Shedding Some Obesity Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s shed some obesity myths!
There are a lot of myths and misconceptions surrounding obesity… And then there are also reactive opposite myths and misconceptions, which can sometimes be just as harmful!
To tackle them all would take a book, but in classic 10almonds style, we’re going to put a spotlight on some of the ones that might make the biggest difference:
True or False: Obesity is genetically pre-determined
False… With caveats.
Some interesting results have been found from twin studies and adoption studies, showing that genes definitely play some role, but lifestyle is—for most people—the biggest factor:
- The body-mass index of twins who have been reared apart
- An adoption study of human obesity
- Using a sibling-adoption design to parse genetic and environmental influences on children’s body mass index
In short: genes predispose; they don’t predetermine. But that predisposition alone can make quite a big difference, if it in turn leads to different lifestyle factors.
But upon seeing those papers centering BMI, let’s consider…
True or False: BMI is a good, accurate measure of health in the context of bodyweight
False… Unless you’re a very large group of thin white men of moderate height, which was the demographic the system was built around.
Bonus information: it was never intended to be used to measure the weight-related health of any individual (not even an individual thin white man of moderate height), but rather, as a tool to look at large-scale demographic trends.
Basically, as a system, it’s being used in a way it was never made for, and the results of that misappropriation of an epidemiological tool for individual health are predictably unhelpful.
To do a deep-dive into all the flaws of the BMI system, which are many, we’d need to devote a whole main feature just to that.
Update: we have now done so!
Here it is: When BMI Doesn’t Measure Up
True or False: Obesity does not meaningfully impact more general health
False… In more ways than one (but there are caveats)
Obesity is highly correlated with increased risk of all-cause mortality, and weight loss, correspondingly, correlates with a reduced risk. See for example:
So what are the caveats?
Let’s put it this way: owning a horse is highly correlated with increased healthy longevity. And while owning a horse may come with some exercise and relaxation (both of which are good for the health), it’s probably mostly not the horse itself that conveys the health benefits… it’s that someone who has the resources to look after a horse, probably has the resources to look after their own health too.
So sometimes there can be a reason for a correlation (it’s not a coincidence!) but the causative factor is partially (or in some cases, entirely) something else.
So how could this play out with obesity?
There’s a lot of discrimination in healthcare settings, unfortunately! In this case, it often happens that a thin person goes in with a medical problem and gets treated for that, while a fat person can go in with the same medical problem and be told “you should try losing some weight”.
Top tip if this happens to you… Ask: “what would you advise/prescribe to a thin person with my same symptoms?”
Other things may be more systemic, for example:
When a thin person goes to get their blood pressure taken, and that goes smoothly, while a fat person goes to get their blood pressure taken, and there’s not a blood pressure cuff to fit them, is the problem the size of the person or the size of the cuff? It all depends on perspective, in a world built around thin people.
That’s a trivial-seeming example, but the same principle has far-reaching (and harmful) implications in healthcare in general, e.g:
- Surgeons being untrained (and/or unwilling) to operate on fat people
- Getting a one-size-fits-all dose that was calculated using average weight, and now doesn’t work
- MRI machines are famously claustrophobia-inducing for thin people; now try not fitting in it in the first place
…and so forth. So oftentimes, obesity will be correlated with a poor healthcare outcome, where the problem is not actually the obesity itself, but rather the system having been set up with thin people in mind.
It would be like saying “Having O- blood type results in higher risks when receiving blood transfusions”, while omitting to add “…because we didn’t stock O- blood”.
True or False: to reduce obesity, just eat less and move more!
False… Mostly.
Moving more is almost always good for most people. When it comes to diet, quality is much more important than quantity. But these factors alone are only part of the picture!
But beyond diet and exercise, there are many other implicated factors in weight gain, weight maintenance, and weight loss, including but not limited to:
- Disrupted sleep
- Chronic stress
- Chronic pain
- Hormonal imbalances
- Physical disabilities that preclude a lot of exercise
- Mental health issues that add (and compound) extra levels of challenge
- Medications that throw all kinds of spanners into the works with their side effects
…and even just those first two things, diet and exercise, are not always so correlated to weight as one might think—studies have found that the difference for exercise especially is often marginal:
Read: Widespread misconceptions about obesity ← academic article in the Journal of the College of Family Physicians of Canada
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Hearing voices is common and can be distressing. Virtual reality might help us meet and ‘treat’ them

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have you ever heard something that others cannot – such as your name being called? Hearing voices or other noises that aren’t there is very common. About 10% of people report experiencing auditory hallucinations at some point in their life.
The experience of hearing voices can be very different from person to person, and can change over time. They might be the voice of someone familiar or unknown. There might be many voices, or just one or two. They can be loud or quiet like a whisper.
For some people these experiences are positive. They might represent a spiritual or supernatural experience they welcome or a comforting presence. But for others these experiences are distressing. Voices can be intrusive, negative, critical or threatening. Difficult voices can make a person feel worried, frightened, embarrassed or frustrated. They can also make it hard to concentrate, be around other people and get in the way of day-to-day activities.
Although not everyone who hears voices has a mental health problem, these experiences are much more common in people who do. They have been considered a hallmark symptom of schizophrenia, which affects about 24 million people worldwide.
However, such experiences are also common in other mental health problems, particularly in mood- and trauma-related disorders (such as bipolar disorder or depression and post-traumatic stress disorder) where as many as half of people may experience them.

Rawpixel/Shutterstock Why do people hear voices?
It is unclear exactly why people hear voices but exposure to prolonged stress, trauma or depression can increase the chances.
Some research suggests people who hear voices might have brains that are “wired” differently, particularly between the hearing and speaking parts of the brain. This may mean parts of our inner speech can be experienced as external voices. So, having the thought “you are useless” when something goes wrong might be experienced as an external person speaking the words.
Other research suggests it may relate to how our brains use past experiences as a template to make sense of and make predictions about the world. Sometimes those templates can be so strong they lead to errors in how we experience what is going on around us, including hearing things our brain is “expecting” rather than what is really happening.
What is clear is that when people tell us they are hearing voices, they really are! Their brain perceives voice experiences as if someone were talking in the room. We could think of this “mistake” as working a bit like being susceptible to common optical tricks or visual illusions.
There may be differences in the brains of people who hear voices. Triff/Shutterstock Coping with hearing voices
When hearing voices is getting in the way of life, treatment guidelines recommend the use of medications. But roughly a third of people will experience ongoing distress. As such, treatment guidelines also recommend the use of psychological therapies such as cognitive behavioural therapy.
The next generation of psychological therapies are beginning to use digital technologies and virtual reality offers a promising new medium.
Avatar therapy allows a person to create a virtual representation of the voice or voices, which looks and sounds like what they are experiencing. This can help people regain power in the “relationship” as they interact with the voice character, supported by a therapist.
Jason’s experience
Aged 53, Jason (not his real name) had struggled with persistent voices since his early 20s. Antipsychotic medication had helped him to some extent over the years, but he was still living with distressing voices. Jason tried out avatar therapy as part of a research trial.
He was initially unable to stand up to the voices, but he slowly gained confidence and tested out different ways of responding to the avatar and voices with his therapist’s support.
Jason became more able to set boundaries, such as not listening to them for periods throughout the day. He also felt more able to challenge what they said and make his own choices.
Over a couple of months, Jason started to experience some breaks from the voices each day and his relationship with them started to change. They were no longer like bullies, but more like critical friends pointing out things he could consider or be aware of.
A screenshot from HekaVR, the software used in the Australian AMETHYST trial. HekaVR, CC BY-ND Gaining recognition
Following promising results overseas and its recommendation by the United Kingdom’s National Institute for Health and Care Excellence, our team has begun adapting the therapy for an Australian context.
We are trialling delivering avatar therapy from our specialist voices clinic via telehealth. We are also testing whether avatar therapy is more effective than the current standard therapy for hearing voices, based on cognitive behavioural therapy.
As only a minority of people with psychosis receive specialist psychological therapy for hearing voices, we hope our trial will support scaling up these new treatments to be available more routinely across the country.
We would like to acknowledge the advice and input of Dr Nadine Keen (consultant clinical psychologist at South London and Maudsley NHS Foundation Trust, UK) on this article.
Leila Jameel, Trial Co-ordinator and Research Therapist, Swinburne University of Technology; Imogen Bell, Senior Research Fellow and Psychologist, The University of Melbourne; Neil Thomas, Professor of Clinical Psychology, Swinburne University of Technology, and Rachel Brand, Senior Lecturer in Clinical Psychology, University of the Sunshine Coast
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Which Sugars Are Healthier, And Which Are Just The Same?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From Apples to Bees, and High-Fructose Cs

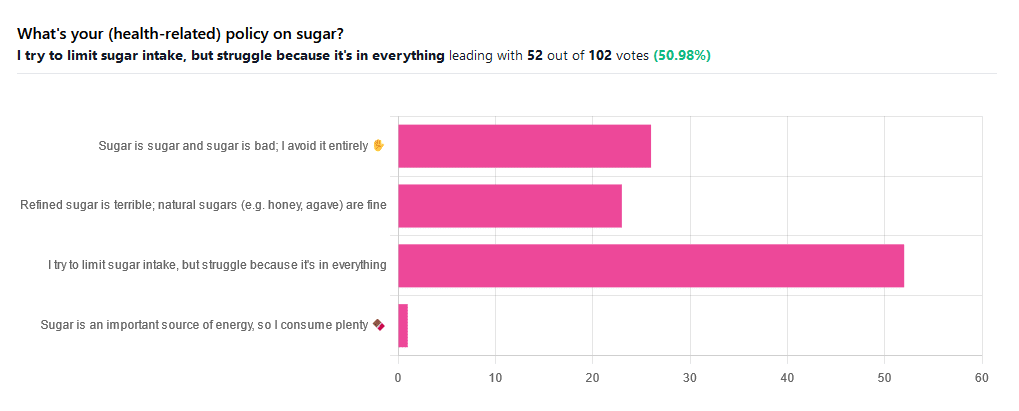
We asked you for your (health-related) policy on sugar. The trends were as follows:
- About half of all respondents voted for “I try to limit sugar intake, but struggle because it’s in everything”
- About a quarter of all respondents voted for “Refined sugar is terrible; natural sugars (e.g. honey, agave) are fine”
- About a quarter of all respondents voted for “Sugar is sugar and sugar is bad; I avoid it entirely”
- One (1) respondent voted for “Sugar is an important source of energy, so I consume plenty”
Writer’s note: I always forget to vote in these, but I’d have voted for “I try to limit sugar intake, but struggle because it’s in everything”.
Sometimes I would like to make my own [whatever] to not have the sugar, but it takes so much more time, and often money too.
So while I make most things from scratch (and typically spend about an hour cooking each day), sometimes store-bought is the regretfully practical timesaver/moneysaver (especially when it comes to condiments).
So, where does the science stand?
There has, of course, been a lot of research into the health impact of sugar.
Unfortunately, a lot of it has been funded by sugar companies, which has not helped. Conversely, there are also studies funded by other institutions with other agendas to push, and some of them will seek to make sugar out to be worse than it is.
So for today’s mythbusting overview, we’ve done our best to quality-control studies for not having financial conflicts of interest. And of course, the usual considerations of favoring high quality studies where possible Large sample sizes, good method, human subjects, that sort of thing.
Sugar is sugar and sugar is bad: True or False?
False and True, respectively.
- Sucrose is sucrose, and is generally bad.
- Fructose is fructose, and is worse.
Both ultimately get converted into glycogen (if not used immediately for energy), but for fructose, this happens mostly* in the liver, which a) taxes it b) goes very unregulated by the pancreas, causing potentially dangerous blood sugar spikes.
This has several interesting effects:
- Because fructose doesn’t directly affect insulin levels, it doesn’t cause insulin insensitivity (yay)
- Because fructose doesn’t directly affect insulin levels, this leaves hyperglycemia untreated (oh dear)
- Because fructose is metabolized by the liver and converted to glycogen which is stored there, it’s one of the main contributors to non-alcoholic fatty liver disease (at this point, we’re retracting our “yay”)
Read more: Fructose and sugar: a major mediator of non-alcoholic fatty liver disease
*”Mostly” in the liver being about 80% in the liver. The remaining 20%ish is processed by the kidneys, where it contributes to kidney stones instead. So, still not fabulous.
Fructose is very bad, so we shouldn’t eat too much fruit: True or False?
False! Fruit is really not the bad guy here. Fruit is good for you!
Fruit does contain fructose yes, but not actually that much in the grand scheme of things, and moreover, fruit contains (unless you have done something unnatural to it) plenty of fiber, which mitigates the impact of the fructose.
- A medium-sized apple (one of the most sugary fruits there is) might contain around 11g of fructose
- A tablespoon of high-fructose corn syrup can have about 27g of fructose (plus about 3g glucose)
Read more about it: Effects of high-fructose (90%) corn syrup on plasma glucose, insulin, and C-peptide in non-insulin-dependent diabetes mellitus and normal subjects
However! The fiber content (in fruit) mitigates the impact of the fructose almost entirely anyway.
And if you take fruits that are high in sugar and/but high in polyphenols, like berries, they now have a considerable net positive impact on glycemic health:
- Polyphenols and Glycemic Control
- Polyphenols and their effects on diabetes management: A review
- Dietary polyphenols as antidiabetic agents: Advances and opportunities
You may be wondering: what was that about “unless you have done something unnatural to it”?
That’s mostly about juicing. Juicing removes much (or all) of the fiber, and if you do that, you’re basically back to shooting fructose into your veins:
- Effect of Fruit Juice on Glucose Control and Insulin Sensitivity in Adults: A Meta-Analysis of 12 Randomized Controlled Trials
- Intake of Fruit, Vegetables, and Fruit Juices and Risk of Diabetes in Women
Natural sugars like honey, agave, and maple syrup, are healthier than refined sugars: True or False?
True… Sometimes, and sometimes marginally.
This is partly because of the glycemic index and glycemic load. The glycemic index scores tail off thus:
- table sugar = 65
- maple syrup = 54
- honey = 46
- agave syrup = 15
So, that’s a big difference there between agave syrup and maple syrup, for example… But it might not matter if you’re using a very small amount, which means it may have a high glycemic index but a low glycemic load.
Note, incidentally, that table sugar, sucrose, is a disaccharide, and is 50% glucose and 50% fructose.
The other more marginal health benefits come from that fact that natural sugars are usually found in foods high in other nutrients. Maple syrup is very high in manganese, for example, and also a fair source of other minerals.
But… Because of its GI, you really don’t want to be relying on it for your nutrients.
Wait, why is sugar bad again?
We’ve been covering mostly the more “mythbusting” aspects of different forms of sugar, rather than the less controversial harms it does, but let’s give at least a cursory nod to the health risks of sugar overall:
- Obesity and associated metabolic risk
- Main contributor to non-alcoholic fatty liver disease
- Increased risk of heart disease
- Insulin resistance and diabetes risk
- Cellular aging (shortened telomeres)
- 95% increased cancer risk
That last one, by the way, was a huge systematic review of 37 large longitudinal cohort studies. Results varied depending on what, specifically, was being examined (e.g. total sugar, fructose content, sugary beverages, etc), and gave up to 200% increased cancer risk in some studies on sugary beverages, but 95% increased risk is a respectable example figure to cite here, pertaining to added sugars in foods.
And finally…
The 56 Most Common Names for Sugar (Some Are Tricky)
How many did you know?
Share This Post
-

Can We Do Fat Redistribution?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The famous answer: no
The truthful answer: yes, and we are doing it all the time whether we want to or not, so we might as well know what things affect our fat distribution in various body parts.
There’s a kernel of truth in the “no”, though, and where that comes from is that we cannot exclusively put fat on in a certain area only, and nor can we do “spot reduction”, i.e., intentionally lose fat from only one place.
How, then, do we do fat redistribution?
Your body is a living organism, not a statue
It’s easy to think “I’ve been carrying this fat in this place for 20 years”, but during that time the fat has been replaced several times and moved often; in fact, the cells containing the fat have even been replaced. Because: fat can seem like a substance that’s alien to your body because it doesn’t respond like muscles, isn’t controllable like muscles, doesn’t have the same sensibility as muscles, etc. But, every bit of fat stored in your body is stored inside a fat cell; it’s not one big unit of fat; it’s lots of tiny ones.
In reality, any given bit of fat on your body has probably been there for 18–24 months at most:
Fat turnover in obese slower than average
…and there are assorted factors that can modify the rate at which our body deals with fat storage:
Human white adipose tissue: A highly dynamic metabolic organ
So, how do I get rid of this tummy?
There are plenty of stories of people who try to lose weight from one part of their body, and lose it from somewhere else instead. Say, a person wants to lose weight from her hips, and with careful diet and exercise, she loses weight—by dropping a couple of bra cup sizes while keeping the hips.
So, we must figure out: why is fat stored in certain places? And the main driving factors are:
- hormones
- metabolic health
- stress
Hormones affect fat distribution insofar as estrogen and progesterone will favor the hips, thighs, butt, breasts, and testosterone will favor a more central (but still subcutaneous, not visceral) distribution. Additionally, estrogen and progesterone will favor a higher body fat percentage, while testosterone will favor a lower one.
This is particularly relevant later in life, when suddenly the hormone(s) you’ve been relying on to keep your shape, are now declining, meaning your shape does too. This goes for everyone regardless of sex.
See:
- What You Should Have Been Told About The Menopause Beforehand
- The BAT-pause! ← this is about the conversion of white adipose tissue to brown adipose tissue, and how estrogen helps this happen
- Topping Up Testosterone?
Metabolic health affects fat distribution insofar as poor metabolic health will result in more fat being stored in the viscera, rather than in the usual subcutaneous places. This is a serious health risk.
See: Visceral Belly Fat & How To Lose It
Stress affects fat distribution insofar as chronically elevated cortisol levels see more fat sent to the stomach, face, and neck. This fat redistribution isn’t dangerous itself, but it can be indicative of the chronic stress, which does pose more of a general threat to health.
See: Lower Your Cortisol! (Here’s Why & How)
What this means in practical terms
Assuming that you would like the fat distribution that says “this is a healthy woman” or “this is a healthy man”, respectively, then you might want to:
- Check your sex hormone levels and get them adjusted if appropriate
- Improve your overall metabolic health—without necessarily trying to lose weight, just, take care of your blood sugars for example, and they will take care of you in terms of fat storage.
- Manage your stress (which includes any stress you are experiencing about your body not being how you’d like it to be).
If you are doing these things, and you don’t have any major untreated medical abnormalities that affect these things, then your fat will go to the places generally considered healthiest.
Can we speed it up?
Yes, we can! Firstly, we can speed up our overall metabolism:
Let’s Burn! Metabolic Tweaks And Hacks
Secondly, we can encourage our body to “move” fat by intentionally “yo-yoing”, something usually considered bad in dieting when people just want to lose weight and instead are going up and down, but: if you lose weight healthily, it comes off everywhere evenly, and if you gain weight healthily, it goes mostly to the places where it should be.
So, a sequence of lose-gain-lose-gain might look like “lose a bit from everywhere, put it back in the good place, lose a bit more from everywhere, put it back in the good place”, etc.
So, you might want to gently cycle these a few months apart, for example:
How To Lose Fat (Healthily!) | How To Gain Fat (Healthily!)
You can also cheat a little, if it suits your purpose! By this we mean: if you’d like a little extra where you already have a little fat, then you can put muscle on underneath it, it will pad it up, and (because of the layer of actual fat on top) nobody will know the difference unless you flex it with their hand on it.
Let’s put it this way: people doing squats for a bubble-butt aren’t doing it to put on fat; they’re putting muscle on under the fat they have.
So, check out: How To Gain Muscle (Healthily!)
And finally, for all your body-sculpting needs, we present these excellent books:
Women’s Strength Training Anatomy Workouts – by Frédéric Delavier
Strength Training Anatomy (For Men) – by Frédéric Delavier
Enjoy!
Share This Post




Related Posts
-

4 Ways Vaccine Skeptics Mislead You on Measles and More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Measles is on the rise in the United States. In the first quarter of this year, the number of cases was about 17 times what it was, on average, during the same period in each of the four years before, according to the Centers for Disease Control and Prevention. Half of the people infected — mainly children — have been hospitalized.
It’s going to get worse, largely because a growing number of parents are deciding not to get their children vaccinated against measles as well as diseases like polio and pertussis. Unvaccinated people, or those whose immunization status is unknown, account for 80% of the measles cases this year. Many parents have been influenced by a flood of misinformation spouted by politicians, podcast hosts, and influential figures on television and social media. These personalities repeat decades-old notions that erode confidence in the established science backing routine childhood vaccines. KFF Health News examined the rhetoric and explains why it’s misguided:
The No-Big-Deal Trope
A common distortion is that vaccines aren’t necessary because the diseases they prevent are not very dangerous, or too rare to be of concern. Cynics accuse public health officials and the media of fear-mongering about measles even as 19 states report cases.
For example, an article posted on the website of the National Vaccine Information Center — a regular source of vaccine misinformation — argued that a resurgence in concern about the disease “is ‘sky is falling’ hype.” It went on to call measles, mumps, chicken pox, and influenza “politically incorrect to get.”
Measles kills roughly 2 of every 1,000 children infected, according to the CDC. If that seems like a bearable risk, it’s worth pointing out that a far larger portion of children with measles will require hospitalization for pneumonia and other serious complications. For every 10 measles cases, one child with the disease develops an ear infection that can lead to permanent hearing loss. Another strange effect is that the measles virus can destroy a person’s existing immunity, meaning they’ll have a harder time recovering from influenza and other common ailments.
Measles vaccines have averted the deaths of about 94 million people, mainly children, over the past 50 years, according to an April analysis led by the World Health Organization. Together with immunizations against polio and other diseases, vaccines have saved an estimated 154 million lives globally.
Some skeptics argue that vaccine-preventable diseases are no longer a threat because they’ve become relatively rare in the U.S. (True — due to vaccination.) This reasoning led Florida’s surgeon general, Joseph Ladapo, to tell parents that they could send their unvaccinated children to school amid a measles outbreak in February. “You look at the headlines and you’d think the sky was falling,” Ladapo said on a News Nation newscast. “There’s a lot of immunity.”
As this lax attitude persuades parents to decline vaccination, the protective group immunity will drop, and outbreaks will grow larger and faster. A rapid measles outbreak hit an undervaccinated population in Samoa in 2019, killing 83 people within four months. A chronic lack of measles vaccination in the Democratic Republic of the Congo led to more than 5,600 people dying from the disease in massive outbreaks last year.
The ‘You Never Know’ Trope
Since the earliest days of vaccines, a contingent of the public has considered them bad because they’re unnatural, as compared with nature’s bounty of infections and plagues. “Bad” has been redefined over the decades. In the 1800s, vaccine skeptics claimed that smallpox vaccines caused people to sprout horns and behave like beasts. More recently, they blame vaccines for ailments ranging from attention-deficit/hyperactivity disorder to autism to immune system disruption. Studies don’t back the assertions. However, skeptics argue that their claims remain valid because vaccines haven’t been adequately tested.
In fact, vaccines are among the most studied medical interventions. Over the past century, massive studies and clinical trials have tested vaccines during their development and after their widespread use. More than 12,000 people took part in clinical trials of the most recent vaccine approved to prevent measles, mumps, and rubella. Such large numbers allow researchers to detect rare risks, which are a major concern because vaccines are given to millions of healthy people.
To assess long-term risks, researchers sift through reams of data for signals of harm. For example, a Danish group analyzed a database of more than 657,000 children and found that those who had been vaccinated against measles as babies were no more likely to later be diagnosed with autism than those who were not vaccinated. In another study, researchers analyzed records from 805,000 children born from 1990 through 2001 and found no evidence to back a concern that multiple vaccinations might impair children’s immune systems.
Nonetheless, people who push vaccine misinformation, like candidate Robert F. Kennedy Jr., dismiss massive, scientifically vetted studies. For example, Kennedy argues that clinical trials of new vaccines are unreliable because vaccinated kids aren’t compared with a placebo group that gets saline solution or another substance with no effect. Instead, many modern trials compare updated vaccines with older ones. That’s because it’s unethical to endanger children by giving them a sham vaccine when the protective effect of immunization is known. In a 1950s clinical trial of polio vaccines, 16 children in the placebo group died of polio and 34 were paralyzed, said Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia and author of a book on the first polio vaccine.
The Too-Much-Too-Soon Trope
Several bestselling vaccine books on Amazon promote the risky idea that parents should skip or delay their children’s vaccines. “All vaccines on the CDC’s schedule may not be right for all children at all times,” writes Paul Thomas in his bestselling book “The Vaccine-Friendly Plan.” He backs up this conviction by saying that children who have followed “my protocol are among the healthiest in the world.”
Since the book was published, Thomas’ medical license was temporarily suspended in Oregon and Washington. The Oregon Medical Board documented how Thomas persuaded parents to skip vaccines recommended by the CDC, and reported that he “reduced to tears” a mother who disagreed. Several children in his care came down with pertussis and rotavirus, diseases easily prevented by vaccines, wrote the board. Thomas recommended fish oil supplements and homeopathy to an unvaccinated child with a deep scalp laceration, rather than an emergency tetanus vaccine. The boy developed severe tetanus, landing in the hospital for nearly two months, where he required intubation, a tracheotomy, and a feeding tube to survive.
The vaccination schedule recommended by the CDC has been tailored to protect children at their most vulnerable points in life and minimize side effects. The combination measles, mumps, and rubella vaccine isn’t given for the first year of a baby’s life because antibodies temporarily passed on from their mother can interfere with the immune response. And because some babies don’t generate a strong response to that first dose, the CDC recommends a second one around the time a child enters kindergarten because measles and other viruses spread rapidly in group settings.
Delaying MMR doses much longer may be unwise because data suggests that children vaccinated at 10 or older have a higher chance of adverse reactions, such as a seizure or fatigue.
Around a dozen other vaccines have discrete timelines, with overlapping windows for the best response. Studies have shown that MMR vaccines may be given safely and effectively in combination with other vaccines.
’They Don’t Want You to Know’ Trope
Kennedy compares the Florida surgeon general to Galileo in the introduction to Ladapo’s new book on transcending fear in public health. Just as the Roman Catholic inquisition punished the renowned astronomer for promoting theories about the universe, Kennedy suggests that scientific institutions oppress dissenting voices on vaccines for nefarious reasons.
“The persecution of scientists and doctors who dare to challenge contemporary orthodoxies is not a new phenomenon,” Kennedy writes. His running mate, lawyer Nicole Shanahan, has campaigned on the idea that conversations about vaccine harms are censored and the CDC and other federal agencies hide data due to corporate influence.
Claims like “they don’t want you to know” aren’t new among the anti-vaccine set, even though the movement has long had an outsize voice. The most listened-to podcast in the U.S., “The Joe Rogan Experience,” regularly features guests who cast doubt on scientific consensus. Last year on the show, Kennedy repeated the debunked claim that vaccines cause autism.
Far from ignoring that concern, epidemiologists have taken it seriously. They have conducted more than a dozen studies searching for a link between vaccines and autism, and repeatedly found none. “We have conclusively disproven the theory that vaccines are connected to autism,” said Gideon Meyerowitz-Katz, an epidemiologist at the University of Wollongong in Australia. “So, the public health establishment tends to shut those conversations down quickly.”
Federal agencies are transparent about seizures, arm pain, and other reactions that vaccines can cause. And the government has a program to compensate individuals whose injuries are scientifically determined to result from them. Around 1 to 3.5 out of every million doses of the measles, mumps, and rubella vaccine can cause a life-threatening allergic reaction; a person’s lifetime risk of death by lightning is estimated to be as much as four times as high.
“The most convincing thing I can say is that my daughter has all her vaccines and that every pediatrician and public health person I know has vaccinated their kids,” Meyerowitz-Katz said. “No one would do that if they thought there were serious risks.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Needle Pain Is a Big Problem for Kids. One California Doctor Has a Plan.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Almost all new parents go through it: the distress of hearing their child scream at the doctor’s office. They endure the emotional torture of having to hold their child down as the clinician sticks them with one vaccine after another.
“The first shots he got, I probably cried more than he did,” said Remy Anthes, who was pushing her 6-month-old son, Dorian, back and forth in his stroller in Oakland, California.
“The look in her eyes, it’s hard to take,” said Jill Lovitt, recalling how her infant daughter Jenna reacted to some recent vaccines. “Like, ‘What are you letting them do to me? Why?’”
Some children remember the needle pain and quickly start to internalize the fear. That’s the fear Julia Cramer witnessed when her 3-year-old daughter, Maya, had to get blood drawn for an allergy test at age 2.
“After that, she had a fear of blue gloves,” Cramer said. “I went to the grocery store and she saw someone wearing blue gloves, stocking the vegetables, and she started freaking out and crying.”
Pain management research suggests that needle pokes may be children’s biggest source of pain in the health care system. The problem isn’t confined to childhood vaccinations either. Studies looking at sources of pediatric pain have included children who are being treated for serious illness, have undergone heart surgeries or bone marrow transplants, or have landed in the emergency room.
“This is so bad that many children and many parents decide not to continue the treatment,” said Stefan Friedrichsdorf, a specialist at the University of California-San Francisco’s Stad Center for Pediatric Pain, speaking at the End Well conference in Los Angeles in November.
The distress of needle pain can follow children as they grow and interfere with important preventive care. It is estimated that a quarter of all adults have a fear of needles that began in childhood. Sixteen percent of adults refuse flu vaccinations because of a fear of needles.
Friedrichsdorf said it doesn’t have to be this bad. “This is not rocket science,” he said.
He outlined simple steps that clinicians and parents can follow:
- Apply an over-the-counter lidocaine, which is a numbing cream, 30 minutes before a shot.
- Breastfeed babies, or give them a pacifier dipped in sugar water, to comfort them while they’re getting a shot.
- Use distractions like teddy bears, pinwheels, or bubbles to divert attention away from the needle.
- Don’t pin kids down on an exam table. Parents should hold children in their laps instead.
At Children’s Minnesota, Friedrichsdorf practiced the “Children’s Comfort Promise.” Now he and other health care providers are rolling out these new protocols for children at UCSF Benioff Children’s Hospitals in San Francisco and Oakland. He’s calling it the “Ouchless Jab Challenge.”
If a child at UCSF needs to get poked for a blood draw, a vaccine, or an IV treatment, Friedrichsdorf promises, the clinicians will do everything possible to follow these pain management steps.
“Every child, every time,” he said.
It seems unlikely that the ouchless effort will make a dent in vaccine hesitancy and refusal driven by the anti-vaccine movement, since the beliefs that drive it are often rooted in conspiracies and deeply held. But that isn’t necessarily Friedrichsdorf’s goal. He hopes that making routine health care less painful can help sway parents who may be hesitant to get their children vaccinated because of how hard it is to see them in pain. In turn, children who grow into adults without a fear of needles might be more likely to get preventive care, including their yearly flu shot.
In general, the onus will likely be on parents to take a leading role in demanding these measures at medical centers, Friedrichsdorf said, because the tolerance and acceptance of children’s pain is so entrenched among clinicians.
Diane Meier, a palliative care specialist at Mount Sinai, agrees. She said this tolerance is a major problem, stemming from how doctors are usually trained.
“We are taught to see pain as an unfortunate, but inevitable side effect of good treatment,” Meier said. “We learn to repress that feeling of distress at the pain we are causing because otherwise we can’t do our jobs.”
During her medical training, Meier had to hold children down for procedures, which she described as torture for them and for her. It drove her out of pediatrics. She went into geriatrics instead and later helped lead the modern movement to promote palliative care in medicine, which became an accredited specialty in the United States only in 2006.
Meier said she thinks the campaign to reduce needle pain and anxiety should be applied to everyone, not just to children.
“People with dementia have no idea why human beings are approaching them to stick needles in them,” she said. And the experience can be painful and distressing.
Friedrichsdorf’s techniques would likely work with dementia patients, too, she said. Numbing cream, distraction, something sweet in the mouth, and perhaps music from the patient’s youth that they remember and can sing along to.
“It’s worthy of study and it’s worthy of serious attention,” Meier said.
This article is from a partnership that includes KQED, NPR, and KFF Health News.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What Your Mucus Says About Your Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s not a sexy topic (unless perhaps you have a fetish), but it is a useful topic to know about.
So, let’s get down to business with this much-maligned bodily fluid:
What is mucus? And why?
Sometimes, it can seem that mucus only exists to be an inconvenience, and to convey disease.
And… Actually, that’s mostly true.
While some kinds of mucus have other jobs beyond the scope of today’s article (did you know semen is mostly mucus? If not, now you do), the primary job of most of our mucus is to stop things (especially pathogens) going where they shouldn’t.
So, in essence, it really does exist to be an inconvenience—to pathogens. And to convey those pathogens to where they can be disposed of safely, either outside of the body, or to be an easy meal (what with being stuck in mucus, and thus at least moderately immobilized) for our various active immune cells. To make matters worse for the pathogens, there are (usually) enzymes in our mucus that have antimicrobial properties, too.
Some of mucus’s protective role can be in other ways too, such as by lining our stomach. You know, the stomach that contains the acid that can dissolve meat, despite us also being made of meat.
The slimiest rainbow
Ok, maybe not the slimiest rainbow—there’s probably a YouTube slime channel producing more colors. But, our noses are capable of dispensing astonishing quantities of mucus sometimes, and the color can vary widely, so here’s what we can know from that:
Clear
This is as it should be, in good health. If you’re getting lots of it but it’s clear, then it’s usually allergies, but watch out in case it changes color, heralding an infection. This “clear is how it looks when in ideal health”, by the way, is why when someone is sobbing in abject grief, any mucus that shows up to add to that picture will generally be clear.
White
As above, but now inflamed. Inflammation is usually something we don’t want, but in the case of a threat from a pathogen, we actually do want acute inflammation like this—the body is assembling its armies, of which, the most visible (when they appear in mass) are white blood cells. Because of their abundant presence at this stage, the mucus will also become thicker.
Yellow
As above, but the battle is now truly underway, and the yellow color comes from dead white blood cells. This does not, however, mean the battle is necessarily going badly—the body treats its white blood cells as very disposable fighters, and their deaths in large numbers are expected and normal when doing battle.
Green
As above, but neutrophils (a specific kind of white blood cell) have joined the party. They release an enzyme that colors the mucus green—and kills a lot of pathogens. Popular lore says that green mucus means a bacterial infection, but it’s not always so; these can be deployed against viruses too, depending on various factors beyond the scope of this article (but generally pertaining to severity). In any case, this too does not mean the battle is necessarily going badly, but it does express that your body is taking it very seriously—and you should, too.
Red
Nothing to do with infections, usually—it’s just a little blood (the red kind, this time). Usually it got into the mucus because the mucus membrane got damaged, usually due to some kind of physical trauma (e.g. very vigorous nose-blowing, poking things up the nose, etc) or sometimes if the air is very dry (then the mucus itself can dry out, and become stabby inside the nose; when more mucus is produced, it gets infused with blood from the injury).
Pink
As above, but combined with the “white” stage of infection response.
Orange
As above, but combined with the “yellow” stage of infection response.
Brown
As above, but the blood has oxidized—or, as a completely alterative possibility, it could mean you have been breathing a lot of pollutants. Smoke of various kinds (from fires, from smoking, etc) can cause this.
Black
There are various possible explanations here and all of them are bad. Get thee to a doctor. Superficial examples include:
- Fungal infection (you thought toxic black mold was bad when it was on the wall of the house, wait until it’s on the walls of your respiratory system)
- Blood, in abundance, oxidized (which begs the question of what caused that, but certainly: something wrong is not right)
- Pollutants again, but this time at absurd levels of exposure
That last one might sound very transient and self-correcting, but it’s not, and it comes with many increased short- and long-term health risks.
Want to know more?
Knowledge is power, so read up, and stay well:
- Beyond Supplements: The Real Immune-Boosters!
- The Cold Truth About Respiratory Infections
- Why Some People Get Sick More (And How To Not Be One Of Them)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: