How To Escape From A Despairing Mood
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When we are in a despairing mood, that’s when it can feel hardest to actually implement anything we know about getting out of one. That’s why sometimes, the simplest solutions are the best:
Imagination Is Key
Despairing moods occur when it’s hard to envision a better life. Imagination is the power to envision alternatives, such as new jobs, relationships, or lifestyle, but sadness can cloud our ability to imagine solutions like changing careers, moving house, or starting fresh. With enough imagination, most problems can be worked around—and new opportunities can always be found.
Importantly: we are not bound by our past or present circumstances; we have the freedom and flexibility to choose new paths. That doesn’t mean it’ll always be a walk in the park, but “this too shall pass”.
You may be thinking: “sometimes the hardship does pass, but can last many years”, and that is true. All the more reason to check if there’s a freer lane you can slip into to speed ahead. Even if there isn’t, the mere act of imagining such lanes is already respite from the hardships—and having envisioned such will make it much easier for you to recognise when opportunities for change do come along.
To foster imagination, we are advised to expose ourselves to different narratives, preparing ourselves for alternative ways of living. Thus, we can reframe life’s challenges as intellectual puzzles, urging us to rebuild creatively and find new solutions!
For more on all this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Behavioral Activation Against Depression & Anxiety
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What will aged care look like for the next generation? More of the same but higher out-of-pocket costs

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Aged care financing is a vexed problem for the Australian government. It is already underfunded for the quality the community expects, and costs will increase dramatically. There are also significant concerns about the complexity of the system.
In 2021–22 the federal government spent A$25 billion on aged services for around 1.2 million people aged 65 and over. Around 60% went to residential care (190,000 people) and one-third to home care (one million people).
The final report from the government’s Aged Care Taskforce, which has been reviewing funding options, estimates the number of people who will need services is likely to grow to more than two million over the next 20 years. Costs are therefore likely to more than double.
The taskforce has considered what aged care services are reasonable and necessary and made recommendations to the government about how they can be paid for. This includes getting aged care users to pay for more of their care.
But rather than recommending an alternative financing arrangement that will safeguard Australians’ aged care services into the future, the taskforce largely recommends tidying up existing arrangements and keeping the status quo.
No Medicare-style levy
The taskforce rejected the aged care royal commission’s recommendation to introduce a levy to meet aged care cost increases. A 1% levy, similar to the Medicare levy, could have raised around $8 billion a year.
The taskforce failed to consider the mix of taxation, personal contributions and social insurance which are commonly used to fund aged care systems internationally. The Japanese system, for example, is financed by long-term insurance paid by those aged 40 and over, plus general taxation and a small copayment.
Instead, the taskforce puts forward a simple, pragmatic argument that older people are becoming wealthier through superannuation, there is a cost of living crisis for younger people and therefore older people should be required to pay more of their aged care costs.
Separating care from other services
In deciding what older people should pay more for, the taskforce divided services into care, everyday living and accommodation.
The taskforce thought the most important services were clinical services (including nursing and allied health) and these should be the main responsibility of government funding. Personal care, including showering and dressing were seen as a middle tier that is likely to attract some co-payment, despite these services often being necessary to maintain independence.
The task force recommended the costs for everyday living (such as food and utilities) and accommodation expenses (such as rent) should increasingly be a personal responsibility.

Aged care users will pay more of their share for cooking and cleaning.
Lizelle Lotter/ShutterstockMaking the system fairer
The taskforce thought it was unfair people in residential care were making substantial contributions for their everyday living expenses (about 25%) and those receiving home care weren’t (about 5%). This is, in part, because home care has always had a muddled set of rules about user co-payments.
But the taskforce provided no analysis of accommodation costs (such as utilities and maintenance) people meet at home compared with residential care.
To address the inefficiencies of upfront daily fees for packages, the taskforce recommends means testing co-payments for home care packages and basing them on the actual level of service users receive for everyday support (for food, cleaning, and so on) and to a lesser extent for support to maintain independence.
It is unclear whether clinical and personal care costs and user contributions will be treated the same for residential and home care.
Making residential aged care sustainable
The taskforce was concerned residential care operators were losing $4 per resident day on “hotel” (accommodation services) and everyday living costs.
The taskforce recommends means tested user contributions for room services and everyday living costs be increased.
It also recommends that wealthier older people be given more choice by allowing them to pay more (per resident day) for better amenities. This would allow providers to fully meet the cost of these services.
Effectively, this means daily living charges for residents are too low and inflexible and that fees would go up, although the taskforce was clear that low-income residents should be protected.
Moving from buying to renting rooms
Currently older people who need residential care have a choice of making a refundable up-front payment for their room or to pay rent to offset the loans providers take out to build facilities. Providers raise capital to build aged care facilities through equity or loan financing.
However, the taskforce did not consider the overall efficiency of the private capital market for financing aged care or alternative solutions.
Instead, it recommended capital contributions be streamlined and simplified by phasing out up-front payments and focusing on rental contributions. This echoes the royal commission, which found rent to be a more efficient and less risky method of financing capital for aged care in private capital markets.
It’s likely that in a decade or so, once the new home care arrangements are in place, there will be proportionally fewer older people in residential aged care. Those who do go are likely to be more disabled and have greater care needs. And those with more money will pay more for their accommodation and everyday living arrangements. But they may have more choice too.
Although the federal government has ruled out an aged care levy and changes to assets test on the family home, it has yet to respond to the majority of the recommendations. But given the aged care minister chaired the taskforce, it’s likely to provide a good indication of current thinking.

Hal Swerissen, Emeritus Professor, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Sugar Alcohol That Reduces BMI!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Inositol Does-It-Ol’!
First things first, a quick clarification up-front:
Myo-inositol or D-chiro-inositol?
We’re going to be talking about inositol today, which comes in numerous forms, but most importantly:
- Myo-inositol (myo-Ins)
- D-chiro-inositol (D-chiro-Ins)
These are both inositol, (a sugar alcohol!) and for our purposes today, the most relevant form is myo-inositol.
The studies we’ll look at today are either:
- just about myo-inositol, or
- about myo-inositol in the presence of d-chiro-inositol at a 40:1 ratio.
You have both in your body naturally; wherever supplementation is mentioned, it means supplementing with either:
- extra myo-inositol (because that’s the one the body more often needs more of), or
- both, at the 40:1 ratio that we mentioned above (because that’s one way to help balance an imbalanced ratio)
With that in mind…
Inositol against diabetes?
Inositol is known to:
- decrease insulin resistance
- increase insulin sensitivity
- have an important role in cell signaling
- have an important role in metabolism
The first two things there both mean that inositol is good against diabetes. It’s not “take this and you’re cured”, but:
- if you’re pre-diabetic it may help you avoid type 2 diabetes
- if you are diabetic (either type) it can help in the management of your diabetes.
It does this by allowing your body to make better use of insulin (regardless of whether that insulin is from your pancreas or from the pharmacy).
How does it do that? Research is still underway and there’s a lot we don’t know yet, but here’s one way, for example:
❝Evidence showed that inositol phosphates might enhance the browning of white adipocytes and directly improve insulin sensitivity through adipocytes❞
Read: Role of Inositols and Inositol Phosphates in Energy Metabolism
We mentioned its role in metabolism in a bullet-point above, and we didn’t just mean insulin sensitivity! There’s also…
Inositol for thyroid function?
The thyroid is one of the largest endocrine glands in the body, and it controls how quickly the body burns energy, makes proteins, and how sensitive the body should be to other hormones. So, it working correctly or not can have a big impact on everything from your mood to your weight to your energy levels.
How does inositol affect thyroid function?
- Inositol has an important role in thyroid function and dealing with autoimmune diseases.
- Inositol is essential to produce H2O2 (yes, really) required for the synthesis of thyroid hormones.
- Depletion of inositol may lead to the development of some thyroid diseases, such as hypothyroidism.
- Inositol supplementation seems to help in the management of thyroid diseases.
Read: The Role of Inositol in Thyroid Physiology and in Subclinical Hypothyroidism Management
Inositol for PCOS?
A systematic review published in the Journal of Gynecological Endocrinology noted:
- Inositol can restore spontaneous ovarian activity (and consequently fertility) in most patients with PCOS.
- Myo-inositol is a safe and effective treatment to improve:
- ovarian function
- healthy metabolism
- healthy hormonal balance
While very comprehensive (which is why we included it here), that review’s a little old, so…
Check out this cutting edge (Jan 2023) study whose title says it all:
Inositol for fertility?
Just last year, Mendoza et al published that inositol supplementation, together with antioxidants, vitamins, and minerals, could be an optimal strategy to improve female fertility.
This built from Gambiole and Forte’s work, which laid out how inositol is a safe compound for many issues related to fertility and pregnancy. In particular, several clinical trials demonstrated that:
- inositol can have therapeutic effects in infertile women
- inositol can also be useful as a preventive treatment during pregnancy
- inositol could prevent the onset of neural tube defects
- inositol also reduces the occurrence of gestational diabetes
Due to the safety and efficiency of inositol, it can take the place of many drugs that are contraindicated in pregnancy. Basically: take this, and you’ll need fewer other drugs. Always a win!
Read: Myo-Inositol as a Key Supporter of Fertility and Physiological Gestation
Inositol For Weight Loss
We promised you “this alcohol sugar can reduce your BMI”, and we weren’t making it up!
Zarezadeh et al conducited a very extensive systematic review, and found:
- Oral inositol supplementation has positive effect on BMI reduction.
- Inositol in the form of myo-inositol had the strongest effect on BMI reduction.
- Participants with PCOS and/or who were overweight, experienced the most significant improvement of all.
Want some inositol?
As ever, we don’t sell it (or anything else), but for your convenience, here’s myo-inositol and d-chiro-inositol at a 40:1 ratio, available on Amazon!
Share This Post
-

End the Insomnia Struggle – by Dr. Colleen Ehrnstrom and Dr. Alisha Brosse
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed sleep books before, and we always try to recommend books that have something a little different than the rest, so what makes this one stand out?
While there is the usual quick overview of the basics that we’re sure you already know (sleep hygiene etc), most of the attention here is given to cold, hard clinical psychology… in a highly personalized way.
How, you may ask, can they personalize a book, that is the same for everyone?
The answer is, by guiding the reader through examining our own situation. With template logbooks, worksheets, and the like—for this reason we recommend getting a paper copy of the book, rather than the Kindle version, in case you’d like to use/photocopy those.
Essentially, reading this book is much like having your own psychologist (or two) to guide you through finding a path to better sleep.
The therapeutic approach, by the way, is a combination of Cognitive Behavioral Therapy (CBT) and Acceptance-Commitment Therapy (ACT), which work very well together here.
Bottom line: if you’ve changed your bedsheets and turned off your electronic devices and need something a little more, this book is the psychological “big guns” for removing the barriers between you and good sleep.
Click here to check out End the Insomnia Struggle, and end yours once and for all!
Share This Post


Related Posts
-

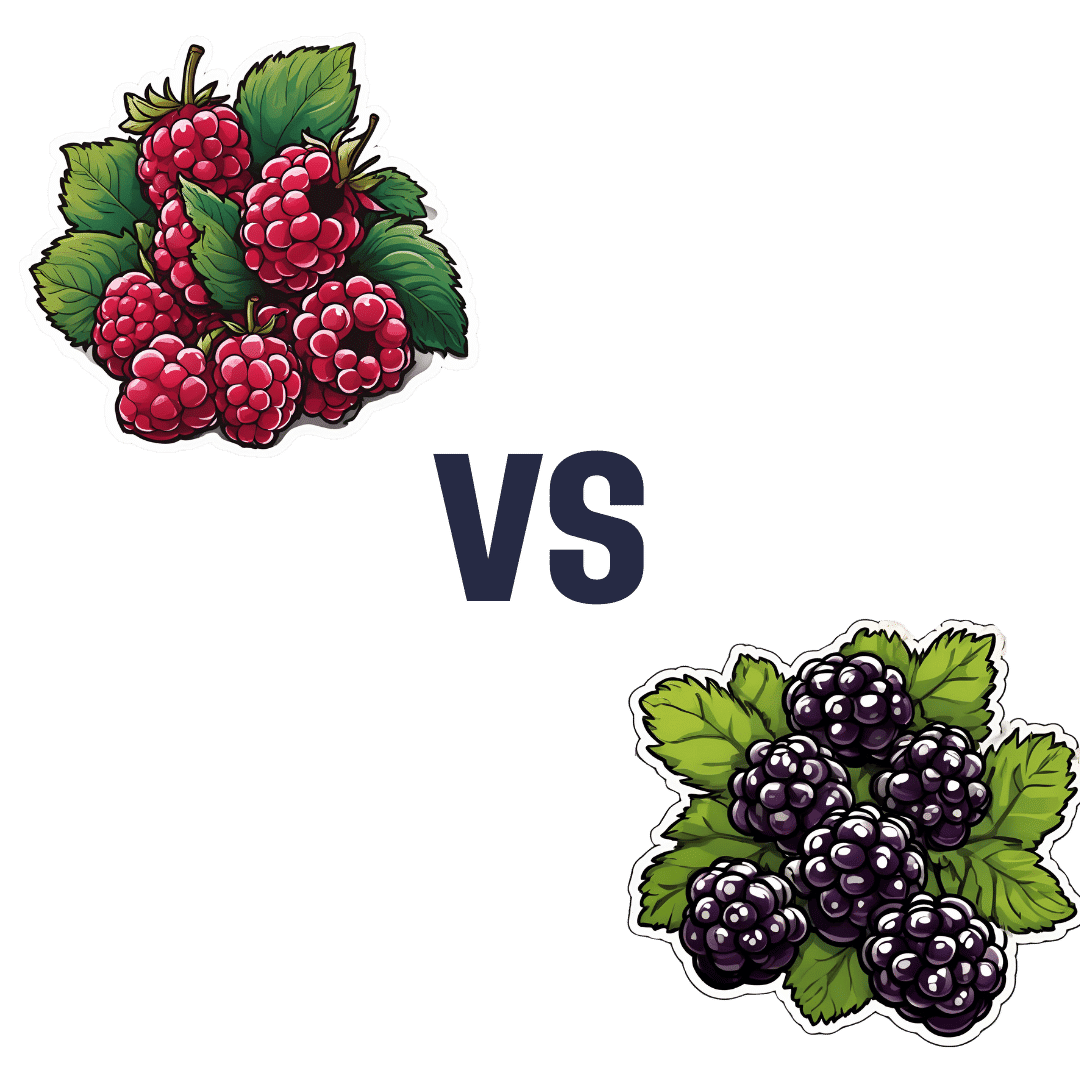
Raspberries vs Blackberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing raspberries to blackberries, we picked the blackberries.
Why?
It was very close! Raspberries most certainly also have their merits. But blackberries do just a little bit better in a few categories:
In terms of macros, raspberries have a tiny bit more carbs and fiber, while blackberries have a even tinier bit more protein, and the two berries have an equal glycemic index. We’ll call this category a tie, or else the meanest of nominal wins for raspberry.
In the category of vitamins, raspberries have more of vitamins B1, B2, B5, B6, and choline, while blackberries have more of vitamins A, B3, B9, C, E, and K. This would be a very marginal win for blackberries, except that blackberries have more than 6x the vitamin A, a much larger margin than any of the other differences in vitamins (which were usually small differences), which gives blackberry a more convincing win here.
When it comes to minerals, things are closer: raspberries have more iron, magnesium, manganese, and phosphorus, while blackberries have more calcium, copper, potassium, selenium, and zinc. None of the differences are outstanding, so this is a simple marginal victory for blackberries.
It would be rude to look at berries without noting their polyphenols; we’re not list them all (or this article will get very long, because each has very many polyphenols with names like “pelargonidin 3-O-glucosyl-rutinoside” and so forth), but suffice it to say: raspberries are great for polyphenols and blackberries are even better for polyphenols.
That said… In the category of specific polyphenols we’ve written about before at 10almonds, it’s worth noting a high point of each berry, for the sake of fairness: raspberries have more quercetin (but blackberries have lots too) and blackberries have more ellagic acid (of which, raspberries have some, but not nearly as much). Anyway, just going off total polyphenol content, blackberries are the clear winner here.
Adding up the sections makes for an overall win for blackberries, but by all means, enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
21 Most Beneficial Polyphenols & What Foods Have Them
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
As Nuns Disappear, Many Catholic Hospitals Look More Like Megacorporations
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
ST. LOUIS — Inside the more than 600 Catholic hospitals across the country, not a single nun can be found occupying a chief executive suite, according to the Catholic Health Association.
Nuns founded and led those hospitals in a mission to treat sick and poor people, but some were also shrewd business leaders. Sister Irene Kraus, a former chief executive of Daughters of Charity National Health System, was famous for coining the phrase “no margin, no mission.” It means hospitals must succeed — generating enough revenue to exceed expenses — to fulfill their original mission.
The Catholic Church still governs the care that can be delivered to millions in those hospitals each year, using religious directives to ban abortions and limit contraceptives, in vitro fertilization, and medical aid in dying.
But over time, that focus on margins led the hospitals to transform into behemoths that operate for-profit subsidiaries and pay their executives millions, according to hospital tax filings. These institutions, some of which are for-profit companies, now look more like other megacorporations than like the charities for the destitute of yesteryear.
The absence of nuns in the top roles raises the question, said M. Therese Lysaught, a Catholic moral theologist and professor at Loyola University Chicago: “What does it mean to be a Catholic hospital when the enterprise has been so deeply commodified?”
The St. Louis area serves as the de facto capital of Catholic hospital systems. Three of the largest are headquartered here, along with the Catholic hospital lobbying arm. Catholicism is deeply rooted in the region’s culture. During Pope John Paul II’s only U.S. stop in 1999, he led Mass downtown in a packed stadium of more than 100,000 people.
For a quarter century, Sister Mary Jean Ryan led SSM Health, one of those giant systems centered on St. Louis. Now retired, the 86-year-old said she was one of the last nuns in the nation to lead a Catholic hospital system.
Ryan grew up Catholic in Wisconsin and joined a convent while in nursing school in the 1960s, surprising her family. She admired the nuns she worked alongside and felt they were living out a higher purpose.
“They were very impressive,” she said. “Not that I necessarily liked all of them.”
Indeed, the nuns running hospitals defied the simplistic image often ascribed to them, wrote John Fialka in his book “Sisters: Catholic Nuns and the Making of America.”
“Their contributions to American culture are not small,” he wrote. “Ambitious women who had the skills and the stamina to build and run large institutions found the convent to be the first and, for a long time, the only outlet for their talents.”
This was certainly true for Ryan, who climbed the ranks, working her way from nurse to chief executive of SSM Health, which today has hospitals in Illinois, Missouri, Oklahoma, and Wisconsin.
The system was founded more than a century ago when five German nuns arrived in St. Louis with $5. Smallpox swept through the city and the Sisters of St. Mary walked the streets offering free care to the sick.
Their early foray grew into one of the largest Catholic health systems in the country, with annual revenue exceeding $10 billion, according to its 2023 audited financial report. SSM Health treats patients in 23 hospitals and co-owns a for-profit pharmacy benefit manager, Navitus, that coordinates prescriptions for 14 million people.
But Ryan, like many nuns in leadership roles in recent decades, found herself confronted with an existential crisis. As fewer women became nuns, she had to ensure the system’s future without them.
When Ron Levy, who is Jewish, started at SSM as an administrator, he declined to lead a prayer in a meeting, Ryan recounted in her book, “On Becoming Exceptional.”
“Ron, I’m not asking you to be Catholic,” she recalled telling him. “And I know you’ve only been here two weeks. So, if you’d like to make it three, I suggest you be prepared to pray the next time you’re asked.”
Levy went on to serve SSM for more than 30 years — praying from then on, Ryan wrote.
In Catholic hospitals, meetings are still likely to start with a prayer. Crucifixes often adorn buildings and patient rooms. Mission statements on the walls of SSM facilities remind patients: “We reveal the healing presence of God.”
Above all else, the Catholic faith calls on its hospitals to treat everyone regardless of race, religion, or ability to pay, said Diarmuid Rooney, a vice president of the Catholic Health Association. No nuns run the trade group’s member hospitals, according to the lobbying group. But the mission that compelled the nuns is “what compels us now,” Rooney said. “It’s not just words on a wall.”
The Catholic Health Association urges its hospitals to evaluate themselves every three years on whether they’re living up to Catholic teachings. It created a tool that weighs seven criteria, including how a hospital acts as an extension of the church and cares for poor and marginalized patients.
“We’re not relying on hearsay that the Catholic identity is alive and well in our facilities and hospitals,” Rooney said. “We can actually see on a scale where they are at.”
The association does not share the results with the public.
At SSM Health, “our Catholic identity is deeply and structurally ingrained” even with no nun at the helm, spokesperson Patrick Kampert said. The system reports to two boards. One functions as a typical business board of directors while the other ensures the system abides by the rules of the Catholic Church. The church requires the majority of that nine-member board to be Catholic. Three nuns currently serve on it; one is the chair.
Separately, SSM also is required to file an annual report with the Vatican detailing the ways, Kampert said, “we deepen our Catholic identity and further the healing ministry of Jesus.” SSM declined to provide copies of those reports.
From a business perspective, though, it’s hard to distinguish a Catholic hospital system like SSM from a secular one, said Ruth Hollenbeck, a former Anthem insurance executive who retired in 2018 after negotiating Missouri hospital contracts. In the contracts, she said, the difference amounted to a single paragraph stating that Catholic hospitals wouldn’t do anything contrary to the church’s directives.
To retain tax-exempt status under Internal Revenue Service rules, all nonprofit hospitals must provide a “benefit” to their communities such as free or reduced-price care for patients with low incomes. But the IRS provides a broad definition of what constitutes a community benefit, which gives hospitals wide latitude to justify not needing to pay taxes.
On average, the nation’s nonprofit hospitals reported that 15.5% of their total annual expenses were for community benefits in 2020, the latest figure available from the American Hospital Association.
SSM Health, including all of its subsidiaries, spent proportionately far less than the association’s average for individual hospitals, allocating roughly the same share of its annual expenses to community efforts over three years: 5.1% in 2020, 4.5% in 2021, and 4.9% in 2022, according to a KFF Health News analysis of its most recent publicly available IRS filings and audited financial statements.
A separate analysis from the Lown Institute think tank placed five Catholic systems — including the St. Louis region’s Ascension — on its list of the 10 health systems with the largest “fair share” deficits, which means receiving more in tax breaks than what they spent on the community. And Lown said three St. Louis-area Catholic health systems — Ascension, SSM Health, and Mercy — had fair share deficits of $614 million, $235 million, and $92 million, respectively, in the 2021 fiscal year.
Ascension, Mercy, and SSM disputed Lown’s methodology, arguing it doesn’t take into account the gap between the payments they receive for Medicaid patients and the cost of delivering their care. The IRS filings do.
But, Kampert said, many of the benefits SSM provides aren’t reflected in its IRS filings either. The forms reflect “very simplistic calculations” and do not accurately represent the health system’s true impact on the community, he said.
Today, SSM Health is led by longtime business executive Laura Kaiser. Her compensation in 2022 totaled $8.4 million, including deferred payments, according to its IRS filing. Kampert defended the amount as necessary “to retain and attract the most qualified” candidate.
By contrast, SSM never paid Ryan a salary, giving instead an annual contribution to her convent of less than $2 million a year, according to some tax filings from her long tenure. “I didn’t join the convent to earn money,” Ryan said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Over-50s Physio: What My 5 Oldest Patients (Average Age 92) Do Right
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Oftentimes, people of particularly advanced years will be asked their secret to longevity, and sometimes the answers aren’t that helpful because they don’t actually know, and ascribe it to some random thing. Will Harlow, the over-50s specialist physio, talks about the top 5 science-based things that his 5 oldest patients do, that enhances the healthy longevity that they are enjoying:
The Top 5’s Top 5
Here’s what they’re doing right:
Daily physical activity: all five patients maintain a consistent habit of daily exercise, which includes activities like exercise classes, home workouts, playing golf, or taking daily walks. They prioritize movement even when it’s difficult, rarely skipping a day unless something serious happened. A major motivator was the fear of losing mobility, as they had seen spouses, friends, or family members stop exercising and never start again.
Stay curious: a shared trait among the patients was their curiosity and eagerness to learn. They enjoy meeting new people, exploring new experiences, and taking on new challenges. Two of them attended the University of the Third Age to learn new skills, while another started playing bridge as a new hobby. The remaining two have recently made new friends. They all maintain a playful attitude, a good sense of humor, and aren’t afraid to fail or laugh at themselves.
Prioritize sleep (but not too much): the patients each average seven hours of sleep per night, aligning with research suggesting that 7–9 hours of sleep is ideal for health. They maintain consistent sleep and wake-up times, which contributes to their well-being. While they allow themselves short naps when needed, they avoid long afternoon naps to avoid disrupting their sleep patterns.
Spend time in nature: spending time outdoors is a priority for all five individuals. Whether through walking, gardening, or simply sitting on a park bench, they make it a habit to connect with nature. This aligns with studies showing that time spent in natural environments, especially near water, significantly reduces stress. When water isn’t accessible, green spaces still provide a beneficial boost to mental health.
Stick to a routine: the patients all value simple daily routines, such as enjoying an evening cup of tea, taking a daily walk, or committing to small gardening tasks. These routines offer mental and physical grounding, providing stability even when life becomes difficult sometimes. They emphasized the importance of keeping routines simple and manageable to ensure they could stick to them regardless of life’s challenges.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Top 8 Habits Of The Top 1% Healthiest Over-50s ← another approach to the same question, this time with a larger sample size, and/but many younger (than 90s) respondents.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: