Aloe Vera vs Alzheimer’s Disease?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Regular 10almonds readers are probably already fairly on top of Alzheimer’s preventative measures, such as:
Alzheimer’s Causative Factors To Avoid
…but here’s a new development:
All about acetylcholine (and its friends)
Researchers (Dr. Meriem Khedraoui et al.) have investigated bioactive compounds from aloe vera as potential treatments for Alzheimer’s disease, using advanced computer modeling techniques.
Specifically, Dr. Khedraoui and her team focused on how the aloe vera compounds affected acetylcholinesterase and butyrylcholinesterase, two enzymes that break down acetylcholine, a neurotransmitter already reduced in Alzheimer’s and closely linked to memory loss and cognitive decline.
Managing neurotransmitters has often been an angle of research when it comes to brain health, and we’ve written about that before with other neurotransmitters.
For example, with regard to dopamine, there’s a study that found:
- Increasing dopamine activity increased neprilysin levels.
- Higher neprilysin reduced amyloid-β levels.
- Reduced amyloid burden was associated with better memory performance
You can read about that, here: An Accessible New Development Against Alzheimer’s
And when it comes to norephinephrine, there was a study that concluded “β2AR manipulations can alter disease pathology”, which is a great example of how carefully scientists say things, but the series of declarations adds up to the same; we’ll quote some points directly from the paper’s abstract:
- NE inhibits surveillance activity of microglia, the brain’s resident immune cells, via their β2 adrenergic receptors (β2ARs)
- Microglial β2AR signaling is an important modulator of amyloid pathology.
- Endogenous β2AR signaling degenerates as a function of amyloid pathology and aging.
- In AD, microglia downregulate β2AR expression early and progressively.
- β2AR manipulations can alter disease pathology.
- Importantly, dampening microglial β2AR signaling worsened plaque load and the associated neuritic damage, while stimulating microglial β2AR signaling attenuated amyloid pathology.
- Our results suggest that microglial β2AR could be explored as a potential therapeutic target to modify AD pathology.
Translating from sciencese (if you’ll pardon that we’ll still use some big words, but only ones we explain in the below-linked article):
Norepinephrine activates certain receptors in microglia, and those receptors tell the microglia to “keep calm & carry on”. In the case of Alzheimer’s disease, those receptors stop working correctly, leading to increased neuroinflammation. Thus, stimulating those receptors with norepinephrine reduces neuroinflammation, allowing the microglia to calmly carry on with their actual job of getting rid of the amyloid that leads to Alzheimer’s disease.
You read more about that, here: Norepinephrine vs Alzheimer’s Disease
So, what about acetylcholine?
Acetylcholine is the main neurotransmitter of the parasympathetic nervous system, and is also heavily involved in cognitive functions including memory and creative thinking.
In this study we’re sharing today, they found that the compounds from aloe vera demonstrated strong binding affinities of −8.6 kcal/mol with acetylcholinesterase and −8.7 kcal/mol with butyrylcholinesterase.
This is relevant, because if you take an acetylcholinesterase inhibitor, it will inhibit acetylcholinesterase, meaning you will have more acetylcholine to work with. That’s good (for most people most of the time).
You can find the paper itself, here: In silico exploration of Aloe vera leaf compounds as dual AChE and BChE inhibitors for Alzheimer’s disease therapy
So, should you stock up on aloe vera and get juicing?
Probably not just yet, though don’t let us stop you. It’s just, this research is new and needs more testing to be sure of its conclusions, which will doubtlessly be done in non-human animals and then in humans.
In the meantime, here are two ways of improving your choline and/or acetylcholine levels:
Huperzine A: A Natural Nootropic ← it’s an acetylcholinesterase inhibitor
…and:
Citicoline: Better Than Dietary Choline?
Want to learn more?
Here’s a great starting point:
How To Reduce Your Alzheimer’s Risk
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fast Like A Girl – by Dr. Mindy Pelz

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of information out there when it comes to intermittent fasting is very much centered on men in the 25–35 years age range. What about the rest of us?
Our physiological needs are not the same, and it’d be foolhardy to ignore that. But what things do still stand the same, and what things would benefit from a different approach in our cases?
Dr. Pelz has our back with this book packed with information based on the best science currently out there. She gives a general overview of fasting with full consideration to the fact that we the reader may well be female or over a certain age or both. In addition, the book offers:
- Metabolic switching (the “missing key to weight loss”)
- Building a fasting lifestyle (that works with your actual life, not just on paper)
- How to time fasting according to your menstrual cycle (if you don’t have a cycle, she has you covered too)
- How to break a fast—properly (and many other hacks/tips/tricks to make fasting so much easier)
Bottom line: if you want to do intermittent fasting and want to work with rather than against your body, then this book is a fine option.
Share This Post
-

The Brain As A Work-In-Progress
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
And The Brain Goes Marching On!

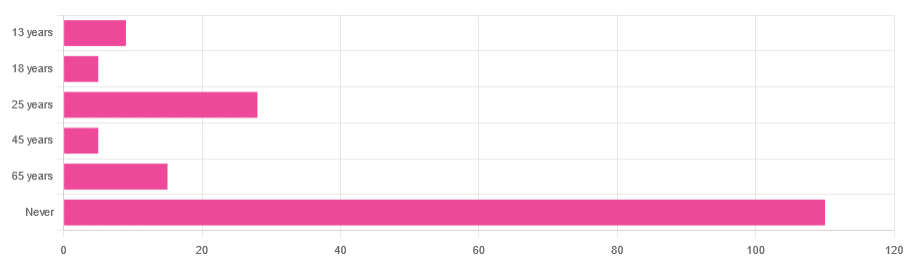
In Tuesday’s newsletter, we asked you “when does the human brain stop developing?” and got the above-depicted, below-described, set of responses:
- About 64% of people said “Never”
- About 16% of people said “25 years”
- About 9% of people said “65 years”
- About 5% of people said “13 years”
- About 3% of people said “18 years”
- About 3% of people said “45 years”
Some thoughts, before we get into the science:
An alternative wording for the original question was “when does the human brain finish developing”; the meaning is the same but the feeling is slightly different:
- “When does the human brain stop developing?” focuses attention on the idea of cessation, and will skew responses to later ages
- When does the human brain finish developing?” focuses on attention on a kind of “is it done yet?” and will skew responses to earlier ages
Ultimately, since we had to chose one word or another, we picked the shortest one, but it would have been interesting if we could have done an A/B test, and asked half one way, and half the other way!
Why we picked those ages
We picked those ages as poll options for reasons people might be drawn to them:
- 13 years: in English-speaking cultures, an important milestone of entering adolescence (note that the concept of a “teenager” is not precisely universal as most languages do not have “-teen” numbers in the same way; the concept of “adolescent” may thus be tied to other milestones)
- 18 years: age of legal majority in N. America and many other places
- 25 years: age popularly believed to be when the brain is finished developing, due to a study that we’ll talk about shortly (we guess that’s why there’s a spike in our results for this, too!)
- 45 years: age where many midlife hormonal changes occur, and many professionals are considered to have peaked in competence and start looking towards retirement
- 65 years: age considered “senior” in much of N. America and many other places, as well as the cut-off and/or starting point for a lot of medical research
Notice, therefore, how a lot of things are coming from places they really shouldn’t. For example, because there are many studies saying “n% of people over 65 get Alzheimer’s” or “n% of people over 65 get age-related cognitive decline”, etc, 65 becomes the age where we start expecting this—because of an arbitrary human choice of where to draw the cut-off for the study enrollment!
Similarly, we may look at common ages of legal majority, or retirement pensions, and assume “well it must be for a good reason”, and dear reader, those reasons are more often economically motivated than they are biologically reasoned.
So, what does the science say?
Our brains are never finished developing: True or False?
True! If we define “finished developing” as “we cease doing neurogenesis and neuroplasticity is no longer in effect”.
Glossary:
- Neurogenesis: the process of creating new brain cells
- Neuroplasticity: the process of the brain adapting to changes by essentially rebuilding itself to suit our perceived current needs
We say “perceived” because sometimes neuroplasticity can do very unhelpful things to us (e.g: psychological trauma, or even just bad habits), but on a biological level, it is always doing its best to serve our overall success as an organism.
For a long time it was thought that we don’t do neurogenesis at all as adults, but this was found to be untrue:
How To Grow New Brain Cells (At Any Age)
Summary of conclusions of the above: we’re all growing new brain cells at every age, even if we be in our 80s and with Alzheimer’s disease, but there are things we can do to enhance our neurogenic potential along the way.
Neuroplasticity will always be somewhat enhanced by neurogenesis (after all, new neurons get given jobs to do), and we reviewed a great book about the marvels of neuroplasticity including in older age:
Our brains are still developing up to the age of 25: True or False?
True! And then it keeps on developing after that, too. Now this is abundantly obvious considering what we just talked about, but see what a difference the phrasing makes? Now it makes it sound like it stops at 25, which this statement doesn’t claim at all—it only speaks for the time up to that age.
A lot of the popular press about “the brain isn’t fully mature until the age of 25” stems from a 2006 study that found:
❝For instance, frontal gray matter volume peaks at about age 11.0 years in girls and 12.1 years in boys, whereas temporal gray matter volume peaks at about age at 16.7 years in girls and 16.2 years in boys. The dorsal lateral prefrontal cortex, important for controlling impulses, is among the latest brain regions to mature without reaching adult dimensions until the early 20s.❞
Source: Structural Magnetic Resonance Imaging of the Adolescent Brain
There are several things to note here:
- The above statement is talking about the physical size of the brain growing
- Nowhere does he say “and stops developing at 25”
However… The study only looked at brains up to the age of 25. After that, they stopped looking, because the study was about “the adolescent brain” so there has to be a cut-off somewhere, and that was the cut-off they chose.
This is the equivalent of saying “it didn’t stop raining until four o’clock” when the reality is that four o’clock is simply when you gave up on checking.
The study didn’t misrepresent this, by the way, but the popular press did!
Another 2012 study looked at various metrics of brain development, and found:
- Synapse overproduction into the teens
- Cortex pruning into the late 20s
- Prefrontal pruning into middle age at least (they stopped looking)
- Myelination beyond middle age (they stopped looking)
Source: Experience and the developing prefrontal cortex ← check out figure 1, and make sure you’re looking at the human data not the rat data
So how’s the most recent research looking?
Here’s a 2022 study that looked at 123,984 brain scans spanning the age range from mid-gestation to 100 postnatal years, and as you can see from its own figure 1… Most (if not all) brain-things keep growing for life, even though most slow down at some point, they don’t stop:
Brain charts for the human lifespan ← check out figure 1; don’t get too excited about the ventricular volume column as that is basically “brain that isn’t being a brain”. Do get excited about the rest, though!
Want to know how not to get caught out by science being misrepresented by the popular press? Check out:
How Science News Outlets Can Lie To You (Yes, Even If They Cite Studies!)
Take care!
Share This Post
-

Should I take vitamin C to ward off colds, lower blood pressure or reduce cancer risk?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Vitamin C is one of the most iconic nutrients in popular health culture, often credited with preventing colds, boosting immunity and even fighting serious diseases.
But while it’s essential for our bodies to function, its benefits are often misunderstood or overstated. Before you stock up on supplements, here’s what to consider.

Sean Anthony Eddy/Getty Images What is vitamin C and why does my body need it?
Vitamin C, also known as ascorbic acid, plays several essential roles in the body.
It is a powerful antioxidant, protecting cells from damage. Vitamin C supports the immune functions of the body, aids in absorption of iron, and is involved in wound healing.
Vitamin C also helps in the synthesis of collagen, which holds together tissues and is a structural component of gums and skin. A severe deficiency of vitamin C leads to a health condition called scurvy, where the body produces insufficient collagen and can’t hold tissue together. Eventually, the gums cannot hold onto teeth and they fall out, and blood vessels break down, causing internal bleeding.
Humans cannot synthesise vitamin C. We must take it in through our diet. Most of our vitamin C comes from vegetables (about 40%), fruits (19%) and from vegetable or fruit juices (29%).
Chemically, the vitamin C in supplements is identical to the vitamin C in food. Your body cannot tell the difference.
Vitamin C in supplements and food are identical. Diana Polekhina/Unsplash What is missing in supplement forms of vitamin C is the fibre, flavonoids, other vitamins, minerals and phytochemicals that come with food, and that may work together with vitamin C.
These other compounds help with absorption, provide complementary antioxidants, and together with vitamin C, provide health benefits that the vitamin by itself does not.
Historically, sailors often had a very limited diet and were often struck down with scurvy. But if you have a balanced diet, you don’t need vitamin C supplements.
What does vitamin C treat and not treat?
Common cold
Vitamin C has been promoted as a way to boost the immune system. It’s widely considered as a way to prevent and treat the common cold and flu.
However, results from a review of all the evidence has shown regular supplementation of 200 mg or more vitamin C does not reduce the incidence of the common cold.
Regular vitamin C supplement does reduce the duration, and at doses greater than 1,000 mg or more, could reduce the severity of common cold symptoms.
When vitamin C is used for treating common colds and only taken at the start of cold symptoms, it does not affect the duration and severity. Some studies have a shown very limited benefit when taken daily before getting sick, but the benefit was very small. Overall, the authors concluded routine supplementation with vitamin C is not worthwhile.
Heart disease and stroke
Research has shown vitamin C supplementation does not change the risk of a range of cardiovascular diseases including heart attack (myocardial infraction), stroke or angina.
One study found vitamin C supplementation at more than 200 mg daily may lower systolic blood pressure (the top number in a reading) by around 4 mmHg and diastolic blood pressure (the lower number) by around 2 mmHg. These are very small changes.
These effects are comparable to regular aerobic exercise and may not be clinically meaningful compared to treatment with conventional medicine, which generally lowers systolic blood pressure by at least 12 mmHg.
Cancer
There are consistent results from multiple studies that show vitamin C supplementation is unable to prevent cancer, including for gastrointestinal, lung, breast, prostate and colorectal cancers.
Is it possible to take too much vitamin C?
The Recommended Daily Intake (RDI) of vitamin C for adults is 45 mg per day. You can get that from a single small glass of orange juice.
The tolerable upper intake level of vitamin C is 2,000 mg daily for adults.
Vitamin C is water-soluble and gets excreted in urine, so the body cannot store it. This means mega-dosing does not provide any benefit, and may in fact cause health problems.
At high doses (above 2,000 mg daily), vitamin C may cause mild to serious side effects. Too much is known to cause diarrhoea, nausea and abdominal cramps. It can also contribute to the formation of kidney stones in men, but not women.
For people who have chronic kidney disease, vitamin C can be especially problematic because vitamin C is flushed from the body by the kidneys. But when the kidneys don’t work properly, it can build up and cause kidney stones.
Should you take a vitamin C supplement?
For most people, a vitamin C tablet is unnecessary. You will get enough from a good balanced diet, from foods such as citrus fruits, berries, tomatoes, capsicum, broccoli and kale.
The evidence doesn’t support claims that vitamin C supplements prevent colds, heart disease or cancer. In fact, the risks may outweigh the benefits.
Nial Wheate, Professor, School of Natural Sciences, Macquarie University; Ian Jamie, Senior Lecturer, School of Natural Sciences, Macquarie University, and Wai-Jo Jocelin Chan, Pharmacist and Lecturer, UNSW Sydney; University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



-
Blackberries vs Cranberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing blackberries to cranberries, we picked the blackberries.
Why?
This one’s not close:
In terms of macros, blackberries have more fiber while cranberries have more carbs, so we give the win to blackberries in this round.
In the category of vitamins, blackberries have a lot more of vitamins A, B1, B2, B3, B7, B9, C, K, and choline, while cranberries have more vitamin B6; another easy win for blackberries.
Looking at minerals, blackberries have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while cranberries have more sodium. Definitely a win for blackberries.
When it comes to other considerations, blackberries also have far more polyphenols, although cranberries have some UTI-fighting properties that are worth mentioning too (but also come with increased risk of kidney stones if you are prone to such). On balance, we’ll call this round a win for blackberries, but your personal circumstances (for example if you are prone to UTIs while also not being prone to kidney stones) could change that.
Adding up the sections makes for a clear overall win for blackberries in any case!
Want to learn more?
You might like:
21 Most Beneficial Polyphenols & What Foods Have Them
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Oral retinoids can harm unborn babies. But many women taking them for acne may not be using contraception
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Oral retinoids are a type of medicine used to treat severe acne. They’re sold under the brand name Roaccutane, among others.
While oral retinoids are very effective, they can have harmful effects if taken during pregnancy. These medicines can cause miscarriages and major congenital abnormalities (harm to unborn babies) including in the brain, heart and face. At least 30% of children exposed to oral retinoids in pregnancy have severe congenital abnormalities.
Neurodevelopmental problems (in learning, reading, social skills, memory and attention) are also common.
Because of these risks, the Australasian College of Dermatologists advises oral retinoids should not be prescribed a month before or during pregnancy under any circumstances. Dermatologists are instructed to make sure a woman isn’t pregnant before starting this treatment, and discuss the risks with women of childbearing age.
But despite this, and warnings on the medicines’ packaging, pregnancies exposed to oral retinoids continue to be reported in Australia and around the world.
In a study published this month, we wanted to find out what proportion of Australian women of reproductive age were taking oral retinoids, and how many of these women were using contraception.
Our results suggest a high proportion of women are not using effective contraception while on these drugs, indicating Australia needs a strategy to reduce the risk oral retinoids pose to unborn babies.
Contraception options
Using birth control to avoid pregnancy during oral retinoid treatment is essential for women who are sexually active. Some contraception methods, however, are more reliable than others.
Long-acting-reversible contraceptives include intrauterine devices (IUDs) inserted into the womb (such as Mirena, Kyleena, or copper devices) and implants under the skin (such as Implanon). These “set and forget” methods are more than 99% effective.
Oral retinoids taken during pregnancy can cause complications in babies. Gorodenkoff/Shutterstock The effectiveness of oral contraceptive pills among “perfect” users (following the directions, with no missed or late pills) is similarly more than 99%. But in typical users, this can fall as low as 91%.
Condoms, when used as the sole method of contraception, have higher failure rates. Their effectiveness can be as low as 82% in typical users.
Oral retinoid use over time
For our study, we analysed medicine dispensing data among women aged 15–44 from Australia’s Pharmaceutical Benefit Scheme (PBS) between 2013 and 2021.
We found the dispensing rate for oral retinoids doubled from one in every 71 women in 2013, to one in every 36 in 2021. The increase occurred across all ages but was most notable in young women.
Most women were not dispensed contraception at the same time they were using the oral retinoids. To be sure we weren’t missing any contraception that was supplied before the oral retinoids, we looked back in the data. For example, for an IUD that lasts five years, we looked back five years before the oral retinoid prescription.
Our analysis showed only one in four women provided oral retinoids were dispensed contraception simultaneously. This was even lower for 15- to 19-year-olds, where only about one in eight women who filled a prescription for oral retinoids were dispensed contraception.
A recent study found 43% of Australian year 10 and 69% of year 12 students are sexually active, so we can’t assume this younger age group largely had no need for contraception.
One limitation of our study is that it may underestimate contraception coverage, because not all contraceptive options are listed on the PBS. Those options not listed include male and female sterilisation, contraceptive rings, condoms, copper IUDs, and certain oral contraceptive pills.
But even if we presume some of the women in our study were using forms of contraception not listed on the PBS, we’re still left with a significant portion without evidence of contraception.
What are the solutions?
Other countries such as the United States and countries in Europe have pregnancy prevention programs for women taking oral retinoids. These programs include contraception requirements, risk acknowledgement forms and regular pregnancy tests. Despite these programs, unintended pregnancies among women using oral retinoids still occur in these countries.
But Australia has no official strategy for preventing pregnancies exposed to oral retinoids. Currently oral retinoids are prescribed by dermatologists, and most contraception is prescribed by GPs. Women therefore need to see two different doctors, which adds costs and burden.
Preventing pregnancy during oral retinoid treatment is essential. Krakenimages.com/Shutterstock Rather than a single fix, there are likely to be multiple solutions to this problem. Some dermatologists may not feel confident discussing sex or contraception with patients, so educating dermatologists about contraception is important. Education for women is equally important.
A clinical pathway is needed for reproductive-aged women to obtain both oral retinoids and effective contraception. Options may include GPs prescribing both medications, or dermatologists only prescribing oral retinoids when there’s a contraception plan already in place.
Some women may initially not be sexually active, but change their sexual behaviour while taking oral retinoids, so constant reminders and education are likely to be required.
Further, contraception access needs to be improved in Australia. Teenagers and young women in particular face barriers to accessing contraception, including costs, stigma and lack of knowledge.
Many doctors and women are doing the right thing. But every woman should have an effective contraception plan in place well before starting oral retinoids. Only if this happens can we reduce unintended pregnancies among women taking these medicines, and thereby reduce the risk of harm to unborn babies.
Dr Laura Gerhardy from NSW Health contributed to this article.
Antonia Shand, Research Fellow, Obstetrician, University of Sydney and Natasha Nassar, Professor of Paediatric and Perinatal Epidemiology and Chair in Translational Childhood Medicine, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Dr. Patrick Walsh’s Guide to Surviving Prostate Cancer – by Dr. Patrick Walsh & Janet Farrar Worthington
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Prostate cancer is not glamorous or fun, and neither is this book.
Nevertheless, it’s a disease that affects 12% of men in general, and 60% of men aged 60+, with that percentage climbing every year after that.
So, if you have a prostate or love someone who has one, this book is worthwhile reading—yes, even as a preventative.
Like many cancers, prostate cancer is easy to treat if caught very early, becomes harder to treat as it goes, and almost impossible to cure if it gets as far as metastasis (i.e., it spread). Like all cancers, it’s better off avoided entirely if possible.
This book covers all the stages:
- How to avoid it
- How to check for it
- How to “nip it in the bud”
- Why some might want to delay treatment (!)
- What options are available afterwards
This latter is quite extensive, and covers not just surgery, but radiation, thermo- or cryoablation, and hormone therapy.
And as for surgery, not just “remove the tumor”, but other options like radical prostatectomy, and even orchiectomy. Not many men will choose to have their testicles removed to stop them from feeding the prostate, but the point is that this book is comprehensive.
It’s asking whenever possible “is there another option?” and exploring all options, with information and without judgment, at each stage.
The writing style (likely co-author Worthington’s influence; she is an award-winning science-writer) is very “for the layman”, and that’s really helpful in demystifying a lot of what can be quite opaque in the field of oncology.
Bottom line: absolutely not an enjoyable read, but a potentially lifesaving one, especially given the odds we mentioned up top.
Click here to check out Dr. Patrick Walsh’s Guide To Surviving Prostate Cancer, and be prepared!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: