Can you get sunburnt or UV skin damage through car or home windows?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When you’re in a car, train or bus, do you choose a seat to avoid being in the sun or do you like the sunny side?
You can definitely feel the sun’s heat through a window. But can you get sunburn or skin damage when in your car or inside with the windows closed?
Let’s look at how much UV (ultraviolet) radiation passes through different types of glass, how tinting can help block UV, and whether we need sunscreen when driving or indoors.

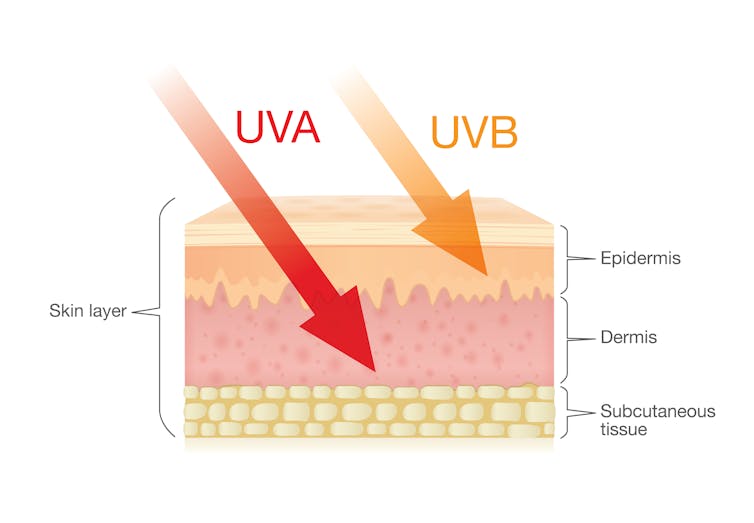
What’s the difference between UVA and UVB?
Of the total UV radiation that reaches Earth, about 95% is UVA and 5% is UVB.
UVB only reaches the upper layers of our skin but is the major cause of sunburn, cataracts and skin cancer.
UVA penetrates deeper into our skin and causes cell damage that leads to skin cancer.
Glass blocks UVA and UVB radiation differently
All glass used in house, office and car windows completely blocks UVB from passing through.
But only laminated glass can completely block UVA. UVA can pass through other glass used in car, house and office windows and cause skin damage, increasing the risk of cancer.
Car windscreens block UVA, but the side and rear windows don’t
A car’s front windscreen lets in lots of sunshine and light. Luckily it blocks 98% of UVA radiation because it is made of two layers of laminated glass.
But the side and rear car windows are made of tempered glass, which doesn’t completely block UVA. A study of 29 cars found a range from 4% to almost 56% of UVA passed through the side and rear windows.
The UVA protection was not related to the car’s age or cost, but to the type of glass, its colour and whether it has been tinted or coated in a protective film. Grey or bronze coloured glass, and window tinting, all increase UVA protection. Window tinting blocks around 95% of UVA radiation.
In a separate study from Saudi Arabia, researchers fitted drivers with a wearable radiation monitor. They found drivers were exposed to UV index ratings up to 3.5. (In Australia, sun protection is generally recommended when the UV index is 3 or above – at this level it takes pale skin about 20 minutes to burn.)
So if you have your windows tinted, you should not have to wear sunscreen in the car. But without tinted windows, you can accumulate skin damage.
UV exposure while driving increases skin cancer risk
Many people spend a lot of time in the car – for work, commuting, holiday travel and general transport. Repeated UVA radiation exposure through car side windows might go unnoticed, but it can affect our skin.
Indeed, skin cancer is more common on the driver’s side of the body. A study in the United States (where drivers sit on the left side) found more skin cancers on the left than the right side for the face, scalp, arm and leg, including 20 times more for the arm.
Another US study found this effect was higher in men. For melanoma in situ, an early form of melanoma, 74% of these cancers were on the on the left versus 26% on the right.
Earlier Australian studies reported more skin damage and more skin cancer on the right side.
Cataracts and other eye damage are also more common on the driver’s side of the body.
What about UV exposure through home or office windows?
We see UV damage from sunlight through our home windows in faded materials, furniture or plastics.
Most glass used in residential windows lets a lot of UVA pass through, between 45 and 75%.

Single-pane glass lets through the most UVA, while thicker, tinted or coated glass blocks more UVA.
The best options are laminated glass, or double-glazed, tinted windows that allow less than 1% of UVA through.
Skylights are made from laminated glass, which completely stops UVA from passing through.
Most office and commercial window glass has better UVA protection than residential windows, allowing less than 25% of UVA transmission. These windows are usually double-glazed and tinted, with reflective properties or UV-absorbent chemicals.
Some smart windows that reduce heat using chemical treatments to darken the glass can also block UVA.
So when should you wear sunscreen and sunglasses?
The biggest risk with skin damage while driving is having the windows down or your arm out the window in direct sun. Even untinted windows will reduce UVA exposure to some extent, so it’s better to have the car window up.
For home windows, window films or tint can increase UVA protection of single pane glass. UVA blocking by glass is similar to protection by sunscreen.
When you need to use sunscreen depends on your skin type, latitude and time of the year. In a car without tinted windows, you could burn after one hour in the middle of the day in summer, and two hours in the middle of a winter’s day.
But in the middle of the day next to a home window that allows more UVA to pass through, it could take only 30 minutes to burn in summer and one hour in winter.
When the UV index is above three, it is recommended you wear protective sunglasses while driving or next to a sunny window to avoid eye damage.
Theresa Larkin, Associate Professor of Medical Sciences, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Captivate – by Vanessa van Edwards

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book isn’t just for one area of human interactions. It covers everything from the boardroom to the bedroom (not necessarily a progression with the same person!), business associates, friends, partners, kids, and more.
She presents information in a layered manner, covering for example, chapter-by-chapter:
- the first five minutes
- the first five hours
- the first five days
She also covers such things as:
- starting conversations in a way that makes you memorable (without making it weird!)
- the importance of really listening (and how to do that)
- collecting like-minded people appropriately
- introducing other people! Because a) it’s not all about you, but also b) you’re the person who knows everybody now
- where to stand at parties / networking events!
- dating and early-days dating messages
- reading the room, reading the people
All in all, a great resource for anyone who wants to make (and maintain!) meaningful relationships with those around you.
Share This Post
-

10 Mistakes To Sabotage Your Ozempic Progress
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ozempic has a good reputation for getting reliable results, but there are ways to mess it up:
It’s not just inject-and-go
We’ll not keep the 10 ways a secret; they are:
- Increasing the dose too quickly: avoid cranking doses up too high too quickly, to prevent severe nausea, appetite suppression, and muscle loss. It’s worth being aware that high doses without proper management can lead to metabolic health disasters.
- Pushing through side effects: severe nausea or vomiting means you probably have an unhelpfully high dose; consult your prescribing doctor—it’s easy to feel “more is better; I don’t want to have less!”, but there really is a sweet spot, and if you’re not in it, then adjustments are needed in order to find it.
- Eating nutritionally scant food: reducing the quantity of unhealthy food isn’t enough—please prioritize nutrient-rich foods instead. Remember, “it’s not the calories in your food; it’s the food in your calories”.
- Consuming fried food and refined carbs: their general metabolic woes aside, fried foods and ultra-refined carbs can exacerbate nausea and other side effects, so it really is best to skip them. The good news is that Ozempic will help overcome those cravings more easily.
- Neglecting muscle protection: especially women, especially middle-aged or older, are at higher risk of osteoporosis and should maintain muscle mass (strong muscles and strong bones go together, by necessity). So, eat protein and do resistance training!
- Assuming it’s a monotherapy: GLP-1 drugs work best as part of a holistic protocol, including proper nutrition, strength training, and hormone therapy if appropriate.
- Not addressing metabolic health first: GLP-1 drugs are less effective in people with poor baseline metabolic health, so there’s a bit of a catch-22 here, but it’s important to be aware of. Fortunately, Ozempic and adopting a healthy lifestyle will each make the other work better.
- Neglecting comprehensive treatment plans: in other words, going through the motions of a holistic protocol and then expecting Ozempic to do all the work.
- Upping doses to overcome plateaus: plateaus often signal other issues (e.g. lack of protein, no strength training), so do address these before increasing dosage.
- Lack of collaboration with doctors: the human body is complex, and what’s going on metabolically is complex too, so there’s a lot a layperson can easily miss. For that matter, there’s a lot that doctors can easily miss too, but more heads are better than one.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
5 Ways To Naturally Boost The Ozempic Effect
Take care!
Share This Post
-

Hair-Loss Remedies, By Science
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
10almonds Gets Hairy
Hair loss is a thing that at some point affects most men and a large minority of women. It can be a source of considerable dysphoria for both, as it’s often seen as a loss of virility/femininity respectively, and is societally stigmatized in various ways.
Today we’re going to focus on the most common kind: androgenic alopecia, which is called “male pattern baldness” in men and “female pattern baldness” in women, despite being the same thing.
We won’t spend a lot of time on the science of why this happens (we’re going to focus on the remedies instead), but suffice it to say that genes and hormones both play a role, with dihydrogen testosterone (DHT) being the primary villain in this case.
We’ve talked before about the science of 5α-reductase inhibitors to block the conversion of regular testosterone* to DHT, its more potent form:
One Man’s Saw Palmetto Is Another Woman’s Serenoa Repens…
*We all make this to a greater or lesser degree, unless we have had our ovaries/testes removed.
Finasteride
Finasteride is a 5α-reductase inhibitor that performs similarly to saw palmetto, but comes in tiny pills instead of needing to take a much higher dose of supplement (5mg of finasteride is comparable in efficacy to a little over 300mg of saw palmetto).
Does it work? Yes!
Any drawbacks? A few:
- It’ll take 3–6 months to start seeing effects. This is because of the hormonal life-cycle of human hairs.
- Common side-effects include ED.
- It is popularly labelled/prescribed as “only for men”
On that latter point: the warnings about this are severe, detailing how women must not take it, must not even touch it if it has been cut up or crushed.
However… That’s because it can carry a big risk to our unborn fetuses. So, if we are confident we definitely don’t have one of those, it’s not actually applicable to us.
That said, finasteride’s results in women aren’t nearly so clear-cut as in men (though also, there has been less research, largely because of the above). Here’s an interesting breakdown in more words than we have room for here:
Finasteride for Women: Everything You Need to Know
Spironolactone
This one’s generally prescribed to women, not men, largely because it’s the drug sometimes popularly known as a “chemical castration” drug, which isn’t typically great marketing for men (although it can be applied topically, which will have less of an effect on the rest of the body). For women, this risk is simply not an issue.
We’ll be brief on this one, but we’ll just drop this, so that you know it’s an option that works:
❝Spironolactone is an effective and safe treatment of androgenic alopecia which can enhance the efficacy when combined with other conventional treatments such as minoxidil.
Topical spironolactone is safer than oral administration and is suitable for both male and female patients, and is expected to become a common drug for those who do not have a good response to minoxidil❞
Minoxidil
This one is available (to men and women) without prescription. It’s applied topically, and works by shortcutting the hair’s hormonal growth cycle, to reduce the resting phase and kick it into a growth phase.
Does it work? Yes!
Any drawbacks? A few:
- Whereas you’ll remember finasteride takes 3–6 months to see any effect, this one will have an effect very quickly
- Specifically, the immediate effect is: your rate of hair loss will appear to dramatically speed up
- This happens because when hairs are kicked into their growth phase if they were in a resting phase, the first part of that growth phase is to shed each old hair to make room for the new one
- You’ll then need the same 3–6 months as with finasteride, to see the regrowth effects
- If you stop using it, you will immediately shed whatever hair you gained by this method
Why do people choose this over finasteride? For one of three reasons, mainly:
- They are women, and not offered finasteride
- They are men, and do not want the side effects of finasteride
- They just saw an ad and tried it
As to how it works:
Some final notes:
There are some other contraindications and warnings with each of these drugs by the way, so do speak with your doctor/pharmacist. For example:
- Finasteride can tax the liver a little
- Spironolactone can reduce bone turnover
- Minoxidil is a hypotensive; this shouldn’t be an issue for most people, but for some people it could be a problem
There are other hair loss remedies and practices, but the above three are the heavy-hitters, so that’s what we spent our time/space on today. We’ll perhaps cover the less powerful (but less risky) options one of these days.
Meanwhile, take care!
Share This Post
Related Posts
-
Stimulant Users Are Caught in Fatal ‘Fourth Wave’ of Opioid Epidemic
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In Pawtucket, Rhode Island, near a storefront advertising “free” cellphones, J.R. sat in an empty back stairwell and showed a reporter how he tries to avoid overdosing when he smokes crack cocaine. KFF Health News is identifying him by his initials because he fears being arrested for using illegal drugs.
It had been several hours since his last hit, and the chatty, middle-aged man’s hands moved quickly. In one hand, he held a glass pipe. In the other, a lentil-size crumb of cocaine.
Or at least J.R. hoped it was cocaine, pure cocaine — uncontaminated by fentanyl, a potent opioid that was linked to about 75% of all overdose deaths in Rhode Island in 2022. He flicked his lighter to “test” his supply. He believed that if it had a “cigar-like sweet smell,” he said, it would mean that the cocaine was laced with fentanyl. He put the pipe to his lips and took a tentative puff. “No sweet,” he said, reassured.
But this method offers only false and dangerous reassurance. A mistake can be fatal.
It is impossible to tell whether a drug contains fentanyl by the taste or smell. “Somebody can believe that they can smell it or taste it, or see it … but that’s not a scientific test,” said Josiah “Jody” Rich, an addiction specialist and researcher who teaches at Brown University. “People are going to die today because they buy some cocaine that they don’t know has fentanyl in it.”
The first wave of the long-running and devastating opioid epidemic began in the United States with the abuse of prescription painkillers in the early 2000s. The second wave involved an increase in heroin use, starting around 2010. The third wave began when powerful synthetic opioids such as fentanyl started appearing in the supply around 2015. Now experts are observing a fourth phase of the deadly epidemic.
The mix of stimulants such as cocaine and methamphetamines with fentanyl — a synthetic opioid 50 times as powerful as heroin — is driving what experts call the opioid epidemic’s “fourth wave.” The mixture of stimulants and fentanyl presents powerful challenges to efforts to reduce overdoses because many users of stimulants don’t know they are at risk of ingesting opioids, so they don’t take overdose precautions.
The only way to know whether cocaine or other stimulants contain fentanyl is to use drug-checking tools such as fentanyl test strips — a best practice for what’s known as “harm reduction,” now embraced by federal health officials in combating drug overdose deaths. Fentanyl test strips cost as little as $2 for a two-pack online, but many front-line organizations also give them out free.
Nationwide, illicit stimulants mixed with fentanyl were the most common drugs found in fentanyl-related overdoses, according to a study published in 2023 in the scientific journal Addiction. The stimulant in the fatal mixture tends to be cocaine in the Northeast, and methamphetamine in the West and much of the Midwest and South.
“The No. 1 thing that people in the U.S. are dying from in terms of drug overdoses is the combination of fentanyl and a stimulant,’’ said Joseph Friedman, a researcher at UCLA and the study’s lead author. “Black and African Americans are disproportionately affected by this crisis to a large magnitude, especially in the Northeast.”
Friedman was also the lead author of another new study, published in the American Journal of Psychiatry, that shows the fourth wave of the opioid epidemic is driving up the mortality rate among older Black Americans (ages 55-64) and, more recently, Hispanic people. Friedman said part of the reason street fentanyl is so deadly is that there’s no way to tell how potent it is. Hospitals have safely used medical-grade fentanyl for surgical pain because the potency is strictly regulated, but “the potency fluctuates wildly in the illicit market” Friedman said.
Studies of street drugs, he said, show that in illicit drugs the potency can vary from 1% to 70% fentanyl.
“Imagine ordering a mixed drink in a bar and it contains one to 70 shots,” Friedman said, “and the only way you know is to start drinking it. … There would be a huge number of alcohol overdose deaths.”
Drug-checking technology can provide a rough estimate of fentanyl concentration, he said, but to get a precise measure requires sending drugs to a laboratory.
It’s not clear how much of the latest trend in polydrug use — in which users mix substances, such as cocaine and fentanyl, for example — is accidental versus intentional. It can vary for individual users: a recent study from Millennium Health found that most people who use fentanyl do so at times intentionally and other times unintentionally.
People often use stimulants to power through the rapid withdrawal from fentanyl, Friedman said. And the high-risk practice of using cocaine or meth with heroin, known as “speedballing,” has been around for decades. Other factors include manufacturers’ adding the cheap synthetic opioid to a stimulant to stretch their supply, or dealers mixing up bags.
Researchers say many people still think they are using unadulterated cocaine or crack — a misconception that can be deadly. “Folks who are using stimulants, and not intentionally using opioids, are unprepared to respond to an opioid overdose,” said Brown University epidemiologist Jaclyn White Hughto, “because they don’t perceive themselves to be at risk.” Hughto is a principal investigator in a new, unpublished study called “Preventing Overdoses Involving Stimulants.”
Hughto and the team surveyed more than 260 people in Rhode Island and Massachusetts who use drugs, including some who manufacture and distribute stimulants such as cocaine. More than 60% of the people they interviewed in Rhode Island had bought or used stimulants that they later found out had fentanyl in them. And many of the people interviewed in the study also use drugs alone. That means that if they do overdose, they may not be found until it’s too late.
In 2022, Rhode Island had the fourth-highest rate of overdose deaths involving cocaine in 2022, after Washington, D.C., Delaware, and Vermont, according to the Centers for Disease Control and Prevention.
The fourth wave is also hitting stimulant users who choose pills over what they perceive as more dangerous drugs such as cocaine in an effort to avoid fentanyl. That’s what happened to Jennifer Dubois’ son Cliffton.
Dubois was a single mother raising two Black sons. The older son, Cliffton, had been struggling with addiction since he was 14, she said. Cliffton also had been diagnosed with attention-deficit/hyperactivity disorder and a mood disorder.
In March 2020, Cliffton had checked into a rehab program as the pandemic ramped up, Dubois said. Because of the lockdown at rehab, Cliffton was upset about not being able to visit with his mother. “He said, ‘If I can’t see my mom, I can’t do treatment,’” Dubois recalled. “And I begged him” to stay in treatment.
But soon after, Cliffton left the rehab program. He showed up at her door. “And I just cried,” she said.
Dubois’ younger son was living at home. She didn’t want Cliffton doing drugs around his younger brother. So she gave Cliffton an ultimatum: “If you want to stay home, you have to stay drug-free.”
Cliffton went to stay with family friends, first in Atlanta and later in Woonsocket, an old mill city that has Rhode Island’s highest rate of drug overdose deaths.
In August 2020, Cliffton overdosed but was revived. Cliffton later confided that he’d been snorting cocaine in a car with a friend, Dubois said. Hospital records show he tested positive for fentanyl.
“He was really scared,” Dubois said. After the overdose, he tried to “leave the cocaine and the hard drugs alone,” she said. “But he was taking pills.” Eight months later, on April 17, 2021, Cliffton was found unresponsive in the bedroom of a family member’s home.
The night before, Cliffton had bought counterfeit Adderall, according to the police report. What he didn’t know was that the Adderall pill was laced with fentanyl. “He thought by staying away from the street drugs and just taking pills, he was doing better,” Dubois said.
A fentanyl test strip could have saved his life.
This article is from a partnership that includes The Public’s Radio, NPR, and KFF Health News.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fix Tight Hamstrings In Just 3 Steps
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There’s a better way to increase your flexibility than just stretching and stretching and hoping for the best. Here’s a 3-step method that will transform your flexibility:
As easy as 1-2-3
Only one part actually involves stretching:
Step 1: reciprocal inhibition
- Concept: when one muscle contracts, the opposing muscle relaxes—which is what we need.
- Goal: engage hip flexors to encourage hamstring relaxation.
- Method:
- Kneeling hamstring stretch position with one leg forward.
- Support with yoga blocks or a chair; use a cushion for comfort.
- Maintain a slight arch in the lower back and hinge forward slightly.
- Attempt to lift the foot off the floor, even if it doesn’t move.
- Hold for around 10 seconds.
Step 2: engaging more muscle fibers
- Concept: our muscles contain a lot of fibers, and often not all of them come along for the ride when we do something (exercising, stretching, etc), and those fibers that weren’t engaged will hold back the whole process.
- Goal: activate more fibers in the hamstring for a deeper stretch.
- Method:
- Same kneeling position, slight back arch, and forward hinge.
- Drive the heel into the floor as if trying to dent it.
- Apply significant effort but hold for only 10 seconds.
- A small bend in the knee is acceptable.
Step 3: manipulating the nervous system
- Concept: the nervous system often limits flexibility due to safety signals (causing sensations of discomfort to tell us to stop a lot sooner than we really need to).
- Goal: passive stretching to reduce nervous system resistance.
- Method:
- Avoid muscle engagement or movement—stay completely relaxed.
- Focus on calmness, with slow, steady breaths.
- Avoid signs of tension (e.g. clenched fists, short/sharp breathing). While your nervous system is trying to communicate to you that you are in danger, you need to communicate to your nervous system that this is fine actually, so in order to reassure your nervous system you need to avoid signs that will tip it off that you’re worried too.
- Don’t overstretch; prioritize a relaxed, safe feeling.
For more on all of this, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Tight Hamstrings? Here’s A Test To Know If It’s Actually Your Sciatic Nerve
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Science-Backed Anti-Inflammatory Diet for Beginners – by Dr. Yasmine Elamir & Dr. William Grist
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have written about how to eat to beat inflammation, but what we didn’t do is include 75 recipes and a plan for building up one’s culinary repertoire around those core dishes!
That’s what this book does. It covers briefly the science of inflammation and anti-inflammatory diet, discusses experimental elimination diets (e.g. you eliminate likely culprits of triggering your inflammation, then reintroduce them one by one to see which it was), and ingredients likely to increase or decrease inflammation.
The 75 recipes are good, and/but a caveat is “yes, one of the recipes is ketchup and another is sour cream” so it’s not exactly 75 mains.
However! Where this book excels is in producing anti-inflammatory versions of commonly inflammatory dishes. That ketchup? Not sugary. The sour cream? Vegan. And so forth. We also see crispy roast potatoes, an array of desserts, and sections for popular holiday dishes too, so you will not need to be suddenly inflamed into the next dimension when it comes to festive eating.
The recipes are what the title claims them to be, “science-backed anti-inflammatory”, and that is clearly the main criterion for their inclusion. They are not by default vegan, vegetarian, dairy-free, nut-free, gluten-free, etc. For this reason, all recipes are marked with such tags as “V, VG, DF, GF, EF, NF” etc as applicable.
Bottom line: we’d consider this book more of a jumping-off point than a complete repertoire, but it’s a very good jumping-off point, and will definitely get you “up and running” (there’s a 21-day meal plan, for example).
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: