This Naked Mind – by Annie Grace
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve all read about the many, many, dangers of drinking. We’ve also probably all read about how to make the change to not drinking. Put things out of sight, tell your friends, have this rule, have this excuse (for not drinking) ready to give to people who challenge you, consider a support group, and so on.
What Annie Grace offers in this #1 bestseller is different:
A blend of mostly psychology and sociology, to examine the “liminal thinking” stages that funnel us to drink in the first place… and where that leads, and how to clamber back out of the pitcher plant we weren’t necessarily aware we were sliding into.
While she kicks off citing Jung, from a psychological perspective more of this book is CBTish, as it pertains a lot to examining the process of:
- belief—held and defended, based on the…
- conclusion—drawn, often irrationally, from the…
- experience—that we had upon acting on an…
- observation—often mistaking an illusion for the underlying…
- reality
…and how we can and often do go wrong at each step, and how little of the previous steps we can perceive at any given time.
What does this mean for managing/treating alcoholism or a tendency towards alchoholism?
It means interrupting those processes in a careful, surgically precise fashion, so that suddenly… The thing has no more power over us.
Whether you or a loved one struggle with a tendency to addiction (any addiction, actually, the advice goes the same), or are just curious about the wider factors at hand in the epidemiology of addiction, this book is for you.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Lyme Disease At-A-Glance

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Good info as always…was wondering if you have any recommendations for fighting Lyme disease naturally along wDr advice? Dr’s aren’t real keen on alternatives so always interested. Thanks❞
That depends on whether we’re looking at prevention or cure!
Prevention:
- Try not to get bitten by Lyme-disease-carrying ticks. Boots and long socks are your friends. As are long-gauntletted gloves for gardening.
- If you are in a high-risk area and/or engage in high-risk activities, check your body daily.
- This is because it usually takes 36–48 hours of being attached for a tick to cause an infection
- Obviously best if you can get a partner or close friend to help you with this, unless you have mastered some advanced pretzel positions of yoga.
- Contrary to many folk remedies, the safest way to remove a tick is with tweezers (carefully!).
- If you find and remove a tick, or otherwise suspect you have developed symptoms, go to your doctor immediately (not next week; today; time really counts for this).
Cure:
- No. Sorry. Regretfully, antibiotics are the only known effective treatment.
However! As with almost any kind of recovery, getting good rest, including good quality sleep, will hasten things. Also sensible is reducing stress if possible, and anything that could worsen inflammation.
Share This Post
-

This salt alternative could help reduce blood pressure. So why are so few people using it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One in three Australian adults has high blood pressure (hypertension). Excess salt (sodium) increases the risk of high blood pressure so everyone with hypertension is advised to reduce salt in their diet.
But despite decades of strong recommendations we have failed to get Australians to cut their intake. It’s hard for people to change the way they cook, season their food differently, pick low-salt foods off the supermarket shelves and accept a less salty taste.
Now there is a simple and effective solution: potassium-enriched salt. It can be used just like regular salt and most people don’t notice any important difference in taste.
Switching to potassium-enriched salt is feasible in a way that cutting salt intake is not. Our new research concludes clinical guidelines for hypertension should give patients clear recommendations to switch.
What is potassium-enriched salt?
Potassium-enriched salts replace some of the sodium chloride that makes up regular salt with potassium chloride. They’re also called low-sodium salt, potassium salt, heart salt, mineral salt, or sodium-reduced salt.
Potassium chloride looks the same as sodium chloride and tastes very similar.
Potassium-enriched salt works to lower blood pressure not only because it reduces sodium intake but also because it increases potassium intake. Insufficient potassium, which mostly comes from fruit and vegetables, is another big cause of high blood pressure.
What is the evidence?
We have strong evidence from a randomised trial of 20,995 people that switching to potassium-enriched salt lowers blood pressure and reduces the risks of stroke, heart attacks and early death. The participants had a history of stroke or were 60 years of age or older and had high blood pressure.
An overview of 21 other studies suggests much of the world’s population could benefit from potassium-enriched salt.
The World Health Organisation’s 2023 global report on hypertension highlighted potassium-enriched salt as an “affordable strategy” to reduce blood pressure and prevent cardiovascular events such as strokes.
What should clinical guidelines say?
We teamed up with researchers from the United States, Australia, Japan, South Africa and India to review 32 clinical guidelines for managing high blood pressure across the world. Our findings are published today in the American Heart Association’s journal, Hypertension.
We found current guidelines don’t give clear and consistent advice on using potassium-enriched salt.
While many guidelines recommend increasing dietary potassium intake, and all refer to reducing sodium intake, only two guidelines – the Chinese and European – recommend using potassium-enriched salt.
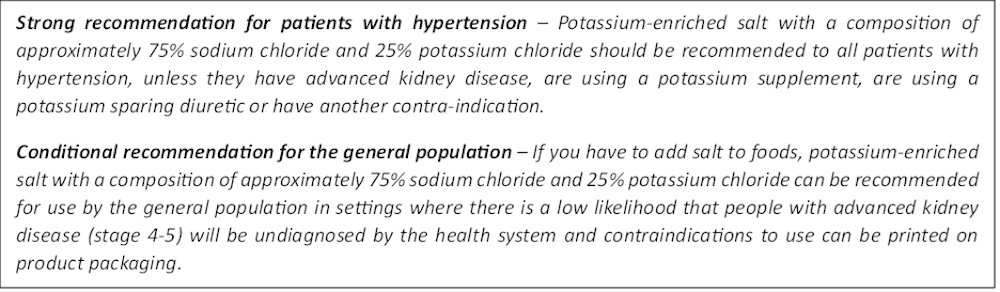
To help guidelines reflect the latest evidence, we suggested specific wording which could be adopted in Australia and around the world:

Recommended wording for guidance about the use of potassium-enriched salt in clinical management guidelines. Why do so few people use it?
Most people are unaware of how much salt they eat or the health issues it can cause. Few people know a simple switch to potassium-enriched salt can help lower blood pressure and reduce the risk of a stroke and heart disease.
Limited availability is another challenge. Several Australian retailers stock potassium-enriched salt but there is usually only one brand available, and it is often on the bottom shelf or in a special food aisle.
Potassium-enriched salts also cost more than regular salt, though it’s still low cost compared to most other foods, and not as expensive as many fancy salts now available.
It looks and tastes like normal salt.
Jimmy Dean/UnsplashA 2021 review found potassium-enriched salts were marketed in only 47 countries and those were mostly high-income countries. Prices ranged from the same as regular salt to almost 15 times greater.
Even though generally more expensive, potassium-enriched salt has the potential to be highly cost effective for disease prevention.
Preventing harm
A frequently raised concern about using potassium-enriched salt is the risk of high blood potassium levels (hyperkalemia) in the approximately 2% of the population with serious kidney disease.
People with serious kidney disease are already advised to avoid regular salt and to avoid foods high in potassium.
No harm from potassium-enriched salt has been recorded in any trial done to date, but all studies were done in a clinical setting with specific guidance for people with kidney disease.
Our current priority is to get people being managed for hypertension to use potassium-enriched salt because health-care providers can advise against its use in people at risk of hyperkalemia.
In some countries, potassium-enriched salt is recommended to the entire community because the potential benefits are so large. A modelling study showed almost half a million strokes and heart attacks would be averted every year in China if the population switched to potassium-enriched salt.
What will happen next?
In 2022, the health minister launched the National Hypertension Taskforce, which aims to improve blood pressure control rates from 32% to 70% by 2030 in Australia.
Potassium-enriched salt can play a key role in achieving this. We are working with the taskforce to update Australian hypertension management guidelines, and to promote the new guidelines to health professionals.
In parallel, we need potassium-enriched salt to be more accessible. We are engaging stakeholders to increase the availability of these products nationwide.
The world has already changed its salt supply once: from regular salt to iodised salt. Iodisation efforts began in the 1920s and took the best part of 100 years to achieve traction. Salt iodisation is a key public health achievement of the last century preventing goitre (a condition where your thyroid gland grows larger) and enhancing educational outcomes for millions of the poorest children in the world, as iodine is essential for normal growth and brain development.
The next switch to iodised and potassium-enriched salt offers at least the same potential for global health gains. But we need to make it happen in a fraction of the time.

Xiaoyue Xu (Luna), Scientia Lecturer, UNSW Sydney; Alta Schutte, SHARP Professor of Cardiovascular Medicine, UNSW Sydney, and Bruce Neal, Executive Director, George Institute Australia, George Institute for Global Health
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Welcoming the Unwelcome – by Pema Chödrön
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There’s a lot in life that we don’t get to choose. Some things we have zero control over, like the weather. Others, we can only influence, like our health. Still yet others might give us an illusion of control, only to snatch it away, like a financial reversal or a bereavement.
How, then, to suffer those “slings and arrows of outrageous fortune” and come through the other side with an even mind and a whole heart?
Author Pema Chödrön has a guidebook for us.
Quick note: this book does not require the reader to have any particular religious faith to enjoy its benefits, but the author is a nun. As such, the way she describes things is generally within the frame of her religion. So that’s a thing to be aware of in case it might bother you. That said…
The largest part of her approach is one that psychology might describe as rational emotive behavioral therapy.
As such, we are encouraged to indeed “meet with triumph and disaster, and treat those two imposters just the same”, and more importantly, she lays out the tools for us to do so.
Does this mean not caring? No! Quite the opposite. It is expected, and even encouraged, that we might care very much. But: this book looks at how to care and remain compassionate, to others and to ourselves.
For Chödrön, welcoming the unwelcome is about de-toothing hardship by accepting it as a part of the complex tapestry of life, rather than something to be endured.
Bottom line: this book can greatly increase the reader’s ability to “go placidly amid the noise and haste” and bring peace to an often hectic world—starting with our own.
Share This Post

Related Posts
-

Kiwi vs Papaya – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kiwi to papaya, we picked the papaya.
Why?
This one was an open-and-shut
casefruit basket:In terms of macros, kiwi has nearly 2x the fiber, slightly more carbs, and (for what it’s worth, which isn’t much because the numbers are small) more than 2x the protein, adding up to a clear win for kiwi in this round—mostly because of the fiber, though.
In the category of vitamins, kiwi has more of vitamins B1, B6, B7, C, E K, and choline, while papaya has more of vitamins A and B9. It’s worth noting that kiwi has (appropriately enough) a lot more vitamin K, while papaya has a lot more of vitamin A (whence the color). In any case, an easy overall win for kiwi on strength of numbers (a clear 7:2 win for kiwi), plus a bonus that we’d prioritize the vitamin K over the vitamin A, as far fewer foods contain vitamin K in high doses (in contrast, so many foods are so high in vitamin A, that it’s almost impossible to be deficient in it unless one is literally starving).
Looking at minerals, kiwi has more calcium, copper, iron, manganese, phosphorus, potassium, and zinc, while papaya has more magnesium and selenium; another clear win for kiwi.
When it comes to specifically phytochemical considerations, kiwi has more polyphenols, and also some anticancer properties that are special to it, while papaya cannot boast any more than any other fruit in this regard.
Adding up the sections makes a complete win for kiwi, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Top 8 Fruits That Prevent & Kill Cancer
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What pathogen might spark the next pandemic? How scientists are preparing for ‘disease X’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Before the COVID pandemic, the World Health Organization (WHO) had made a list of priority infectious diseases. These were felt to pose a threat to international public health, but where research was still needed to improve their surveillance and diagnosis. In 2018, “disease X” was included, which signified that a pathogen previously not on our radar could cause a pandemic.
While it’s one thing to acknowledge the limits to our knowledge of the microbial soup we live in, more recent attention has focused on how we might systematically approach future pandemic risks.
Former US Secretary of Defense Donald Rumsfeld famously talked about “known knowns” (things we know we know), “known unknowns” (things we know we don’t know), and “unknown unknowns” (the things we don’t know we don’t know).
Although this may have been controversial in its original context of weapons of mass destruction, it provides a way to think about how we might approach future pandemic threats.
Anna Shvets/Pexels Influenza: a ‘known known’
Influenza is largely a known entity; we essentially have a minor pandemic every winter with small changes in the virus each year. But more major changes can also occur, resulting in spread through populations with little pre-existing immunity. We saw this most recently in 2009 with the swine flu pandemic.
However, there’s a lot we don’t understand about what drives influenza mutations, how these interact with population-level immunity, and how best to make predictions about transmission, severity and impact each year.
The current H5N1 subtype of avian influenza (“bird flu”) has spread widely around the world. It has led to the deaths of many millions of birds and spread to several mammalian species including cows in the United States and marine mammals in South America.
Human cases have been reported in people who have had close contact with infected animals, but fortunately there’s currently no sustained spread between people.
While detecting influenza in animals is a huge task in a large country such as Australia, there are systems in place to detect and respond to bird flu in wildlife and production animals.
Scientists are continually monitoring a range of pathogens with pandemic potential. Edward Jenner/Pexels It’s inevitable there will be more influenza pandemics in the future. But it isn’t always the one we are worried about.
Attention had been focused on avian influenza since 1997, when an outbreak in birds in Hong Kong caused severe disease in humans. But the subsequent pandemic in 2009 originated in pigs in central Mexico.
Coronaviruses: an ‘unknown known’
Although Rumsfeld didn’t talk about “unknown knowns”, coronaviruses would be appropriate for this category. We knew more about coronaviruses than most people might have thought before the COVID pandemic.
We’d had experience with severe acute respiratory syndrome (SARS) and Middle Eastern respiratory syndrome (MERS) causing large outbreaks. Both are caused by viruses closely related to SARS-CoV-2, the coronavirus that causes COVID. While these might have faded from public consciousness before COVID, coronaviruses were listed in the 2015 WHO list of diseases with pandemic potential.
Previous research into the earlier coronaviruses proved vital in allowing COVID vaccines to be developed rapidly. For example, the Oxford group’s initial work on a MERS vaccine was key to the development of AstraZeneca’s COVID vaccine.
Similarly, previous research into the structure of the spike protein – a protein on the surface of coronaviruses that allows it to attach to our cells – was helpful in developing mRNA vaccines for COVID.
It would seem likely there will be further coronavirus pandemics in the future. And even if they don’t occur at the scale of COVID, the impacts can be significant. For example, when MERS spread to South Korea in 2015, it only caused 186 cases over two months, but the cost of controlling it was estimated at US$8 billion (A$11.6 billion).
COVID could be regarded as an ‘unknown known’. Markus Spiske/Pexels The 25 viral families: an approach to ‘known unknowns’
Attention has now turned to the known unknowns. There are about 120 viruses from 25 families that are known to cause human disease. Members of each viral family share common properties and our immune systems respond to them in similar ways.
An example is the flavivirus family, of which the best-known members are yellow fever virus and dengue fever virus. This family also includes several other important viruses, such as Zika virus (which can cause birth defects when pregnant women are infected) and West Nile virus (which causes encephalitis, or inflammation of the brain).
The WHO’s blueprint for epidemics aims to consider threats from different classes of viruses and bacteria. It looks at individual pathogens as examples from each category to expand our understanding systematically.
The US National Institute of Allergy and Infectious Diseases has taken this a step further, preparing vaccines and therapies for a list of prototype pathogens from key virus families. The goal is to be able to adapt this knowledge to new vaccines and treatments if a pandemic were to arise from a closely related virus.
Pathogen X, the ‘unknown unknown’
There are also the unknown unknowns, or “disease X” – an unknown pathogen with the potential to trigger a severe global epidemic. To prepare for this, we need to adopt new forms of surveillance specifically looking at where new pathogens could emerge.
In recent years, there’s been an increasing recognition that we need to take a broader view of health beyond only thinking about human health, but also animals and the environment. This concept is known as “One Health” and considers issues such as climate change, intensive agricultural practices, trade in exotic animals, increased human encroachment into wildlife habitats, changing international travel, and urbanisation.
This has implications not only for where to look for new infectious diseases, but also how we can reduce the risk of “spillover” from animals to humans. This might include targeted testing of animals and people who work closely with animals. Currently, testing is mainly directed towards known viruses, but new technologies can look for as yet unknown viruses in patients with symptoms consistent with new infections.
We live in a vast world of potential microbiological threats. While influenza and coronaviruses have a track record of causing past pandemics, a longer list of new pathogens could still cause outbreaks with significant consequences.
Continued surveillance for new pathogens, improving our understanding of important virus families, and developing policies to reduce the risk of spillover will all be important for reducing the risk of future pandemics.
This article is part of a series on the next pandemic.
Allen Cheng, Professor of Infectious Diseases, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How Vitamin D May Help Protect Against Diabetes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
…and other items from this week’s health science news:
D vs D
Vitamin D may help protect you from diabetes… Or it may not. The science is clear on this!
In other words: the data (with a large amount of data analysis and a RCT with 2,098 people with prediabetes) is clear about the effect in general, and what that science says, is that whether or not it helps you as an individual, will depend on your genes.
Specifically:
- Participants with the AA variation of the vitamin D receptor gene showed no meaningful response when taking 4,000 IU of vitamin D daily compared with a placebo.
- Participants with AC or CC in the the vitamin D receptor gene had a 19% lower risk of developing diabetes when taking 4,000 IU of vitamin D daily compared with a placebo.
Why the genetic variation matters: vitamin D must bind to the vitamin D receptor to work in your body, and differences in this receptor—particularly in insulin-producing cells in your pancreas—will affect how well vitamin D helps regulate blood sugar.
So, this one’s a case for personalized prevention, where a simple genetic test could identify who is likely to benefit from higher vitamin D intake.
Read in full: Vitamin D may help prevent diabetes
Related: The Real Benefit Of Genetic Testing
Relighting the brain’s fire for happiness
Researchers (Dr. Alice Meuret et al.) have found that a therapy that directly targets lost pleasure (anhedonia*) improves depression and anxiety more than standard treatments that mainly reduce negative emotions.
*It’s not just about pleasure in the sense most might speak of such, though; anhedonia is the reduced or absent ability to feel positive emotions in general. It affects nearly all people with depression, and is strongly linked to worse outcomes, relapse, and suicidal risk.
The problem with standard therapies: most treatments focus on reducing sadness, fear, or distress, but largely ignore rebuilding positive emotions—even though patients often see that as their main goal.
Positive Affect Treatment (PAT), in contrast, is a 15-session psychotherapy designed to restore joy, motivation, meaning, and reward sensitivity. Specifically, it targets the brain’s reward system by encouraging engagement in meaningful activities, shifting attention towards positive experiences, and practising gratitude, savoring, and compassion-based exercises.
As for how well it works: the RCT of 98 adults with severe anhedonia, depression, and anxiety compared PAT to a conventional therapy focused on negative emotions. The results? PAT produced greater overall clinical improvement, including reductions in both depression and anxiety, even though it never directly targeted negative emotions.
Read in full: Targeting lost pleasure lifts depression and anxiety more than standard therapy, new study finds
Related: Behavioral Activation Against Depression & Anxiety
Allergy season feeling different this year?
Due to climate change, pollen seasons are starting earlier, lasting longer, and even overlapping. because of warmer temperatures and higher CO₂, which keeps your immune system in overdrive for longer and leads to more intense symptoms.
Air pollution (which is getting steadily worse in the US and likely many other places too) can also alter pollen particles, making them more irritating to your airways and increasing inflammation.
Children’s symptoms are easy to miss: kids may show allergies through mouth breathing, fatigue, irritability, sleep issues, ear infections, or dark circles under your eyes rather than clearly describing symptoms.
A very common mistake (regardless of age), is starting treatment too late, and/or using medication only when symptoms become onerous, but by this time, your immune system has already been overworked, and taking anti-allergy meds now won’t mean the already-in-progress war in your body suddenly stops instantly.
So instead, you might consider starting allergy medication before symptoms peak, and then taking it consistently for a few weeks (even if the symptoms stop, because that is what the meds are for!), to prevent your immune response from ramping up.
Read in full: Are you managing your allergies the wrong way?
Related: Antihistamines’ Generation Gap
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: