How To Grow New Brain Cells (At Any Age)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Grow New Brain Cells (At Any Age)
It was long believed that brain growth could not occur later in life, due to expending our innate stock of pluripotent stem cells. However, this was mostly based on rodent studies.
Rodent studies are often used for brain research, because it’s difficult to find human volunteers willing to have their brains sliced thinly (so that the cells can be viewed under a microscope) at the end of the study.
However, neurobiologist Dr. Maura Boldrini led a team that did a lot of research by means of autopsies on the hippocampi of (previously) healthy individuals ranging in age from 14 to 79.
What she found is that while indeed the younger subjects did predictably have more young brain cells (neural progenitors and immature neurons), even the oldest subject, at the age of 79, had been producing new brain cells up until death.
Read her landmark study: Human Hippocampal Neurogenesis Persists throughout Aging
There was briefly a flurry of news articles about a study by Dr. Shawn Sorrels that refuted this, however, it later came to light that Dr. Sorrels had accidentally destroyed his own evidence during the cell-fixing process—these things happen; it’s just unfortunate the mistake was not picked up until after publication.
A later study by a Dr. Elena Moreno-Jiménez fixed this flaw by using a shorter fixation time for the cell samples they wanted to look at, and found that there were tens of thousands of newly-made brain cells in samples from adults ranging from 43 to 87.
Now, there was still a difference: the samples from the youngest adult had 30% more newly-made braincells than the 87-year-old, but given that previous science thought brain cell generation stopped in childhood, the fact that an 87-year-old was generating new brain cells 30% less quickly than a 43-year-old is hardly much of a criticism!
As an aside: samples from patients with Alzheimer’s also had a 30% reduction in new braincell generation, compared to samples from patients of the same age without Alzheimer’s. But again… Even patients with Alzheimer’s were still growing some new brain cells.
Read it for yourself: Adult hippocampal neurogenesis is abundant in neurologically healthy subjects and drops sharply in patients with Alzheimer’s disease
Practical advice based on this information
Since we can do neurogenesis at any age, but the rate does drop with age (and drops sharply in the case of Alzheimer’s disease), we need to:
Feed your brain. The brain is the most calorie-consuming organ we have, by far, and it’s also made mostly of fat* and water. So, get plenty of healthy fats, and get plenty of water.
*Fun fact: while depictions in fiction (and/or chemically preserved brains) may lead many to believe the brain has a rubbery consistency, the untreated brain being made of mostly fat and water gives it more of a blancmange-like consistency in reality. That thing is delicate and spatters easily. There’s a reason it’s kept cushioned inside the strongest structure of our body, far more protected than anything in our torso.
Exercise. Specifically, exercise that gets your blood pumping. This (as our earlier-featured video today referenced) is one of the biggest things we can do to boost Brain-Derived Neurotrophic Factor, or BDNF.
Here be science: Brain-Derived Neurotrophic Factor, Depression, and Physical Activity: Making the Neuroplastic Connection
However, that’s not the only way to increase BDNF; another is to enjoy a diet rich in polyphenols. These can be found in, for example, berries, tea, coffee, and chocolate. Technically those last two are also botanically berries, but given how we usually consume them, and given how rich they are in polyphenols, they merit a special mention.
See for example: Effects of nutritional interventions on BDNF concentrations in humans: a systematic review
Some supplements can help neuron (re)growth too, so if you haven’t already, you might want to check out our previous main feature on lion’s mane mushroom, a supplement which does exactly that.
For those who like videos, you may also enjoy this TED talk by neuroscientist Dr. Sandrine Thuret:
Prefer text? Click here to read the transcript
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cranberries vs Goji Berries – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cranberries to goji berries, we picked the cranberries.
Why?
Both are great! And your priorities may differ. Here’s how they stack up:
In terms of macros, goji berries have more protein, carbs, and fiber. This is consistent with them generally being eaten very dried, whereas cranberries are more often eaten fresh or from frozen, or partially rehydrated. In any case, goji berries are the “more food per food” option, so it wins this category. The glycemic indices are both low, by the way, though goji berries are the lower.
When it comes to vitamins, cranberries have more of vitamins B1, B2, B3, B5, B6, B9, E, K, and choline, while goji berries have more of vitamins A and C. Admittedly it’s a lot more, but still, on strength of overall vitamin coverage, the clear winner here is cranberries.
We see a similar story when it comes to minerals: cranberries have more copper, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while goji berries have (a lot) more calcium and iron. Again, by strength of overall mineral coverage, the clear winner here is cranberries.
Cranberries do also have some extra phytochemical benefits, including their prevention/cure status when it comes to UTIs—see our link below for more on that.
At any rate, enjoy either or both, but those are the strengths and weaknesses of these two berries!
Want to learn more?
You might like to read:
- Health Benefits Of Cranberries (But: You’d Better Watch Out)
- Goji Berries: Which Benefits Do They Really Have?
- The Sugary Food That Lowers Blood Sugars ← this is also about goji berries
Take care!
Share This Post
-
Kidney Beans vs Pinto Beans – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kidney beans to pinto beans, we picked the pinto.
Why?
Looking at the macros first, pinto beans have slightly more protein and carbs, and a lot more fiber, making them the all-round “more food per food” choice.
In the vitamins category, kidney beans have more of vitamins B3, C, and K, while pinto beans have more of vitamins B1, B2, B6, B9, E, and choline; another win for pinto beans. In kidney beans’ defense though, with the exception of vitamin E (31x more in pinto beans) the margins of difference are small for the rest of these vitamins, making kidney beans a close runner-up. Still, at least a nominal win for pinto beans here, by the numbers.
When it comes to minerals, kidney beans are not higher in any minerals, while pinto beans have more calcium, copper, magnesium, manganese, phosphorus, potassium, and selenium. In kidney beans’ defense, though, with the exception of selenium (5–6x more in pinto beans) the margins of difference are small for the rest of these minerals, making kidney beans a fine choice here too. Once again though, a winner is declarable here by the numbers, and it’s pinto beans.
Adding up the three wins makes for one big win for pinto beans. Still, enjoy either or both, because kidney beans are great too, and so is diversity!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Take care!
Share This Post
-
Honeydew vs Cantaloupe – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing honeydew to cantaloupe, we picked the cantaloupe.
Why?
In terms of macros, there’s not a lot between them—they’re both mostly water. Nominally, honeydew has more carbs while cantaloupe has more fiber and protein, but the differences are very small. So, a very slight win for cantaloupe.
Looking at vitamins: honeydew has slightly more of vitamins B5 and B6 (so, the vitamins that are in pretty much everything), while cantaloupe has a more of vitamins A, B1, B2, B3, C, and E (especially notably 67x more vitamin A, whence its color). A more convincing win for cantaloupe.
The minerals category is even more polarized: honeydew has more selenium (and for what it’s worth, more sodium too, though that’s not usually a plus for most of us in the industrialized world), while cantaloupe has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc. An overwhelming win for cantaloupe.
No surprises: adding up the slight win for cantaloupe, the convincing win for cantaloupe, and the overwhelming win for cantaloupe, makes cantaloupe the overall best pick here.
Enjoy!
Want to learn more?
You might like to read:
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
Take care!
Share This Post

-

Dreams: Relevance, Meanings, Interpretations
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I have a question or a suggestion for coverage in your “Psychology Sunday”. Dreams: their relevance, meanings ( if any) interpretations? I just wondered what the modern psychological opinions are about dreams in general.❞
We’ll indeed do that one of these Psychology Sundays! Thanks for suggesting it.
What we can say in advance is that there’s certainly not a single unified scientific consensus yet, but there are two or three prevailing views definitely worth covering, e.g. randomly generated, a by-product of reorganizing information in the brain, or expressions of subconscious thoughts/feelings.
There are also differences between a top-down/bottom-up approach to understanding dreaming, and efforts to tie those two together.
Watch this space!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Intermittent Fasting, Intermittently?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Have you come across any research on alternate-day intermittent fasting—specifically switching between one day of 16:8 fasting and the next day of regular eating patterns? I’m curious if there are any benefits or drawbacks to this alternating approach, or if the benefits mainly come from consistent intermittent fasting?❞
Short and unhelpful answer: no
Longer and hopefully more helpful answer:
As you probably know, usually people going for approaches based on the above terms either
- practise 16:8 fasting (fast for 16 hours each day, eat during an 8-hour window) or
- practise alternate-day fasting (fast for 24 hours, eat whenever for 24 hours, repeat)
…which latter scored the best results in this large meta-analysis of studies:
There is also the (popular) less extreme version of alternate-day fasting, sometimes called “eat stop eat”, which is not a very helpful description because that describes almost any kind of eating/fasting, but it usually refers to “once per week, take a day off from eating”.
You can read more about each of these (and some other variants), here:
Intermittent Fasting: What’s The Truth?
What you are describing (doing 16:8 fasting on alternate days, eating whenever on the other days) is essentially: intermittent fasting, just with one 16-hour fast per 48 hours instead of per the usual 24 hours.
See also: International consensus on fasting terminology ← the section on the terms “STF & PF” covers why this gets nudged back under the regular IF umbrella
Good news: this means there is a lot of literature into the acute (i.e., occurring the same day, not long-term)* benefits of 16:8 IF, and that means that you will be getting those benefits, every second day.
You remember that meta-analysis we posted above? While it isn’t mentioned in the conclusion (which only praised complete alternate-day fasting producing the best outcomes overall), sifting through the results data discovers that time-restricted eating (which is what you are doing, by these classifications) was the only fasting method to significantly reduce fasting blood glucose levels.
(However, no significant differences were observed between any IF form and the reference (continuous energy restriction, CER, i.e. calorie-controlled) diets in fasting insulin and HbA1c levels)
*This is still good news in the long-term though, because getting those benefits every second day is better than getting those benefits on no days, and this will have a long-term impact on your healthy longevity, just like how it is better to exercise every second day than it is to exercise no days, or better to abstain from alcohol every second day than it is to abstain on no days, etc.
In short, by doing IF every second day, you are still giving your organs a break sometimes, and that’s good.
All the same, if it would be convenient and practical for you, we would encourage you to consider either the complete alternate-day fasting (which, according to a lot of data, gives the best results overall),or time-restricted eating (TRE) every day (which, according to a lot of data, gives the best fasting blood sugar levels).
You could also improve the TRE days by shifting to 20:4 (i.e., 20 hours fasting and 4 hours eating), this giving your organs a longer break on those days.
Want to learn more?
For a much more comprehensive discussion of the strengths and weaknesses of different approaches to intermitted fasting, check out:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Our blood-brain barrier stops bugs and toxins getting to our brain. Here’s how it works
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our brain is an extremely complex and delicate organ. Our body fiercely protects it by holding onto things that help it and keeping harmful things out, such as bugs that can cause infection and toxins.
It does that though a protective layer called the blood-brain barrier. Here’s how it works, and what it means for drug design.

The Conversation, Rattiya Thongdumhyu/Shutterstock, Petr Ganaj/Pexels First, let’s look at the circulatory system
Adults have roughly 30 trillion cells in their body. Every cell needs a variety of nutrients and oxygen, and they produce waste, which needs to be taken away.
Our circulatory system provides this service, delivering nutrients and removing waste.
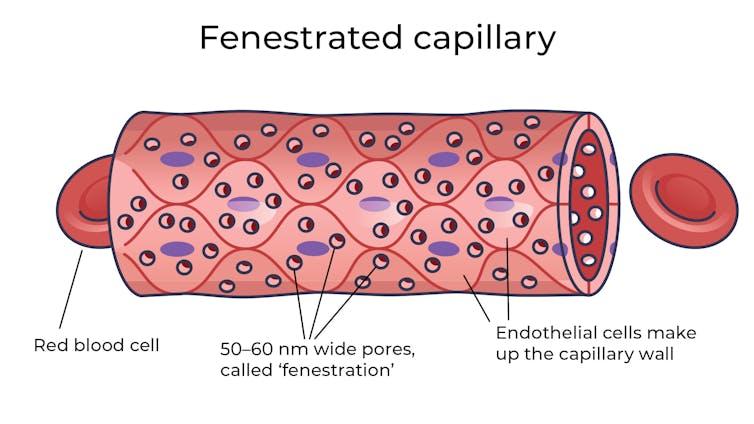
Fenestrated capillaries let nutrients and waste pass through. Vectormine/Shutterstock Where the circulatory system meets your cells, it branches down to tiny tubes called capillaries. These tiny tubes, about one-tenth the width of a human hair, are also made of cells.
But in most capillaries, there are some special features (known as fenestrations) that allow relatively free exchange of nutrients and waste between the blood and the cells of your tissues.
It’s kind of like pizza delivery
One way to think about the way the circulation works is like a pizza delivery person in a big city. On the really big roads (vessels) there are walls and you can’t walk up to the door of the house and pass someone the pizza.
But once you get down to the little suburban streets (capillaries), the design of the streets means you can stop, get off your scooter and walk up to the door to deliver the pizza (nutrients).
We often think of the brain as a spongy mass without much blood in it. In reality, the average brain has about 600 kilometres of blood vessels.
The difference between the capillaries in most of the brain and those elsewhere is that these capillaries are made of specialised cells that are very tightly joined together and limit the free exchange of anything dissolved in your blood. These are sometimes called continuous capillaries.
Continuous capillaries limit the free exchange of anything dissolved in your blood. Vectormine/Shutterstock This is the blood brain barrier. It’s not so much a bag around your brain stopping things from getting in and out but more like walls on all the streets, even the very small ones.
The only way pizza can get in is through special slots and these are just the right shape for the pizza box.
The blood brain barrier is set up so there are specialised transporters (like pizza box slots) for all the required nutrients. So mostly, the only things that can get in are things that there are transporters for or things that look very similar (on a molecular scale).
The analogy does fall down a little bit because the pizza box slot applies to nutrients that dissolve in water. Things that are highly soluble in fat can often bypass the slots in the wall.
Why do we have a blood-brain barrier?
The blood brain barrier is thought to exist for a few reasons.
First, it protects the brain from toxins you might eat (think chemicals that plants make) and viruses that often can infect the rest of your body but usually don’t make it to your brain.
It also provides protection by tightly regulating the movement of nutrients and waste in and out, providing a more stable environment than in the rest of the body.
Lastly, it serves to regulate passage of immune cells, preventing unnecessary inflammation which could damage cells in the brain.
What it means for medicines
One consequence of this tight regulation across the blood brain barrier is that if you want a medicine that gets to the brain, you need to consider how it will get in.
There are a few approaches. Highly fat-soluble molecules can often pass into the brain, so you might design your drug so it is a bit greasy.
The blood-brain barrier stops many medicines getting into the brain. Ron Lach/Pexels Another option is to link your medicine to another molecule that is normally taken up into the brain so it can hitch a ride, or a “pro-drug”, which looks like a molecule that is normally transported.
Using it to our advantage
You can also take advantage of the blood brain barrier.
Opioids used for pain relief often cause constipation. They do this because their target (opioid receptors) are also present in the nervous system of the intestines, where they act to slow movement of the intestinal contents.
Imodium (Loperamide), which is used to treat diarrhoea, is actually an opioid, but it has been specifically designed so it can’t cross the blood brain barrier.
This design means it can act on opioid receptors in the gastrointestinal tract, slowing down the movement of contents, but does not act on brain opioid receptors.
In contrast to Imodium, Ozempic and Victoza (originally designed for type 2 diabetes, but now popular for weight-loss) both have a long fat attached, to improve the length of time they stay in the body.
A consequence of having this long fat attached is that they can cross the blood-brain barrier, where they act to suppress appetite. This is part of the reason they are so effective as weight-loss drugs.
So while the blood brain barrier is important for protecting the brain it presents both a challenge and an opportunity for development of new medicines.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: