Should You Go Light Or Heavy On Carbs?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Carb-Strong or Carb-Wrong?
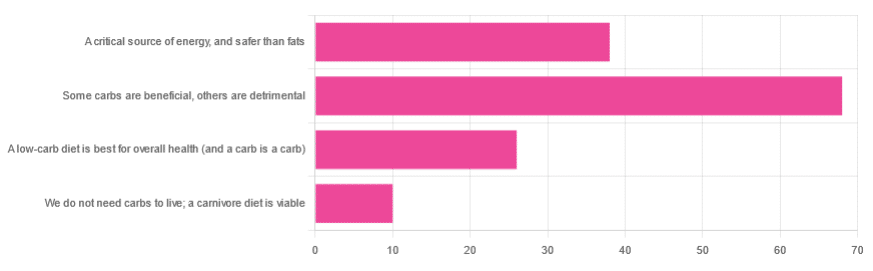
We asked you for your health-related view of carbs, and got the above-depicted, below-described, set of responses
- About 48% said “Some carbs are beneficial; others are detrimental”
- About 27% said “Carbs are a critical source of energy, and safer than fats”
- About 18% said “A low-carb diet is best for overall health (and a carb is a carb)”
- About 7% said “We do not need carbs to live; a carnivore diet is viable”
But what does the science say?
Carbs are a critical source of energy, and safer than fats: True or False?
True and False, respectively! That is: they are a critical source of energy, and carbs and fats both have an important place in our diet.
❝Diets that focus too heavily on a single macronutrient, whether extreme protein, carbohydrate, or fat intake, may adversely impact health.❞
Source: Low carb or high carb? Everything in moderation … until further notice
(the aforementioned lead author Dr. de Souza, by the way, served as an external advisor to the World Health Organization’s Nutrition Guidelines Advisory Committee)
Some carbs are beneficial; others are detrimental: True or False?
True! Glycemic index is important here. There’s a big difference between eating a raw carrot and drinking high-fructose corn syrup:
Which Sugars Are Healthier, And Which Are Just The Same?
While some say grains and/or starchy vegetables are bad, best current science recommends:
- Eat some whole grains regularly, but they should not be the main bulk of your meal (non-wheat grains are generally better)
- Starchy vegetables are not a critical food group, but in moderation they are fine.
To this end, the Mediterranean Diet is the current gold standard of healthful eating, per general scientific consensus:
A low-carb diet is best for overall health (and a carb is a carb): True or False?
True-ish and False, respectively. We covered the “a carb is a carb” falsehood earlier, so we’ll look at “a low-carb diet is best”.
Simply put: it can be. One of the biggest problems facing the low-carb diet though is that adherence tends to be poor—that is to say, people crave their carby comfort foods and eat more carbs again. As for the efficacy of a low-carb diet in the context of goals such as weight loss and glycemic control, the evidence is mixed:
❝There is probably little to no difference in weight reduction and changes in cardiovascular risk factors up to two years’ follow-up, when overweight and obese participants without and with T2DM are randomised to either low-carbohydrate or balanced-carbohydrate weight-reducing diets❞
Source: Low-carbohydrate versus balanced-carbohydrate diets for reducing weight and cardiovascular risk
❝On the basis of moderate to low certainty evidence, patients adhering to an LCD for six months may experience remission of diabetes without adverse consequences.
Limitations include continued debate around what constitutes remission of diabetes, as well as the efficacy, safety, and dietary satisfaction of longer term LCDs❞
~ Dr. Joshua Goldenberg et al.
Source: Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission
❝There should be no “one-size-fits-all” eating pattern for different patient´s profiles with diabetes.
It is clinically complex to suggest an ideal percentage of calories from carbohydrates, protein and lipids recommended for all patients with diabetes.❞
Source: Current Evidence Regarding Low-carb Diets for The Metabolic Control of Type-2 Diabetes
We do not need carbs to live; a carnivore diet is viable: True or False?
False. For a simple explanation:
The Carnivore Diet: Can You Have Too Much Meat?
There isn’t a lot of science studying the effects of consuming no plant products, largely because such a study, if anything other than observational population studies, would be unethical. Observational population studies, meanwhile, are not practical because there are so few people who try this, and those who do, do not persist after their first few hospitalizations.
Putting aside the “Carnivore Diet” as a dangerous unscientific fad, if you are inclined to meat-eating, there is some merit to the Paleo Diet, at least for short-term weight loss even if not necessarily long-term health:
What’s The Real Deal With The Paleo Diet?
For longer-term health, we refer you back up to the aforementioned Mediterranean Diet.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Huperzine A: A Natural Nootropic

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Huperzine A: A Natural Nootropic
Huperzine A is a compound, specifically a naturally occurring sesquiterpene alkaloid, that functions as an acetylcholinesterase inhibitor. If that seems like a bunch of big words, don’t worry, we’ll translate in a moment.
First, a nod to its origins: it is found in certain kinds of firmoss, especially the “toothed clubmoss”, Huperzia serrata, which grows in many Asian countries.
What’s an acetylcholinesterase inhibitor?
Let’s do this step-by-step:
- An acetylcholinesterase inhibitor is a compound that inhibits acetylcholinesterase.
- Acetylcholinesterase is an enzyme that catalyzes (speeds up) the breakdown of acetylcholine.
- Acetylcholine is a neurotransmitter; it’s an ester of acetic acid and choline.
- This is the main neurotransmitter of the parasympathetic nervous system, and is also heavily involved in cognitive functions including memory and creative thinking.
What this means: if you take an acetylcholinesterase inhibitor like huperzine A, it will inhibit acetylcholinesterase, meaning you will have more acetylcholine to work with. That’s good.
What can I expect from it?
Huperzine A has been well-studied for a while, mostly for the prevention and treatment of Alzheimer’s disease:
- New insights into huperzine A for the treatment of Alzheimer’s disease
- Huperzine A: Is it an Effective Disease-Modifying Drug for Alzheimer’s Disease?
- Huperzine A and Its Neuroprotective Molecular Signaling in Alzheimer’s Disease
However, research has suggested that huperzine A is much better as a prevention than a treatment:
❝A central event in the pathogenesis of Alzheimer’s disease (AD) is the accumulation of senile plaques composed of aggregated amyloid-β (Aβ) peptides.
Ex vivo electrophysiological experiments showed that 10 μM of Aβ1-40 significantly decreased the effect of the AChE inhibitor huperzine A on the synaptic potential parameters. ❞
~ Dr. Irina Zueva
In other words: the answer to the titular question is “Yes, yes it can”
And, to translate Dr. Zueva’s words into simple English:
- People with Alzheimer’s have amyloid-β plaque in their brains
- That plaque reduces the effectiveness of huperzine A
So, what if we take it in advance? That works much better:
❝Pre-treatment with [huperzine A] at concentrations of 50, 100, and 150 µg/mL completely inhibited the secretion of PGE2, TNF-α, IL-6, and IL-1β compared to post-treatment with [huperzine A].
This suggests that prophylactic treatment is better than post-inflammation treatment. ❞
~ Dr. Thu Kim Dang
Source: Anti-neuroinflammatory effects of alkaloid-enriched extract from Huperzia serrata
As you may know, neuroinflammation is a big part of Alzheimer’s pathology, so we want to keep that down. The above research suggests we should do that sooner rather than later.
Aside from holding off dementia, can it improve memory now, too?
There’s been a lot less research done into this (medicine is generally more concerned with preventing/treating disease, than improving the health of healthy people), but there is some:
^This is a small (n=68) old (1999) study for which the full paper has mysteriously disappeared and we only get to see the abstract. It gave favorable results, though.
The effects of huperzine A and IDRA 21 on visual recognition memory in young macaques
^This, like most non-dementia research into HupA, is an animal study. But we chose to spotlight this one because, unlike most of the studies, it did not chemically lobotomize the animals first; they were and remained healthy. That said, huperzine A improved the memory scores most for the monkeys that performed worst without it initially.
Where can I get it?
As ever, we don’t sell it, but here’s an example product on Amazon for your convenience
Enjoy!
Share This Post
-

Physical Sunscreen or Chemical Sunscreen – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing physical sunscreens to chemical sunscreens, we picked the physical sunscreens.
Why?
It’s easy to vote against chemical sunscreens, because it has “chemical” in the name, which tends to be offputting PR-wise no matter how healthy something is.
But in this case, there’s actual science here too!
Physical sunscreens physically block the UV rays.
- On the simplest of levels, mud is a physical sunscreen, as you can see widely used by elephants, hippos, pigs, and other animals.
- On a more sophisticated level, modern physical sunscreens often use tiny zinc particles (or similar) to block the UV rays in a way that isn’t so obvious to the naked eye—so we can still see our skin, and it looks just like we applied an oil or other moisturizer.
Chemical sunscreens interact with the UV rays in a way that absorbs them.
- Specifically, they usually convert it into relatively harmless thermal energy (heat)
- However, this can cause problems if there’s too much heat!
- Additionally, chemical sunscreens can get “used up” in a way that physical sunscreens can’t* becoming effectively deactivated once the chemical reaction has run its course and there is no more reagent left unreacted.
- Worse, some of the reagents, when broken down by the UV rays, can potentially cause harm when absorbed by the skin.
*That said, physical sunscreens will still need “topping up” because we are a living organism and our body can’t resist redistributing and using stuff—plus, depending on the climate and our activities, we can lose some externally too.
Further reading
We wrote about sunscreens (of various kinds) here:
And you can also read specifically about today’s topic in more detail, here:
What’s The Difference Between Physical And Chemical Sunscreens?
Take care!
Share This Post
-

Train For The Event Of Your Life!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Mobility As A Sporting Pursuit
As we get older, it becomes increasingly important to treat life like a sporting event. By this we mean:
As an “athlete of life”, there are always events coming up for which we need to train. Many of these events will be surprise tests!
Such events/tests might include:
- Not slipping in the shower and breaking a hip (or worse)
- Reaching an item from a high shelf without tearing a ligament
- Getting out of the car at an awkward angle without popping a vertebra
- Climbing stairs without passing out light-headed at the top
- Descending stairs without making it a sled-ride-without-a-sled
…and many more.
Train for these athletic events now
Not necessarily this very second; we appreciate you finishing reading first. But, now generally in your life, not after the first time you fail such a test; it can (and if we’re not attentive: will) indeed happen to us all.
With regard to falling, you might like to revisit our…
…which covers how to not fall, and to not injure yourself if you do.
You’ll also want to be able to keep control of your legs (without them buckling) all the way between standing and being on the ground.
Slav squats or sitting squats (same exercise, different names, amongst others) are great for building and maintaining this kind of strength and suppleness:
(Click here for a refresher if you haven’t recently seen Zuzka’s excellent video explaining how to do this, especially if it’s initially difficult for you, “The Most Anti-Aging Exercise”)
this exercise is, by the way, great for pretty much everything below the waist!
You will also want to do resistance exercises to keep your body robust:
Resistance Is Useful! (Especially As We Get Older)
And as for those shoulders? If it is convenient for you to go swimming, then backstroke is awesome for increasing and maintaining shoulder mobility (and strength).
If swimming isn’t a viable option for you, then doing the same motion with your arms, while standing, will build the same flexibility. If you do it while holding a small weight (even just 1kg is fine, but feel free to increase if you so wish and safely can) in each hand will build the necessary strength as you go too.
As for why even just 1kg is fine: read on
About that “and strength”, by the way…
Stretching is not everything. Stretching is great, but mobility without strength (in that joint!) is just asking for dislocation.
You don’t have to be built like the Terminator, but you do need to have the structural integrity to move your body and then a little bit more weight than that (or else any extra physical work could be enough to tip you to breaking point) without incurring damage from the strain. So, it needs to not be a strain! See again, the aforementioned resistance exercises.
That said, even very gentle exercise helps too; see for example the impact of walking on osteoporosis:
Living near green spaces linked to higher bone density and lower osteoporosis risk
and…
So you don’t have to run marathons—although you can if you want:
Marathons in Mid- and Later-Life
…to keep your hips and more in good order.
Want to test yourself now?
Check out:
Building & Maintaining Mobility
Take care!
Share This Post

Related Posts
-

Chocolate & Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Chocolate & Health: Fact or Fiction?
“Chocolate Is Good For The Heart”
“When making chocolate chip cookies, you don’t measure using cups, you measure by heart”
…but how good is chocolate when it comes to heart health?
First, what is heart health?
A healthy heart typically has a low resting pulse rate and a strong, steady beat. This is affected strongly by exercise habits, and diet plays only a support role (can’t exercise without energy from food!).
It is also important to have blood pressure within a healthy range (with high blood pressure being a more common problem than low, so things that lower blood pressure are generally considered good).
- Flavanols, flavonoids, and polyphenols in chocolate contribute to lower blood pressure
- Dark chocolate is best for these, as milk chocolate contains much less cocoa solids and more unhelpful fats
- White chocolate contains no cocoa solids and is useless for this
- Some of the fats in most commercial chocolate can contribute to atherosclerosis which raises blood pressure and ultimately can cause heart attacks.
- If you’re diabetic, you will probably not get the usual heart-related benefits from chocolate (sorry)
The Verdict: dark chocolate, in moderation, can support good heart health.
“Chocolate Is Good For The Brain”
Chocolate has been considered a “brain food”… why?
- The brain uses more calories than any other organ (chocolate has many calories)
- The heart benefits we listed above mean improved blood flow—including to your brain
- Chocolate contains phenylethylamine, a powerful chemical that has a similar effect to amphetamines… But it’s metabolized in digestion and never makes it to the central nervous system (so basically, this one’s a miss; we had a good run with the other two, though!)
The Verdict: dark chocolate, in moderation, can support good brain health
“Chocolate Is An Aphrodisiac”
“If chocolate be the food of love, pass me that cocoa; I’m starving”
Most excitingly, chocolate contains phenylethylamine, the “molecule of love” or, more accurately, lust. It has an effect similar to amphetamines, and while we can synthesize it in the body, we can also get it from certain foods. But…
Our body is so keen to get it that most of it is metabolized directly during digestion and doesn’t make it to the brain. Also, chocolate is not as good a source as cabbage—do with that information what you will!
However!
Chocolate contains theobromine and small amounts of caffeine, both stimulants and both generally likely to improve mood; it also contains flavonoids which in turn stimulate production of nitric oxide, which is a relaxant. All in all, things that are convivial to having a good time.
On the other hand…
That relaxation comes specifically with a reduction in blood pressure—something typically considered good for the health for most people most of the time… but that means lowering blood pressure in all parts of your body, which could be the opposite of what you want in intimate moments.
Chocolate also contains zinc, which is essential for hormonal health for most people—the body uses it to produce testosterone and estrogen, respectively. Zinc supplements are popularly sold to those wishing to have more energy in general and good hormonal health in particular, and rightly so. However…
This approach requires long-term supplementation—you can’t just pop a zinc tablet / bar of chocolate / almond before bed and expect immediate results. And if your daily zinc supplementation takes the form of a 3.5oz (100g) bar of chocolate, then you may find it has more effects on your health, and not all of them good!
The Verdict: dark chocolate, in moderation, may promote “the mood”, but could be a double-edged sword when it comes to “the ability”.
“Chocolate Is Good During Menstruation”
The popular wisdom goes that chocolate is rich in iron (of which more is needed during menstruation), and indeed, if you eat 7oz (150g) of dark chocolate made with 85% cocoa, you’ll get a daily a dose of iron (…and nearly 1,000 calories).
More bang-for-buck dietary sources of iron include chickpeas and broccoli, but for some mysterious reason, these are not as commonly reported as popular cravings.
The real explanation for chocolate cravings is more likely that eating chocolate—a food high in sugar and fat along with a chemical bombardment of more specialized “hey, it’s OK, you can relax now” molecules (flavanols/flavonoids, polyphenols, phenylamines, even phenylethylamine, etc) gives a simultaneous dopamine kick (the body’s main “reward” chemical) with a whole-body physiological relaxation… so, little wonder we might crave it in times of stress and discomfort!
The Verdict: it helps, not because it serves a special nutritional purpose, but rather, because the experience of eating chocolate makes us feel good.
Fun fact: Tiramisu (this writer’s favorite dessert) is literally Italian for “pick-me-up”
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Shedding Some Obesity Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s shed some obesity myths!
There are a lot of myths and misconceptions surrounding obesity… And then there are also reactive opposite myths and misconceptions, which can sometimes be just as harmful!
To tackle them all would take a book, but in classic 10almonds style, we’re going to put a spotlight on some of the ones that might make the biggest difference:
True or False: Obesity is genetically pre-determined
False… With caveats.
Some interesting results have been found from twin studies and adoption studies, showing that genes definitely play some role, but lifestyle is—for most people—the biggest factor:
- The body-mass index of twins who have been reared apart
- An adoption study of human obesity
- Using a sibling-adoption design to parse genetic and environmental influences on children’s body mass index
In short: genes predispose; they don’t predetermine. But that predisposition alone can make quite a big difference, if it in turn leads to different lifestyle factors.
But upon seeing those papers centering BMI, let’s consider…
True or False: BMI is a good, accurate measure of health in the context of bodyweight
False… Unless you’re a very large group of thin white men of moderate height, which was the demographic the system was built around.
Bonus information: it was never intended to be used to measure the weight-related health of any individual (not even an individual thin white man of moderate height), but rather, as a tool to look at large-scale demographic trends.
Basically, as a system, it’s being used in a way it was never made for, and the results of that misappropriation of an epidemiological tool for individual health are predictably unhelpful.
To do a deep-dive into all the flaws of the BMI system, which are many, we’d need to devote a whole main feature just to that.
Update: we have now done so!
Here it is: When BMI Doesn’t Measure Up
True or False: Obesity does not meaningfully impact more general health
False… In more ways than one (but there are caveats)
Obesity is highly correlated with increased risk of all-cause mortality, and weight loss, correspondingly, correlates with a reduced risk. See for example:
So what are the caveats?
Let’s put it this way: owning a horse is highly correlated with increased healthy longevity. And while owning a horse may come with some exercise and relaxation (both of which are good for the health), it’s probably mostly not the horse itself that conveys the health benefits… it’s that someone who has the resources to look after a horse, probably has the resources to look after their own health too.
So sometimes there can be a reason for a correlation (it’s not a coincidence!) but the causative factor is partially (or in some cases, entirely) something else.
So how could this play out with obesity?
There’s a lot of discrimination in healthcare settings, unfortunately! In this case, it often happens that a thin person goes in with a medical problem and gets treated for that, while a fat person can go in with the same medical problem and be told “you should try losing some weight”.
Top tip if this happens to you… Ask: “what would you advise/prescribe to a thin person with my same symptoms?”
Other things may be more systemic, for example:
When a thin person goes to get their blood pressure taken, and that goes smoothly, while a fat person goes to get their blood pressure taken, and there’s not a blood pressure cuff to fit them, is the problem the size of the person or the size of the cuff? It all depends on perspective, in a world built around thin people.
That’s a trivial-seeming example, but the same principle has far-reaching (and harmful) implications in healthcare in general, e.g:
- Surgeons being untrained (and/or unwilling) to operate on fat people
- Getting a one-size-fits-all dose that was calculated using average weight, and now doesn’t work
- MRI machines are famously claustrophobia-inducing for thin people; now try not fitting in it in the first place
…and so forth. So oftentimes, obesity will be correlated with a poor healthcare outcome, where the problem is not actually the obesity itself, but rather the system having been set up with thin people in mind.
It would be like saying “Having O- blood type results in higher risks when receiving blood transfusions”, while omitting to add “…because we didn’t stock O- blood”.
True or False: to reduce obesity, just eat less and move more!
False… Mostly.
Moving more is almost always good for most people. When it comes to diet, quality is much more important than quantity. But these factors alone are only part of the picture!
But beyond diet and exercise, there are many other implicated factors in weight gain, weight maintenance, and weight loss, including but not limited to:
- Disrupted sleep
- Chronic stress
- Chronic pain
- Hormonal imbalances
- Physical disabilities that preclude a lot of exercise
- Mental health issues that add (and compound) extra levels of challenge
- Medications that throw all kinds of spanners into the works with their side effects
…and even just those first two things, diet and exercise, are not always so correlated to weight as one might think—studies have found that the difference for exercise especially is often marginal:
Read: Widespread misconceptions about obesity ← academic article in the Journal of the College of Family Physicians of Canada
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Which B Vitamins? It Makes A Difference
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Everyone knows “B vitamins are for energy!” and that is definitely a theme, but there’s a lot more to it than that, and in some cases, there are big mistakes that people make when it comes to supplementing their diet.
First, let’s do a quick overview of what each of the B vitamins do, by number, and putting names to them:
B1 (Thiamine)
- Function: helps convert carbohydrates into energy, supports nerve function
- Forms: thiamine hydrochloride, thiamine mononitrate, benfotiamine (fat-soluble form)
- Example foods: lentils, sunflower seeds
B2 (Riboflavin)
- Function: supports energy production, skin health, and eye function, turns your pee fluorescent yellow (the latter is really only if you consume exciting amounts of it; this will usually occur from supplementation, not from normal diet)
- Forms: riboflavin, riboflavin-5’-phosphate
- Example foods: almonds, mushrooms
B3 (Niacin)
- Function: aids metabolism, supports skin, nerves, and cholesterol levels
- Forms: niacin (nicotinic acid), niacinamide (nicotinamide), inositol hexanicotinate (flush-free niacin)
- Example foods: whole grains, peanuts (literally the best nut for this)
B5 (Pantothenic Acid)
- Function: essential for fatty acid metabolism and hormone production
- Forms: pantothenic acid, calcium pantothenate, panthenol (alcohol form!)
- Example foods: it’s in pretty much everything (hence the name); it’s almost impossible to be deficient in this vitamin unless you are literally starving
B6 (Pyridoxine)
- Function: needed for red blood cell production, supports brain function, as well as specifically being a part of neurotransmitter production (including dopamine and serotonin, despite them being made in different places—the brain and the gut, respectively),
- Forms: pyridoxine hydrochloride, pyridoxal-5’-phosphate (active form)
- Example foods: bananas, potatoes
B7 (Biotin)
- Function: helps with fatty acid synthesis, skin, hair, and nail health
- Forms: d-biotin, biotinylated compounds of various kinds
- Example foods: fava beans, walnuts
B9 (Folate/Folic Acid)
- Function: crucial for DNA synthesis, cell division, and fetal development
- Forms: folic acid, folinic acid, 5-methyltetrahydrofolate (5-MTHF, active form)
- Example foods: chickpeas, spinach ← we only mentioned one leafy green here for fairness, but leafy greens in general are great sources of vitamin B9, hence the name, from the Latin “folium”, meaning leaf.
B12 (Cobalamin)
- Function: supports red blood cell formation, nerve function, and DNA synthesis
- Forms: cyanocobalamin, methylcobalamin (active), hydroxocobalamin (active), adenosylcobalamin (active)
- Example foods: nutritional yeast, nori
You may be wondering: what about vitamins B4, B8, B10, and B11? Those are now vacant spots, that once contained things that are no longer considered vitamins.
Three Critical Vitamin B Mistakes That May Be Sabotaging Your Health
Some mistakes that people make include:
Not supplementing when necessary
This occurs most often after midlife, especially in women, and the most common deficiencies are B1, B9, and B12.
See also: These Signs Often Mean These Nutrient Deficiencies (Do You Have Any?)
While it’s tempting to think “if I have a good balanced diet, I won’t need…” but the fact is sometimes our diet isn’t as nutrient dense as we hope—often through no fault of our own! But many modern farming methods prioritize yield over nutritional value, and that can result in plants and animals that do not have the nutritional qualities they “should”.
We wrote about this a while back, weighing up the “supplementation vs diet alone” dilemma:
Does Our Diet Need A Little Help? ← this also has a very useful chart of which vitamins people usually get too little or too much of. Note however that the statement of marginally excessive folate is slightly misleading, as the data pool contains men and women aged 18–65, while B9 is mostly needed more by women, and especially around childbirth or menopause, so B9 is actually a very common deficiency, but here it’s being balanced out lots of men getting too much (because every multivitamin has it).
Supplementing to excess
Most B vitamins have a very high maximum tolerable dose, because (with the exception of where we marked otherwise) they are water-soluble, which means that if you take more than you need, you’ll just pee it out later. Hence the famous fluorescence, for example.
However, the fat soluble form of vitamin B1 is harder to get in and harder to get out.
As for the others, problems usually only occur if you take enough to cause toxicity, faster than you pee it out. In other words, go easy on those Berocca drinks!
Nevertheless, there are other problems that can arise:
Vitamin B6 is essential—but too much can be toxic. Here’s what to know to stay safe ← tl;dr: there are issues with it causing peripheral neuropathy at doses over 10mg (the safe dose is disputed, so we’re mentioning the lowest safe dose here, but you can read about the others in the article)
Getting forms that don’t work so well
Those different forms we listed? They are not all created equal! For example:
- Folic acid is cheap; unfortunately, it’s not absorbed or used well
- Cyanocobalamin is cheap; unfortunately, it’s not absorbed or used well
Let us quote a recent book review of ours:
❝Rather, the most common forms of vitamins B9 and B12 provided in supplements are folic acid and cyanocobalamin, respectively, which as he demonstrates with extensive research to back up his claims, cannot be easily absorbed or used especially well.
About those vitamers: a vitamer is simply a form of a vitamin—most vitamins we need can arrive in a variety of forms. In the case of vitamins B9 and B12, he advocates for ditching vitamers folic acid and cyanocobalamin, cheap as they are, and springing for bioactive vitamers L-methylfolate, methylcobalamin, and adenosylcobalamin.
He also discusses (again, just as well-evidenced as the above things) why we might struggle to get enough from our diet after a certain age. For example, if trying to get these vitamins from meat, 50% of people over 50 cannot manufacture enough stomach acid to break down that protein to release the vitamins.
And as for methyl-B12 vitamers, you might expect you can get those from meat, and technically you can, but they don’t occur in all animals, just in one kind of animal. Specifically, the kind that has the largest brain-to-body ratio. However, eating the meat of this animal can result in protein folding errors in general and Creutzfeldt–Jakob disease in particular, so the author does not recommend eating humans, however nutritionally convenient that would be.
All this means that supplementation after a certain age really can be a sensible way to do it—but do it wisely, and pick the right vitamers.❞
You can read that review in full here: Your Vitamins are Obsolete: The Vitamer Revolution – by Dr. Sheldon Zablow
Want to try those latter two?
We don’t sell them, but here for your convenience are example products on Amazon:
L-methylfolate (active form of vitamin B9)
Methylcobalamin, adenosylcobalamin, & hydroxocobalamin (active forms of vitamin B12)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: