing illnesses/injuries, but that goes for people of any age
- We also can’t argue against a “safety first” cautious approach to exercise. After all, sure, maybe we can run marathons at any age, but that doesn’t mean we have to. And sure, maybe we can train to lift heavy weights, but if we’re content to be able to carry the groceries or perhaps take our partner’s weight in the dance hall (or the bedroom!), then (if we’re also at least maintaining our bones and muscles at a healthy level) that’s good enough already.
Which prompts the question, what do you want to be able to do, now and years from now? What’s important to you?
For inspiration, check out: Train For The Event Of Your Life!
Take care!
Share This Post
-
Women are less likely to receive CPR than men. Training on manikins with breasts could help
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If someone’s heart suddenly stops beating, they may only have minutes to live. Doing CPR (cardiopulmonary resusciation) can increase their chances of survival. CPR makes sure blood keeps pumping, providing oxygen to the brain and vital organs until specialist treatment arrives.
But research shows bystanders are less likely to intervene to perform CPR when that person is a woman. A recent Australian study analysed 4,491 cardiac arrests between 2017–19 and found bystanders were more likely to give CPR to men (74%) than women (65%).
Could this partly be because CPR training dummies (known as manikins) don’t have breasts? Our new research looked at manikins available worldwide to train people in performing CPR and found 95% are flat-chested.
Anatomically, breasts don’t change CPR technique. But they may influence whether people attempt it – and hesitation in these crucial moments could mean the difference between life and death.
Pixel-Shot/Shutterstock Heart health disparities
Cardiovascular diseases – including heart disease, stroke and cardiac arrest – are the leading cause of death for women across the world.
But if a woman has a cardiac arrest outside hospital (meaning her heart stops pumping properly), she is 10% less likely to receive CPR than a man. Women are also less likely to survive CPR and more likely to have brain damage following cardiac arrests.
Bystanders are less likely to intervene if a woman needs CPR, compared to a man. doublelee/Shutterstock These are just some of many unequal health outcomes women experience, along with transgender and non-binary people. Compared to men, their symptoms are more likely to be dismissed or misdiagnosed, or it may take longer for them to receive a diagnosis.
Bystander reluctance
There is also increasing evidence women are less likely to receive CPR compared to men.
This may be partly due to bystander concerns they’ll be accused of sexual harassment, worry they might cause damage (in some cases based on a perception women are more “frail”) and discomfort about touching a woman’s breast.
Bystanders may also have trouble recognising a woman is experiencing a cardiac arrest.
Even in simulations of scenarios, researchers have found those who intervened were less likely to remove a woman’s clothing to prepare for resuscitation, compared to men. And women were less likely to receive CPR or defibrillation (an electric charge to restart the heart) – even when the training was an online game that didn’t involve touching anyone.
There is evidence that how people act in resuscitation training scenarios mirrors what they do in real emergencies. This means it’s vital to train people to recognise a cardiac arrest and be prepared to intervene, across genders and body types.
Skewed to male bodies
Most CPR training resources feature male bodies, or don’t specify a sex. If the bodies don’t have breasts, it implies a male default.
For example, a 2022 study looking at CPR training across North, Central and South America, found most manikins available were white (88%), male (94%) and lean (99%).
It’s extremely rare for a manikin to have breasts or a larger body. M Isolation photo/Shutterstock These studies reflect what we see in our own work, training other health practitioners to do CPR. We have noticed all the manikins available to for training are flat-chested. One of us (Rebecca) found it difficult to find any training manikins with breasts.
A single manikin with breasts
Our new research investigated what CPR manikins are available and how diverse they are. We identified 20 CPR manikins on the global market in 2023. Manikins are usually a torso with a head and no arms.
Of the 20 available, five (25%) were sold as “female” – but only one of these had breasts. That means 95% of available CPR training manikins were flat-chested.
We also looked at other features of diversity, including skin tone and larger bodies. We found 65% had more than one skin tone available, but just one was a larger size body. More research is needed on how these aspects affect bystanders in giving CPR.
Breasts don’t change CPR technique
CPR technique doesn’t change when someone has breasts. The barriers are cultural. And while you might feel uncomfortable, starting CPR as soon as possible could save a life.
Signs someone might need CPR include not breathing properly or at all, or not responding to you.
To perform effective CPR, you should:
- put the heel of your hand on the middle of their chest
- put your other hand on the top of the first hand, and interlock fingers (keep your arms straight)
- press down hard, to a depth of about 5cm before releasing
- push the chest at a rate of 100-120 beats per minute (you can sing a song) in your head to help keep time!)
https://www.youtube.com/embed/Plse2FOkV4Q?wmode=transparent&start=94 An example of how to do CPR – with a flat-chested manikin.
What about a defibrillator?
You don’t need to remove someone’s bra to perform CPR. But you may need to if a defibrillator is required.
A defibrillator is a device that applies an electric charge to restore the heartbeat. A bra with an underwire could cause a slight burn to the skin when the debrillator’s pads apply the electric charge. But if you can’t remove the bra, don’t let it delay care.
What should change?
Our research highlights the need for a range of CPR training manikins with breasts, as well as different body sizes.
Training resources need to better prepare people to intervene and perform CPR on people with breasts. We also need greater education about women’s risk of getting and dying from heart-related diseases.
Jessica Stokes-Parish, Assistant Professor in Medicine, Bond University and Rebecca A. Szabo, Honorary Senior Lecturer in Critical Care and Obstetrics, Gynaecology and Newborn Health, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Is owning a dog good for your health?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australia loves dogs. We have one of the highest rates of pet ownership in the world, and one in two households has at least one dog.
But are they good for our health?
Mental health is the second-most common reason cited for getting a dog, after companionship. And many of us say we “feel healthier” for having a dog – and let them sleep in our bedroom.
Here’s what it means for our physical and mental health to share our homes (and doonas) with our canine companions.
Pogodina Natalia/Shutterstock Are there physical health benefits to having a dog?
Having a dog is linked to lower risk of death over the long term. In 2019, a systematic review gathered evidence published over 70 years, involving nearly four million individual medical cases. It found people who owned a dog had a 24% lower risk of dying from any cause compared to those who did not own a dog.
Having a dog may help lower your blood pressure through more physical activity. Barnabas Davoti/Pexels Dog ownership was linked to increased physical activity. This lowered blood pressure and helped reduce the risk of stroke and heart disease.
The review found for those with previous heart-related medical issues (such as heart attack), living with a dog reduced their subsequent risk of dying by 35%, compared to people with the same history but no dog.
Another recent UK study found adult dog owners were almost four times as likely to meet daily physical activity targets as non-owners. Children in households with a dog were also more active and engaged in more unstructured play, compared to children whose family didn’t have a dog.
Exposure to dirt and microbes carried in from outdoors may also strengthen immune systems and lead to less use of antibiotics in young children who grow up with dogs.
Children in households with a dog were often more active. Maryshot/Shutterstock Health risks
However, dogs can also pose risks to our physical health. One of the most common health issues for pet owners is allergies.
Dogs’ saliva, urine and dander (the skin cells they shed) can trigger allergic reactions resulting in a range of symptoms, from itchy eyes and runny nose to breathing difficulties.
A recent meta-analysis pooled data from nearly two million children. Findings suggested early exposure to dogs may increase the risk of developing asthma (although not quite as much as having a cat does). The child’s age, how much contact they have with the dog and their individual risk all play a part.
Slips, trips and falls are another risk – more people fall over due to dogs than cats.
Having a dog can also expose you to bites and scratches which may become infected and pose a risk for those with compromised immune systems. And they can introduce zoonotic diseases into your home, including ring worm and Campylobacter, a disease that causes diarrhoea.
For those sharing the bed there is an elevated the risk of allergies and picking up ringworm. It may result in lost sleep, as dogs move around at night.
On the other hand some owners report feeling more secure while co-sleeping with their dogs, with the emotional benefit outweighing the possibility of sleep disturbance or waking up with flea bites.
Proper veterinary care and hygiene practices are essential to minimise these risks.
Many of us don’t just share a home with a dog – we let them sleep in our beds. Claudia Mañas/Unsplash What about mental health?
Many people know the benefits of having a dog are not only physical.
As companions, dogs can provide significant emotional support helping to alleviate symptoms of anxiety, depression and post-traumatic stress. Their presence may offer comfort and a sense of purpose to individuals facing mental health challenges.
Loneliness is a significant and growing public health issue in Australia.
In the dog park and your neighbourhood, dogs can make it easier to strike up conversations with strangers and make new friends. These social interactions can help build a sense of community belonging and reduce feelings of social isolation.
For older adults, dog walking can be a valuable loneliness intervention that encourages social interaction with neighbours, while also combating declining physical activity.
However, if you’re experiencing chronic loneliness, it may be hard to engage with other people during walks. An Australian study found simply getting a dog was linked to decreased loneliness. People reported an improved mood – possibly due to the benefits of strengthening bonds with their dog.
Walking a dog can make it easier to talk to people in your neighbourhood. KPegg/Shutterstock What are the drawbacks?
While dogs can bring immense joy and numerous health benefits, there are also downsides and challenges. The responsibility of caring for a dog, especially one with behavioural issues or health problems, can be overwhelming and create financial stress.
Dogs have shorter lifespans than humans, and the loss of a beloved companion can lead to depression or exacerbate existing mental health conditions.
Lifestyle compatibility and housing conditions also play a significant role in whether having a dog is a good fit.
The so-called pet effect suggests that pets, often dogs, improve human physical and mental health in all situations and for all people. The reality is more nuanced. For some, having a pet may be more stressful than beneficial.
Importantly, the animals that share our homes are not just “tools” for human health. Owners and dogs can mutually benefit when the welfare and wellbeing of both are maintained.
Tania Signal, Professor of Psychology, School of Health, Medical and Applied Sciences, CQUniversity Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Junk Food Turns Public Villain as Power Shifts in Washington
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The new Trump administration could be coming for your snacks.
For years, the federal government has steered clear of regulating junk food, fast food, and ultra-processed food.
Now attitudes are changing. Some members of President-elect Donald Trump’s inner circle are gearing up to battle “Big Food,” or the companies that make most of the food and beverages consumed in the United States. Nominees for top health agencies are taking aim at ultra-processed foods that account for an estimated 70% of the nation’s food supply. Based on recent statements, a variety of potential politically charged policy options to regulate ultra-processed food may land on the Trump team menu, including warning labels, changes to agribusiness subsidies, and limits on which products consumers can buy with government food aid.
The push to reform the American diet is being driven largely by conservatives who have taken up the cause that has long been a darling of the left. Trump supporters such as Robert F. Kennedy Jr., whose controversial nomination to lead the Department of Health and Human Services still faces Senate confirmation, are embracing a concept that champions natural foods and alternative medicine. It’s a movement they’ve dubbed “MAHA,” or Make America Healthy Again. Their interest has created momentum because their goals have fairly broad bipartisan support even amid a bitterly divided Congress in which lawmakers from both sides of the aisle focused on the issue last year.
It’s likely to be a pitched battle because the food industry wields immense political influence and has successfully thwarted previous efforts to regulate its products or marketing. The category of “food processing and sales companies,” which includes Tyson Foods and Nestle SA, tallied $26.7 million in spending on lobbying in 2024, according to OpenSecrets. That’s up from almost $10 million in 1998.
“They have been absolutely instrumental and highly, highly successful at delaying any regulatory effectiveness in America,” said Laura Schmidt, a health policy professor at the University of California-San Francisco. “It really does feel like there needs to be a moment of reckoning here where people start asking the question, ‘Why do we have to live like this?’”
“Ultra-processed food” is a widely used term that means different things to different people and is used to describe items ranging from sodas to many frozen meals. These products often contain added fats, starches, and sugars, among other things. Researchers say consumption of ultra-processed foods is linked — in varying levels of intensity — to chronic conditions like diabetes, cancer, mental health problems, and early death.
Nutrition and health leaders are optimistic that a reckoning is already underway. Kennedy has pledged to remove processed foods from school lunches, restrict certain food additives such as dyes in cereal, and shift federal agricultural subsidies away from commodity crops widely used in ultra-processed foods.
The intensifying focus in Washington has triggered a new level of interest on the legal front as lawyers explore cases to take on major foodmakers for selling products they say result in chronic disease.
Bryce Martinez, now 18, filed a lawsuit in December against almost a dozen foodmakers such as Kraft Heinz, The Coca-Cola Co., and Nestle USA. He developed diabetes and non-alcoholic fatty liver disease by age 16, and is seeking to hold them accountable for his illnesses. According to the suit, filed in the Philadelphia Court of Common Pleas, the companies knew or should have known ultra-processed foods were harmful and addictive.
The lawsuit noted that Martinez grew up eating heavily advertised, brand-name foods that are staples of the American diet — sugary soft drinks, Cheerios and Lucky Charms, Skittles and Snickers, frozen and packaged dinners, just to name a few.
Nestle, Coca-Cola, and Kraft Heinz didn’t return emails seeking comment for this article. The Consumer Brands Association, a trade association for makers of consumer packaged goods, disputed the allegations.
“Attempting to classify foods as unhealthy simply because they are processed, or demonizing food by ignoring its full nutrient content, misleads consumers and exacerbates health disparities,” said Sarah Gallo, senior vice president of product policy, in a statement.
Other law firms are on the hunt for children or adults who believe they were harmed by consuming ultra-processed foods, increasing the likelihood of lawsuits.
One Indiana personal injury firm says on its website that “we are actively investigating ultra processed food (UPF) cases.” Trial attorneys in Texas also are looking into possible legal action against the federal regulators they say have failed to police ultra-processed foods.
“If you or your child have suffered health problems that your doctor has linked directly to the consumption of ultra-processed foods, we want to hear your story,” they say on their website.
Meanwhile, the FDA on Jan. 14 announced it is proposing to require a front-of-package label to appear on most packaged foods to make information about a food’s saturated fat, sodium, and added sugar content easily visible to consumers.
And on Capitol Hill, Sens. Bernie Sanders (I-Vt.), Ron Johnson (R-Wis.), and Cory Booker (D-N.J.) are sounding the alarm over ultra-processed food. Sanders introduced legislation in 2024 that could lead to a federal ban on junk food advertising to children, a national education campaign, and labels on ultra-processed foods that say the products aren’t recommended for children. Booker cosigned the legislation along with Sens. Peter Welch (D-Vt.) and John Hickenlooper (D-Colo.).
The Senate Committee on Health, Education, Labor and Pensions held a December hearing examining links between ultra-processed food and chronic disease during which FDA Commissioner Robert Califf called for more funding for research.
Food companies have tapped into “the same neural circuits that are involved in opioid addiction,” Califf said at the hearing.
Sanders, who presided over the hearing, said there’s “growing evidence” that “these foods are deliberately designed to be addictive,” and he asserted that ultra-processed foods have driven epidemics of diabetes and obesity, and hundreds of billions of dollars in medical expenses.
Research on food and addiction “has accumulated to the point where it’s reached a critical mass,” said Kelly Brownell, an emeritus professor at Stanford who is one of the editors of a scholarly handbook on the subject.
Attacks from three sides — lawyers, Congress, and the incoming Trump administration, all seemingly interested in taking up the fight — could lead to enough pressure to challenge Big Food and possibly spur better health outcomes in the U.S., which has the lowest life expectancy among high-income countries.
“Maybe getting rid of highly processed foods in some things could actually flip the switch pretty quickly in changing the percentage of the American public that are obese,” said Robert Redfield, a virologist who led the Centers for Disease Control and Prevention during the previous Trump administration, in remarks at a December event hosted by the Heritage Foundation, a conservative think tank.
Claims that Big Food knowingly manufactured and sold addictive and harmful products resemble the claims leveled against Big Tobacco before the landmark $206 billion settlement was reached in 1998.
“These companies allegedly use the tobacco industry’s playbook to target children, especially Black and Hispanic children, with integrated marketing tie-ins with cartoons, toys, and games, along with social media advertising,” Rene Rocha, one of the lawyers at Morgan & Morgan representing Martinez, told KFF Health News.
The 148-page Martinez lawsuit against foodmakers draws from documents made public in litigation against tobacco companies that owned some of the biggest brands in the food industry.
Similar allegations were made against opioid manufacturers, distributors, and retailers before they agreed to pay tens of billions of dollars in a 2021 settlement with states.
The FDA ultimately put restrictions on the labeling and marketing of tobacco, and the opioid epidemic led to legislation that increased access to lifesaving medications to treat addiction.
But the Trump administration’s zeal in taking on Big Food may face unique challenges.
The ability of the FDA to impose regulation is hampered in part by funding. While the agency’s drug division collects industry user fees, its division of food relies on a more limited budget determined by Congress.
Change can take time because the agency moves at what some critics call a glacial pace. Last year, the FDA revoked a regulation allowing brominated vegetable oil in food products. The agency determined in 1970 that the additive was not generally recognized as safe.
Efforts to curtail the marketing of ultra-processed food could spur lawsuits alleging that any restrictions violate commercial speech protected by the First Amendment. And Kennedy — if he is confirmed as HHS secretary — may struggle to get support from a Republican-led Congress that champions less federal regulation and a president-elect who during his previous term served fast food in the White House.
“The question is, will RFK be able to make a difference?” said David L. Katz, a doctor who founded True Health Initiative, a nonprofit group that combats public health misinformation. “No prior administration has done much in this space, and RFK is linked to a particularly anti-regulatory administration.”
Meanwhile, the U.S. population is recognized as among the most obese in the world and has the highest rate of people with multiple chronic conditions among high-income countries.
“There is a big grassroots effort out there because of how sick we are,” said Jerold Mande, who served as deputy undersecretary for food safety at the Department of Agriculture from 2009 to 2011. “A big part of it is people shouldn’t be this sick this young in their lives. You’re lucky if you get to 18 without a chronic disease. It’s remarkable.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: