Deskbound – by Kelly Starrett and Glen Cordoza
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve all heard that “sitting is the new smoking”, and whether or not that’s an exaggeration (the jury’s out), one thing that is clear is that sitting is very bad.
Popular advice is “here’s how to sit with good posture and stretch your neck sometimes”… but that advice tends to come from companies that pay people to sit for a long time. They might not be the a very unbiased source.
Starrett and Cordoza offer better. After one opening chapter covering the multifarious ways sitting ruins our health, the rest of the book is all advice, covering:
- The principles of how the body is supposed to be
- The most important movements that we should be doing
- A dynamic workstation setup
- This is great, because “get a standing desk” tends to present more questions than answers, and can cause as much harm as good if done wrong
- The authors also cover how to progressively cut down on sitting, rather than try to go cold-turkey.
- They also recognize that not everyone can stand at all, and…
- Optimizing the sitting position, for when we must sit
- Exercises to maintain our general mobility and compensate about as well as we can for the body-unfriendly nature of modern life.
The book is mostly explanations, so at 682 pages, you can imagine it’s not just “get up, lazybones!”. Rather, things are explained in such detail (and with many high-quality medical diagrams) so that we can truly understand them.
Most of us have gone through life knowing we should have “better posture” and “move more”… but without the details, that can be hard to execute correctly, and worse, we can even sabotage our bodies unknowingly with incorrect form.
This book straightens all that out very comprehensively, and we highly recommend it.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Elderberries vs Strawberries – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing elderberries to strawberries, we picked the elderberries.
Why?
It’s hard to go wrong with (non-poisonous) berries, but…
In terms of macros, elderberries have more than 3x the fiber, 2x the carbs, and (for what it’s worth, which is not a lot because it’s very little) the same amount of protein. An easy win for elderberries.
In the category of vitamins, elderberries have (a lot) more of vitamins A, B1, B2, B3, B5, and B6, while strawberries have more of vitamins B9 and C. Another win for elderberries.
When it comes to minerals, elderberries have more calcium, copper, iron, manganese, phosphorus, potassium, and selenium, while strawberries have more magnesium and zinc. One more win for elderberries.
Looking at phytochemicals, both are good but elderberries have more polyphenols, plus some additional beneficial properties (see the link below). A fourth win for elderberries!
Adding up the sections makes for a clear overall win for elderberries, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Herbs For Evidence-Based Health & Healing ← elderberry significantly hastens recovery from upper respiratory viral infections 😎
Enjoy!
Share This Post
-
Do You Do This During Ab Workouts? 5 Mistakes You Might Be Making
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes people will decide to “get abs” and do a lot of whatever their preferred ab exercise might be, but get discouraged when it doesn’t seem to be yielding results.
So, here’s some troubleshooting:
What not to do
Common mistakes include:
- Doing ab exercises you haven’t worked up to: trying advanced moves without the strength or control leads to compensating with hips or back instead of engaging abs.
- Avoiding spinal flexion exercises: while they are indeed an incomplete exercise, completely dismissing crunches or sit-ups robs you of a key movement pattern that effectively trains the abs.
- Not focusing on the correct muscles: performing exercises with poor form (e.g. using hip flexors instead of abs) prevents proper ab activation and may cause pain.
- Training to fatigue instead of focusing on quality: rushing through workouts or overtraining in a single session leads to poor form and reduced results; spread volume throughout the week.
- Prioritizing duration over intensity: holding long planks or doing more reps with low effort doesn’t challenge the abs effectively; shorter, more intense efforts with full engagement are better.
For more on each of these, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Is A Visible Six-Pack Obtainable Regardless Of Genetic Predisposition?
Take care!
Share This Post
-

From Strength to Strength – by Dr. Arthur Brooks
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For most professions, there are ways in which performance can be measured, and the average professional peak varies by profession, but averages are usually somewhere in the 30–45 range, with a pressure to peak between 25–35.
With a peak by age 45 or perhaps 50 at the latest (aside from some statistical outliers, of course), what then to expect at age 50+? Not long after that, there’s a reason for mandatory retirement ages in some professions.
Dr. Brooks examines the case for accepting that rather than fighting it, and/but making our weaknesses into our strengths as we go. If our fluid intelligence slows, our accumulated crystal intelligence (some might call it “wisdom“) can make up for it, for example.
But he also champions the idea of looking outside of ourselves; of the importance of growing and fostering connections; giving to those around us and receiving support in turn; not transactionally, but just as a matter of mutualism of the kind found in many other species besides our own. Indeed, Dr. Brooks gives the example of a grove of aspen trees (hence the cover art of this book) that do exactly that.
The style is very accessible in terms of language but with frequent scientific references, so very much a “best of both worlds” in terms of readability and information-density.
Bottom line: if ever you’ve wondered at what age you might outlive your usefulness, this book will do as the subtitle suggests, and help you carve out your new place.
Click here to check out From Strength To Strength, and find yours!
Share This Post


Related Posts
-
Is It Worth Taking Testosterone In Menopause?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Why are some people recommending taking testosterone for menopause, doesn’t testosterone go up in menopause anyway?❞
A good question with an interesting answer!
To answer the second part first though: testosterone goes up relative to estrogen, and this relative rise of testosterone is part of what’s responsible for androgenic (masculinizing) effects that occur in menopause. This is a process that, if untreated, will continue to have cumulative effects over time for the rest of one’s life.
See also: Menopause, & When Not To Let Your Guard Down
However, while testosterone goes up relative to estrogen, it actually goes down in terms of its own actual numbers—it’s just that testosterone undergoes a slow, gradual decline, while estrogen plummets quickly. Thus, because of the shortage of estrogen to oppose its masculinizing effects, even the technically now-lower total amount of testosterone is able to do more than the previously higher (but opposed by estrogen) levels were able to do.
It’s worth noting that prior to menopause, most women produce about 3x more testosterone than estrogen—it’s just that estrogen is a lot more powerful, mol for mol, mg for mg.
So of course, when that estrogen drops off, testosterone takes the wheel.
See also: What You Should Have Been Told About The Menopause Beforehand
You may be wondering where this testosterone comes from: circulating testosterone is produced by the ovaries (25%) and the adrenal glands (25%), and the rest comes from peripheral conversion of adrenal androgens in fat cells (50%). So, if for example you have a bilateral ovariectomy (also called oophorectomy), then you’ll only actually take a 25% hit to testosterone levels, assuming normal function beforehand. In contrast, someone having a bilateral orchiectomy (also called orchidectomy, and is the removal of the testes) would take a 95% hit to testosterone levels, assuming normal function beforehand.
This is because the ovaries/testes are (usually, aside from in some intersex conditions) specialized to produce mostly estrogen or testosterone, respectively, since they were differentiated during gestation (prior to that, they were the same basic undifferentiated gonads).
Alright, that’s the “doesn’t testosterone go up in menopause anyway?” part covered, now onto the “why are some people recommending taking testosterone for menopause?” part!
Why it gets prescribed
Testosterone—albeit at much lower levels than for men—can be important in women for bone density and muscle mass, cognitive function, mood, sexual function, and energy.
Of those 5 things, there is one that stands out as the reason that’s usually the reason, and that’s…
❝Numerous studies have shown that adding testosterone to hormonal therapy can improve sexual function and general wellbeing among women during their menopause. A recent systematic review and meta-analysis of testosterone treatment in women has provided robust support for a trial of testosterone in women when clinically indicated. In postmenopausal women, testosterone supplementation improved several domains of sexual response, including sexual desire, pleasure, arousal, orgasm, and self-image.❞
You may be wondering: are there any side effects?
And the answer is yes, but with nuance that’s worth understanding:
❝A significant rise in the amount of LDL-cholesterol, and reductions in the amounts of total cholesterol, HDL-cholesterol, and triglycerides, were seen with testosterone administered orally, but not when administered non-orally (e.g. by transdermal patch or cream).
An overall increase in weight* was recorded with testosterone treatment. No effects of testosterone were reported for body composition, musculoskeletal variables, or cognitive measures, although the number of women who contributed data for these outcomes was small.
Testosterone was associated with a significantly greater likelihood of reporting acne and [facial] hair growth, but no serious adverse events were recorded.❞
*However, since no effects were reported for body composition (i.e. they probably didn’t record it), there is a strong chance that the increase in weight was due to testosterone-induced increase in muscle mass, not an increase in fat. If anything, testosterone will tend towards reducing body fat percentage (which is why men’s healthy body fat levels are lower than women’s healthy body fat levels, on average; it is hormones that mediate this).
Read in full: Safety and efficacy of testosterone for women: a systematic review and meta-analysis of randomised controlled trial data
Further,
❝Androgenic Side Effects:
Exogenous androgen given to women in sufficient quantities or for a sufficient duration can promote androgenic side effects such as acne, hirsutism, and, in extreme cases, virilization.
Virilization includes deepening of the voice, clitoromegaly, masculinization of body habitus, and androgenic alopecia.❞
About some those terms:
- Androgenic alopecia = male pattern baldness; actually the same condition as female pattern baldness, but the visual pattern is slightly different according to testosterone levels.
- Clitoromegaly = the clitoris is receiving hormone-mediated instructions to be a penis (bearing in mind, these two organs are analogous, and were the same undifferentiated organ before they were normally differentiated during gestation), and as such, the visible glans clitoris (the part you can see) will grow (up to an inch or so) and start responding to stimulation like a penis instead of like a clitoris (what feels good to it will change accordingly), and the sensation of orgasm will change too. While many people might not mind this, it’s definitely something worth knowing about in advance!
Read in full: The Safety of Testosterone Therapy in Women
So, while we are neither your gynecologist nor your endocrinologist, we can say that the decision-making process might look something like this:
- Are your T-levels in healthy female ranges (5–55ng/DL, or 0.2–1.9nmol/L)? If so, supplementation will not be indicated for most women.
- If they’re below that, are you experiencing any of the problems commonly associated with such, of which the most evident is usually sexual function (where other* causes of loss of sexual function have been ruled out or otherwise adequately addressed)?
- If you are, do you want to fix that more than you want to avoid the side effects of taking T?
*for example, such as discussed in Come As You Are – by Dr. Emily Nagoski
If so, then talking to a potential prescriber seems like a fine option.
But! There is one last problem, and it’s hardly insurmountable, but it is an inconvenience. For obvious reasons, that vast majority of supplemental testosterone produced is made for men. Now, in and of itself this isn’t an issue; it’s the exact same substance and will work the exact same way in you as it will in a man.
However, it does mean that the doses in which testosterone is most readily available, tend to be aimed at delivering testosterone in normal male quantities, which is about 10x what you’ll want (unless your intention is actually to trans your gender, in which case, congratulations on your manliness). This means that, assuming you want a normal female amount of testosterone, then—depending on the source—you may have to get a bit fiddly with it, since you’re going to be taking the amount that the manufacturer expected to be a daily dose, and making that last 10 days.
For example, if you get T-gel in a dispenser at the standard 1.62% percent/20.25mg per pump, then if a man is prescribed 2 pumps per day then you might be prescribed 0.2 pumps per day. It’s the medical equivalent of a recipe that calls for ⅕ of an egg, which is awkward, and does create risks of accidentally taking more than you wanted.
One last note…
If the issue is libido, you might want to try progesterone (if you’re not already on it) before you try testosterone, as that does boost libido, and is also responsible for a number of other important things, including playing a critical role in bone turnover rates:
Progesterone Menopausal HRT: When, Why, And How To Benefit
And if it’s specifically vaginal dryness that’s the issue, often testosterone is the opposite of what’s needed (though DHEA can help):
Vaginal Dryness In Menopause | Causes & Solutions
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Women are less likely to receive CPR than men. Training on manikins with breasts could help
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If someone’s heart suddenly stops beating, they may only have minutes to live. Doing CPR (cardiopulmonary resusciation) can increase their chances of survival. CPR makes sure blood keeps pumping, providing oxygen to the brain and vital organs until specialist treatment arrives.
But research shows bystanders are less likely to intervene to perform CPR when that person is a woman. A recent Australian study analysed 4,491 cardiac arrests between 2017–19 and found bystanders were more likely to give CPR to men (74%) than women (65%).
Could this partly be because CPR training dummies (known as manikins) don’t have breasts? Our new research looked at manikins available worldwide to train people in performing CPR and found 95% are flat-chested.
Anatomically, breasts don’t change CPR technique. But they may influence whether people attempt it – and hesitation in these crucial moments could mean the difference between life and death.

Pixel-Shot/Shutterstock Heart health disparities
Cardiovascular diseases – including heart disease, stroke and cardiac arrest – are the leading cause of death for women across the world.
But if a woman has a cardiac arrest outside hospital (meaning her heart stops pumping properly), she is 10% less likely to receive CPR than a man. Women are also less likely to survive CPR and more likely to have brain damage following cardiac arrests.
Bystanders are less likely to intervene if a woman needs CPR, compared to a man. doublelee/Shutterstock These are just some of many unequal health outcomes women experience, along with transgender and non-binary people. Compared to men, their symptoms are more likely to be dismissed or misdiagnosed, or it may take longer for them to receive a diagnosis.
Bystander reluctance
There is also increasing evidence women are less likely to receive CPR compared to men.
This may be partly due to bystander concerns they’ll be accused of sexual harassment, worry they might cause damage (in some cases based on a perception women are more “frail”) and discomfort about touching a woman’s breast.
Bystanders may also have trouble recognising a woman is experiencing a cardiac arrest.
Even in simulations of scenarios, researchers have found those who intervened were less likely to remove a woman’s clothing to prepare for resuscitation, compared to men. And women were less likely to receive CPR or defibrillation (an electric charge to restart the heart) – even when the training was an online game that didn’t involve touching anyone.
There is evidence that how people act in resuscitation training scenarios mirrors what they do in real emergencies. This means it’s vital to train people to recognise a cardiac arrest and be prepared to intervene, across genders and body types.
Skewed to male bodies
Most CPR training resources feature male bodies, or don’t specify a sex. If the bodies don’t have breasts, it implies a male default.
For example, a 2022 study looking at CPR training across North, Central and South America, found most manikins available were white (88%), male (94%) and lean (99%).
It’s extremely rare for a manikin to have breasts or a larger body. M Isolation photo/Shutterstock These studies reflect what we see in our own work, training other health practitioners to do CPR. We have noticed all the manikins available to for training are flat-chested. One of us (Rebecca) found it difficult to find any training manikins with breasts.
A single manikin with breasts
Our new research investigated what CPR manikins are available and how diverse they are. We identified 20 CPR manikins on the global market in 2023. Manikins are usually a torso with a head and no arms.
Of the 20 available, five (25%) were sold as “female” – but only one of these had breasts. That means 95% of available CPR training manikins were flat-chested.
We also looked at other features of diversity, including skin tone and larger bodies. We found 65% had more than one skin tone available, but just one was a larger size body. More research is needed on how these aspects affect bystanders in giving CPR.
Breasts don’t change CPR technique
CPR technique doesn’t change when someone has breasts. The barriers are cultural. And while you might feel uncomfortable, starting CPR as soon as possible could save a life.
Signs someone might need CPR include not breathing properly or at all, or not responding to you.
To perform effective CPR, you should:
- put the heel of your hand on the middle of their chest
- put your other hand on the top of the first hand, and interlock fingers (keep your arms straight)
- press down hard, to a depth of about 5cm before releasing
- push the chest at a rate of 100-120 beats per minute (you can sing a song) in your head to help keep time!)
https://www.youtube.com/embed/Plse2FOkV4Q?wmode=transparent&start=94 An example of how to do CPR – with a flat-chested manikin.
What about a defibrillator?
You don’t need to remove someone’s bra to perform CPR. But you may need to if a defibrillator is required.
A defibrillator is a device that applies an electric charge to restore the heartbeat. A bra with an underwire could cause a slight burn to the skin when the debrillator’s pads apply the electric charge. But if you can’t remove the bra, don’t let it delay care.
What should change?
Our research highlights the need for a range of CPR training manikins with breasts, as well as different body sizes.
Training resources need to better prepare people to intervene and perform CPR on people with breasts. We also need greater education about women’s risk of getting and dying from heart-related diseases.
Jessica Stokes-Parish, Assistant Professor in Medicine, Bond University and Rebecca A. Szabo, Honorary Senior Lecturer in Critical Care and Obstetrics, Gynaecology and Newborn Health, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Why the tetanus vaccine matters
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What you need to know
- Tetanus is a serious bacterial infection that attacks the nerves that control muscles, causing painful spasms that can be fatal if untreated.
- The bacteria typically enter the bloodstream through breaks in the skin, such as cuts, bites, burns, and unsanitary injections. Anyone who’s unvaccinated can contract tetanus, but older and immunocompromised people are at highest risk.
- Vaccination is the only way to prevent tetanus. Tetanus vaccines are nearly 100 percent effective and extremely safe, with a very low risk of serious side effects.
What is tetanus?
Tetanus is a painful and potentially deadly infection caused by bacteria living in dirt and soil. When the infection enters the bloodstream, it releases tetanus toxin, which targets the nerves that control your muscles. The bacteria can remain in your body for days or weeks before symptoms appear.
The earliest tetanus symptom is typically lockjaw, characterized by painful spasms in the jaw muscles that make it difficult to speak, swallow, and breathe. Lockjaw can cause severe pain and swelling and may last for days.
After lockjaw sets in, spasms travel down the body, affecting muscles in the neck, chest, abdomen, back, and lower body. Spasms tend to worsen over two weeks and can last for up to a month. In addition to muscle spasms, tetanus may cause fever, heart palpitations, and abnormally high or low blood pressure.
Most people with tetanus are hospitalized, and many require intensive care. Without appropriate treatment, tetanus can turn deadly, as muscle spasms in the neck and chest can impair breathing.
What causes tetanus?
Unlike many infectious diseases, like measles or the flu, tetanus doesn’t spread from person to person. Instead, the infection occurs when bacteria enter your bloodstream, typically through an open wound or unsanitary injection.
Many people believe that stepping on a rusty nail can cause tetanus. But the rust isn’t what poses a risk: it’s the bacteria that live on the nail and other contaminated surfaces. Even a brand-new nail that appears clean can harbor the bacteria that cause tetanus and lead to an infection.
Some common sources of tetanus exposure:
- Cuts or puncture wounds from unsanitized objects, including knives, piercing and sewing needles, and nails.
- Animal and (rarely) insect bites.
- Open wounds or burns contaminated by dirt, feces, or saliva.
- Contaminated needles, including those used in intravenous drug use, piercing, and tattoos.
How can you protect against tetanus?
A tetanus infection does not protect you from future infections, so vaccination is the only way to gain immunity.
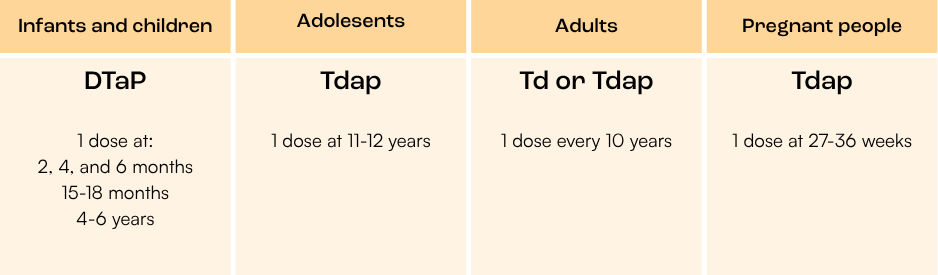
DTaP, which contains full doses of the diphtheria, tetanus, and pertussis vaccines, is for infants and children under 11 years old. All infants and children should receive a total of five doses of DTaP at age 2 months, 4 months, 6 months, 15-18 months, and 4-6 years.
Tdap is a booster that contains a full dose of the tetanus vaccine and low doses of the diphtheria and pertussis vaccines. Adolescents get the booster at age 11 or 12.
The booster is also recommended during pregnancy, after potential tetanus exposure, and every 10 years for adults. Pregnant people should get the Tdap vaccine to protect their baby against both tetanus and whooping cough, which is very dangerous for infants. Non-pregnant adults have the option to receive a Td booster, which does not include a pertussis vaccine.
How effective are tetanus vaccines?
Tetanus vaccines are nearly 100 percent effective. The first modern tetanus vaccines were developed in the 1920s and 1930s. After World War II, the combination vaccine, which also protects against whooping cough (pertussis) and diphtheria, went into widespread use.
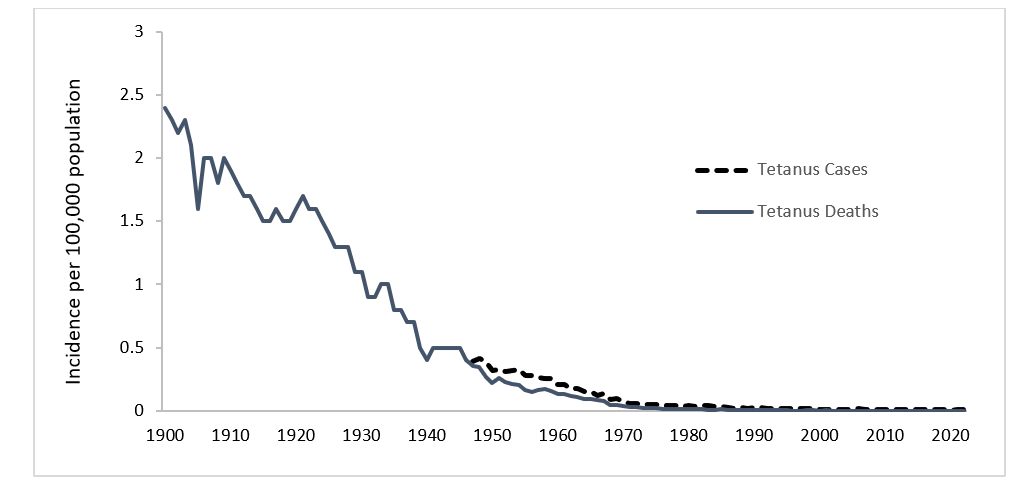
Vaccines, along with improved wound care and the introduction of antibiotics, resulted in a 95 percent reduction in tetanus cases and a 99 percent reduction in tetanus deaths in the U.S. since 1947.
Source: Manual for the Surveillance of Vaccine-Preventable Diseases. Centers for Disease Control and Prevention, 2024. There are currently three tetanus vaccines available in the U.S., depending on your age: DTaP (diphtheria, tetanus, and pertussis), Tdap (tetanus, diphtheria, and pertussis), and Td (tetanus and diphtheria). All three vaccines are nearly 100 percent effective at preventing tetanus.
Tetanus vaccine effectiveness wanes over time, requiring a booster every 10 years. Cases of tetanus in people who are up to date on their vaccinations are extremely rare.
Are tetanus vaccines safe?
Yes, all tetanus vaccines are rigorously tested for safety. There are no safety concerns associated with any tetanus vaccine currently in use. Mild side effects, such as a fever or headache, may occur, but serious side effects are extremely rare.
Like all vaccines, tetanus shots contain ingredients that make them safer and more effective. There are no “toxic” or harmful ingredients in the DTaP, Tdap, or Td vaccines. The full list of ingredients and their purpose has been publicly available for as long as the vaccines have been on the market.
For more information about tetanus vaccination, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: