Cashews vs Walnuts – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cashews to walnuts, we picked the walnuts.
Why?
Both are great! But a winner did emerge:
In terms of macros, cashews have slightly more protein, while walnuts have about 2x the fiber. As for fats, walnuts have more fat. Looking further into it: cashews’ fats are mostly monounsaturated, while walnuts’ fats are mostly polyunsaturated, both of which are considered healthy. All in all, we consider this a win for walnuts on account of the noteworthy fiber difference, but both are great.
It’s worth mentioning that notwithstanding being both high in calories, neither nut is associated with weight gain—largely because of their low glycemic indices (of which, walnuts have the slightly lower GI, but both are low-GI foods).
In the category of vitamins, cashews have more of vitamins B1, B5, E, and K, while walnuts have more of vitamins A, B2, B3 B6, B9, and C, giving walnuts the victory here.
Looking at minerals, cashews get their day, as cashews have more copper, iron, magnesium, phosphorus, potassium, selenium, and zinc, while walnuts have more calcium and manganese, meaning that cashews score a point finally.
In other considerations, walnuts are much higher in polyphenols, of which, especially flavonoids, of which especially flavonols, of which especially epicatechins. So, this round gives an extra point for walnuts.
Adding up the sections makes for a clear overall win for walnuts, but (unless you have a nut allergy, of course) do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
- Are You Getting The Right Kinds Of Flavonoids?
- Enjoy Bitter Foods For Your Heart & Brain
- Why You Should Diversify Your Nuts
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fig vs Mango – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing figs to mangos, we picked the figs.
Why?
In terms of macros, figs have 2x the fiber and only slightly more carbs, for the lower glycemic index, and a win in this category.
In the category of vitamins, figs have more of vitamins B1, B2, B5, B6, B7, and K, while mango has more of vitamins A, B2, B9, C, E, and choline, for a 6:6 tie.
Looking at minerals, figs have more calcium, iron, magnesium, manganese, phosphorus, potassium, and zinc, while mangos have more copper and selenium; a clear a win for figs.
When it comes to other considerations, it’s worth noting also that figs are higher in polyphenols, another point in their favor.
Adding up the sections makes for a clear overall win for figs, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
Enjoy!
Share This Post
-

When Doctors Make House Calls, Modern-Style!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

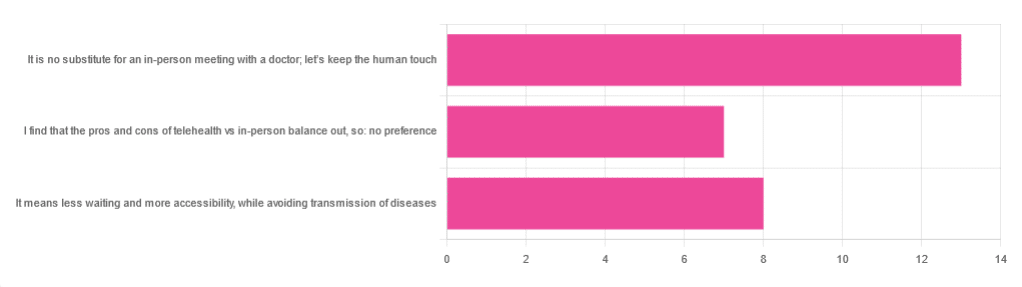
In Tuesday’s newsletter, we asked you foryour opinion of telehealth for primary care consultations*, and got the above-depicted, below-described, set of responses:
- About 46% said “It is no substitute for an in-person meeting with a doctor; let’s keep the human touch”
- About 29% said “It means less waiting and more accessibility, while avoiding transmission of diseases”
- And 25 % said “I find that the pros and cons of telehealth vs in-person balance out, so: no preference”
*We specified that by “primary care” we mean the initial consultation with a non-specialist doctor, before receiving treatment or being referred to a specialist. By “telehealth” we mean by videocall or phonecall.
So, what does the science say?
A quick note first
Because telehealth was barely a thing (statistically speaking) before the first stages of the COVID pandemic, compared to how it is now, most of the science for this is young, and a lot of the science simply hasn’t been done yet, and/or has not been published yet, because the process can take years.
Because of this, some studies we do have aren’t specifically about primary care, and are sometimes about specialists. We think this should not affect the results much, but it bears highlighting.
Nevertheless, we’ll do what we can with the science we have!
Telehealth is more accessible than in-person consultations: True or False?
True, for most people. For example…
❝Data was found from a variety of emergency and non-emergency departments of primary, secondary, and specialised healthcare.
Satisfaction was high among recipients of healthcare, scoring 9-10 on a scale of 0-10 or ranging from 73.3% to 100%.
Convenience was rated high in every specialty examined. Satisfaction of clinicians was high throughout the specialities despite connection failure and concerns about confidentiality of information.❞
whereas…
❝Nonetheless, studies reported perception of increased barriers to accessing care and inequalities for vulnerable patients especially in older people❞
~ Ibid.
Source: Satisfaction with telemedicine use during COVID-19 pandemic in the UK: a systematic review
Now, perception of those things does necessarily equate to an actual increased barrier, but it is reasonable that someone who thinks something is inaccessible will be less inclined to try to access it.
The quality of care provided via telehealth is as good as in-person: True or False?
True, ostensibly, with caveats. The caveats are:
- We’re going offreported patient satisfaction, not objective patient health outcomes (we found little* science as yet for the relative incidence of misdiagnosis, for example—which kind of thing will take time to be revealed).
- We’re also therefore speaking (as statistics do) for the significant majority of people. However, if we happen to be (statistically speaking) an insignificant minority, well, that just sucks for us personally.
*we did find some, but it wasn’t very helpful yet. For example:
An electronic trigger to detect telemedicine-related diagnostic errors
this one does look at the incidence of diagnostic errors, but provides no control group (i.e. otherwise-comparable in-person consultations) for comparison.
While most oft-considered demographic groups reported comparable patient satisfaction (per race, gender, and socioeconomic status, for example), there was one outlier variable, which was age (as we quoted from that first study above).
However!
Looking under the hood of these stats, it seems that age is not the real culprit, so much as technological illiteracy, which is heavily correlated with age:
❝Lower eHealth literacy is associated with more negative attitudes towards I/C technology in healthcare. This trend is consistent across diverse demographics and regions. ❞
Source: Meta-analysis: eHealth literacy and attitudes towards internet/computer technology
There are things that can be done at an in-person consultation that can’t be done by telehealth: True or False?
True, of course. It is incredibly rare that we will cite “common sense”, (as sometimes “common sense” is actually “common mistakes” and is simply and verifiably wrong), but in this case, as one 10almonds subscriber put it:
❝The doctor uses his five senses to assess. This cannot be attained over the phone❞
~ 10almonds subscriber
A quick note first: if your doctor is using their sense of taste to diagnose you, please get a different doctor, because they should definitely not be doing that!
Not in this century, anyway… Once upon a time, diabetes was diagnosed by urine-tasting (and yes, that was a fairly reliable method).
However, nowadays indeed a doctor will use sight, sound, touch, and sometimes even smell.
In a videocall we’re down to two of those senses (sight and sound), and in a phonecall, down to one (sound) and even that is hampered. Your doctor cannot, for example, use a stethoscope over the phone.
With this in mind, it really comes down to what you need from your doctor in that consultation.
- If you’re 99% sure that what you need is to be prescribed an antidepressant, that probably doesn’t need a full physical.
- If you’re 99% sure that what you need is a referral, chances are that’ll be fine by telehealth too.
- If your doctor is 99% sure that what you need is a verbal check-up (e.g. “How’s it been going for you, with the medication that I prescribed for you a month ago?”, then again, a call is probably fine.
If you have a worrying lump, or an unhappy bodily discharge, or an unexplained mysterious pain? These things, more likely an in-person check-up is in order.
Take care!
Share This Post
-

Anticancer: A New Way Of Life – by Dr. David Servan-Schreiber
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A cancer survivor himself, Dr. Servan-Schreiber found himself unimpressed with the advice he was given upon diagnosis, and set out to find better. This, he achieved.
He first provides an introductory overview of cancer, and then devotes most of the book to detailing how to create a “terrain” (the environment of your body and all that you do with/to it) that is hostile to cancer.
This includes things like diet, of course, but also exercise (the right way!), mindset, and much more. He doesn’t cover much about standard medical treatments, as he assumes the reader will already be advised about those by their oncologist, and in any case, such treatments are constantly changing as new discoveries are made. It’s worth mentioning that while he advocates strongly for complementary medicine, he does also make clear it should be just that—complementary—and not a replacement for regular treatments in cases where such are recommended.
The style is comprehensible pop-science, written for the lay reader, and yet with copious scientific references—more than 30 pages thereof. But as well as that, it’s a personal account, often revisiting his own cancer journey to illustrate one point or another, be it something that went well for him or badly, there’s always something to learn.
Bottom line: this book is important for anyone facing cancer, and useful for anyone who simply would like to improve their odds in a more informed fashion. As he notes, “all of us have cancer cells in our bodies, but not all of us will develop cancer”, and it’s good to try to be on the healthiest side of that.
Click here to check out Anticancer, and live an anticancer life!
Share This Post


Related Posts
-

Older, Faster, Stronger – by Margaret Webb
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author, now in her 60s, made it her mission in her 50s to become the best runner she could. Before that, she’d been a keen runner previously, but let things slip rather in her 40s. But the book’s not about her 40s, it’s about her 50s and onwards, and other female runners in their 50s, 60s, 70s, 80s, and even 90s.
There’s a lot of this book that’s about people’s individual stories, and those should certainly be enough to prompt almost any reader that “if they can do it, I can”.
A lot, meanwhile, is about health and exercise science, training methods, and what has worked for various later-life athletes, including the author. So, it’s also partway instruction manual, with plenty of reference to science and medical considerations too.
Bottom line: sometimes, life throws us challenges. Sometimes, the best response is “Yeah? Bet” and surprise everyone.
Click here to check out Older, Faster, Stronger, and become all those cool things!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Life Is in the Transitions – by Bruce Feiler
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Change happens. Sometimes, because we choose it. More often, we don’t get a choice.
Our bodies change; with time, with illness, with accident or incident, or even, sometimes, with effort. People in our lives change; they come, they go, they get sick, they die. Our working lives change; we get a job, we lose a job, we change jobs, our jobs change, we retire.
Whether we’re undergoing cancer treatment or a religious conversion, whether our families are growing or down to the last few standing, change is inescapable.
Our author makes the case that on average, we each undergo at least 5 major “lifequakes”; changes that shake our lives to the core. Sometimes one will come along when we’ve barely got back on our feet from the previous—if we have at all.
What, then, to do about this? We can’t stop change from occurring, and some changes aren’t easy to “roll with”. Feiler isn’t prescriptive about this, but rather, descriptive:
By looking at the stories of hundreds of people he interviewed for this book, he looks at how people pivoted on the spot (or picked up the pieces!) and made the best of their situation—or didn’t.
Bottom line: zooming out like this, looking at many people’s lives, can remind us that while we don’t get to choose what winds we get swept by, we at least get to choose how we set the sails. The examples of others, as this book gives, can help us make better decisions.
Click here to check out Life Is In The Transitions, and get conscious about how you handle yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How pregnant women are tested for gestational diabetes is changing. Here’s what this means for you
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How Australian pregnant women are tested for gestational diabetes is set to change, with new national guidelines released today.
Changes are expected to lead to fewer diagnoses in women at lower risk, reducing the burden of extra monitoring and intervention. Meanwhile the changes focus care and support towards women and babies who will benefit most.
These latest recommendations form the first update in screening for gestational diabetes in more than a decade, and potentially affect more than 280,000 pregnant women a year across Australia.
The new guidelines, which we have been involved in writing, are released today by the Australasian Diabetes in Pregnancy Society and published in the Medical Journal of Australia.
What is gestational diabetes? Why do we test for it?
Gestational diabetes (also known as gestational diabetes mellitus) is one of the most common medical complications of pregnancy. It affects nearly one in five pregnancies in Australia.
It is defined by abnormally high levels of glucose (sugar) in the blood that are first picked up during pregnancy.
Most of the time gestational diabetes goes away after the birth. But women with gestational diabetes are at least seven times more likely to develop type 2 diabetes later in life.
In Australia, routine screening for gestational diabetes is recommended for all pregnant women. This will continue.
That’s because treatment reduces the risk of poorer pregnancy outcomes. This includes babies being born very large – a condition called macrosomia – which can lead to difficult births, and a caesarean. Treatment also reduces the risk of pre-eclampsia, when women have high blood pressure and protein in their urine, and other serious pregnancy complications.
Screening for gestational diabetes is also an opportunity to identify women who may benefit from diabetes prevention programs and ways to support their long-term health, including support with nutrition and physical activity.
Why is testing changing?
Most women benefit from detection and treatment. However, for some women, a diagnosis can have negative impacts. This often relates to how care is delivered.
Women have described feeling shame and stigma after the diagnosis. Others report challenges accessing the care and support they need during pregnancy. This may include access to specialist doctors, allied health professionals and clinics. Some women have restricted their diet in an unhealthy way, without appropriate supervision by a health professional. Some have had to change their preferred maternity care provider or location of birth because their pregnancy is now considered higher risk.
So we must diagnose the condition in women when the benefits outweigh the potential costs.

Which pregnant women need a blood test and when? And when are other types of testing warranted? Elizaveta Galitckaia/Shutterstock When are blood sugar levels too high?
Diagnosing gestational diabetes is based on having blood glucose levels above a certain threshold.
However, there is no clear level above which the risk of complications starts to increase. And determining the best thresholds to identify who does, and who does not, have gestational diabetes has been subject to much research and debate.
Globally, screening approaches and diagnostic criteria vary substantially. There are differences in who is recommended to be screened, when in pregnancy screening should occur, which tests should be used, and what the diagnostic glucose levels should be.
So, what changes?
The new recommendations are the result of reviewing up-to-date evidence with input from a wide range of professional and consumer groups.
Screening will continue
All pregnant women who don’t already have a diagnosis of pre-pregnancy diabetes, or gestational diabetes, will still be recommended screening at between 24 and 28 weeks’ gestation. They’ll still have an oral glucose tolerance test, a measure of how the body processes sugar. The test involves fasting overnight, and having a blood test in the morning before drinking a sugary drink. Then there are two more blood tests over two hours. However, fewer women will have this test twice in their pregnancy.
Changes mean more targeted care
The following changes mean health services should be able to reorient resources to ensure women have access to the care they need to support healthier pregnancies, including early support for women who need it most:
- women with risk factors of existing, undiagnosed diabetes (such as a higher body-mass index or BMI, or a previous large baby) will be screened in the first trimester, with a single, non-fasting blood test (known as HbA1c)
- fewer women will have an oral glucose tolerance test early in the pregnancy, ideally between ten and 14 weeks gestation. This early testing will be reserved for women with specific risk factors, such as gestational diabetes in a previous pregnancy, or a high level on the HbA1c test
- women will only be diagnosed if their blood glucose level is above new, higher cut-off points for the oral glucose tolerance test, for tests conducted early or later in the pregnancy.
Which tests do I need?
These changes will be implemented over coming months. So women are encouraged to speak to their maternity care provider about how the changes apply to them.
Alexis Shub, Obstetrician & Maternal Fetal Medicine specialist, The University of Melbourne; Matthew Hare, Senior Research Fellow & Endocrinologist, Menzies School of Health Research, and Susan de Jersey, Associate Professor, Advanced Dietitian and Credentialled Diabetes Educator., The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: