Putting a Halt to Feeling Lost, Anxious, Stressed & Unhappy
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Starting From the Middle
Today’s video (below) dives straight into the heart of the issue, examining the victim mindset, with Dr. Gabor Maté immediately, and quite vulnerably, sharing his personal experiences conquering feelings of despair and anxiety.
As one of the comments on the video says, Dr. Maté is a “person who teaches about something because they experience it themselves”. And it shows through his approach.
With raw honesty, Dr. Maté empathizes with those grappling with inner turmoil, offering hope by emphasizing the power of healing in the present moment.
What is His Method?
Explained simply, Dr. Maté urges individuals to seek trauma-informed care and therapies that address underlying wounds; he emphasizes the pitfalls of relying solely on medication, and instead highlights the idea that triggers can be seen as opportunities for self-reflection and growth. He urges individuals to approach their triggers with compassionate curiosity rather than self-judgment.
In short, Dr Maté’s empathetic approach immediately calms the viewer, whilst providing knowledge crucial to self-improvement.
Let this video act as a reminder that we should take our mental health as seriously as our general health.
How was the video? If you’ve discovered any great videos yourself that you’d like to share with fellow 10almonds readers, then please do email them to us!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cabbage vs Cauliflower – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cabbage to cauliflower, we picked the cauliflower.
Why?
First, let’s note: these are two different cultivars of the same species (Brassica oleracea) and/but as usual (we say, as there are a lot of cultivars of Brassica oleracea, and we’ve done a fair few pairings of them before) there are still nutritional differences to consider, such as…
In terms of macros, cabbage has very slightly more carbs and fiber, while cauliflower has very slightly more protein. However, the numbers are all so close (and the glycemic index equal), such that we’re going to call the macros category a tie.
In the category of vitamins, cabbage has more of vitamins A, B1, E, and K, while cauliflower has more of vitamins B2, B3, B5, B6, B7, B9, C, and choline. Superficially, this is a clear 8:4 win for cauliflower; it’s worth noting though that the differences in amounts are mostly small, so this isn’t as big a win as it looks like. Still a win for cauliflower, though.
When it comes to minerals, it’s a similar story: cabbage has a little more calcium, iron, and manganese, while cauliflower has a little more copper, magnesium, phosphorus, potassium, and zinc. This time a 6:3 win for cauliflower, and again, the margins are small so there’s really not as much between them as it looks like. Still a win for cauliflower, though.
In short: enjoy either or both (diversity is good), but the most nutritionally dense is cauliflower, even if cabbage isn’t far behind it.
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Take care!
Share This Post
-
Strength training has a range of benefits for women. Here are 4 ways to get into weights
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Picture a gym ten years ago: the weights room was largely a male-dominated space, with women mostly doing cardio exercise. Fast-forward to today and you’re likely to see women of all ages and backgrounds confidently navigating weights equipment.
This is more than just anecdotal. According to data from the Australian Sports Commission, the number of women participating in weightlifting (either competitively or not) grew nearly five-fold between 2016 and 2022.
Women are discovering what research has long shown: strength training offers benefits beyond sculpted muscles.

John Arano/Unsplash Health benefits
Osteoporosis, a disease in which the bones become weak and brittle, affects more women than men. Strength training increases bone density, a crucial factor for preventing osteoporosis, especially for women negotiating menopause.
Strength training also improves insulin sensitivity, which means your body gets better at using insulin to manage blood sugar levels, reducing the risk of type 2 diabetes. Regular strength training contributes to better heart health too.
There’s a mental health boost as well. Strength training has been linked to reduced symptoms of depression and anxiety.
Strength training can have a variety of health benefits. Ground Picture/Shutterstock Improved confidence and body image
Unlike some forms of exercise where progress can feel elusive, strength training offers clear and tangible measures of success. Each time you add more weight to a bar, you are reminded of your ability to meet your goals and conquer challenges.
This sense of achievement doesn’t just stay in the gym – it can change how women see themselves. A recent study found women who regularly lift weights often feel more empowered to make positive changes in their lives and feel ready to face life’s challenges outside the gym.
Strength training also has the potential to positively impact body image. In a world where women are often judged on appearance, lifting weights can shift the focus to function.
Instead of worrying about the number on the scale or fitting into a certain dress size, women often come to appreciate their bodies for what they can do. “Am I lifting more than I could last month?” and “can I carry all my groceries in a single trip?” may become new measures of physical success.
Strength training can have positive effects on women’s body image. Drazen Zigic/Shutterstock Lifting weights can also be about challenging outdated ideas of how women “should” be. Qualitative research I conducted with colleagues found that, for many women, strength training becomes a powerful form of rebellion against unrealistic beauty standards. As one participant told us:
I wanted something that would allow me to train that just didn’t have anything to do with how I looked.
Society has long told women to be small, quiet and not take up space. But when a woman steps up to a barbell, she’s pushing back against these outdated rules. One woman in our study said:
We don’t have to […] look a certain way, or […] be scared that we can lift heavier weights than some men. Why should we?
This shift in mindset helps women see themselves differently. Instead of worrying about being objects for others to look at, they begin to see their bodies as capable and strong. Another participant explained:
Powerlifting changed my life. It made me see myself, or my body. My body wasn’t my value, it was the vehicle that I was in to execute whatever it was that I was executing in life.
This newfound confidence often spills over into other areas of life. As one woman said:
I love being a strong woman. It’s like going against the grain, and it empowers me. When I’m physically strong, everything in the world seems lighter.
Feeling inspired? Here’s how to get started
1. Take things slow
Begin with bodyweight exercises like squats, lunges and push-ups to build a foundation of strength. Once you’re comfortable, add external weights, but keep them light at first. Focus on mastering compound movements, such as deadlifts, squats and overhead presses. These exercises engage multiple joints and muscle groups simultaneously, making your workouts more efficient.
2. Prioritise proper form
Always prioritise proper form over lifting heavier weights. Poor technique can lead to injuries, so learning the correct way to perform each exercise is crucial. To help with this, consider working with an exercise professional who can provide personalised guidance and ensure you’re performing exercises correctly, at least initially.
Bodyweight exercises, such as lunges, are a good way to get started before lifting weights. antoniodiaz/Shutterstock 3. Consistency is key
Like any fitness regimen, consistency is key. Two to three sessions a week are plenty for most women to see benefits. And don’t be afraid to occupy space in the weights room – remember you belong there just as much as anyone else.
4. Find a community
Finally, join a community. There’s nothing like being surrounded by a group of strong women to inspire and motivate you. Engaging with a supportive community can make your strength-training journey more enjoyable and rewarding, whether it’s an in-person class or an online forum.
Are there any downsides?
Gym memberships can be expensive, especially for specialist weightlifting gyms. Home equipment is an option, but quality barbells and weightlifting equipment can come with a hefty price tag.
Also, for women juggling work and family responsibilities, finding time to get to the gym two to three times per week can be challenging.
If you’re concerned about getting too “bulky”, it’s very difficult for women to bulk up like male bodybuilders without pharmaceutical assistance.
The main risks come from poor technique or trying to lift too much too soon – issues that can be easily avoided with some guidance.
Erin Kelly, Lecturer and PhD Candidate, Discipline of Sport and Exercise Science, University of Canberra
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Oral vaccines could provide relief for people who suffer regular UTIs. Here’s how they work
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In a recent TikTok video, Australian media personality Abbie Chatfield shared she was starting a vaccine to protect against urinary tract infections (UTIs).
Huge news for the UTI girlies. I am starting a UTI vaccine tonight for the first time.
Chatfield suffers from recurrent UTIs and has turned to the Uromune vaccine, an emerging option for those seeking relief beyond antibiotics.
But Uromune is not a traditional vaccine injected to your arm. So what is it and how does it work?
9nong/Shutterstock First, what are UTIs?
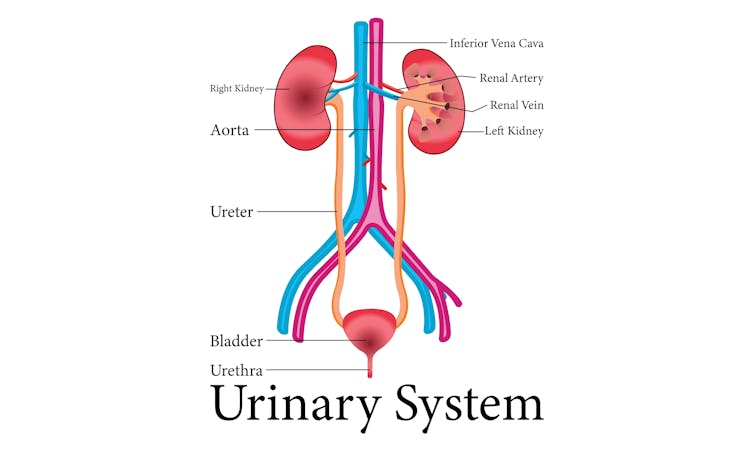
UTIs are caused by bacteria entering the urinary system. This system includes the kidneys, bladder, ureters (thin tubes connecting the kidneys to the bladder), and the urethra (the tube through which urine leaves the body).
The most common culprit is Escherichia coli (E. coli), a type of bacteria normally found in the intestines.
While most types of E. coli are harmless in the gut, it can cause infection if it enters the urinary tract. UTIs are particularly prevalent in women due to their shorter urethras, which make it easier for bacteria to reach the bladder.
Roughly 50% of women will experience at least one UTI in their lifetime, and up to half of those will have a recurrence within six months.
UTIs are caused by bacteria enterning the urinary system. oxo7051/Shutterstock The symptoms of a UTI typically include a burning sensation when you wee, frequent urges to go even when the bladder is empty, cloudy or strong-smelling urine, and pain or discomfort in the lower abdomen or back. If left untreated, a UTI can escalate into a kidney infection, which can require more intensive treatment.
While antibiotics are the go-to treatment for UTIs, the rise of antibiotic resistance and the fact many people experience frequent reinfections has sparked more interest in preventive options, including vaccines.
What is Uromune?
Uromune is a bit different to traditional vaccines that are injected into the muscle. It’s a sublingual spray, which means you spray it under your tongue. Uromune is generally used daily for three months.
It contains inactivated forms of four bacteria that are responsible for most UTIs, including E. coli. By introducing these bacteria in a controlled way, it helps your immune system learn to recognise and fight them off before they cause an infection. It can be classified as an immunotherapy.
A recent study involving 1,104 women found the Uromune vaccine was 91.7% effective at reducing recurrent UTIs after three months, with effectiveness dropping to 57.6% after 12 months.
These results suggest Uromune could provide significant (though time-limited) relief for women dealing with frequent UTIs, however peer-reviewed research remains limited.
Any side effects of Uromune are usually mild and may include dry mouth, slight stomach discomfort, and nausea. These side effects typically go away on their own and very few people stop treatment because of them. In rare cases, some people may experience an allergic reaction.
How can I access it?
In Australia, Uromune has not received full approval from the Therapeutic Goods Administration (TGA), and so it’s not something you can just go and pick up from the pharmacy.
However, Uromune can be accessed via the TGA’s Special Access Scheme or the Authorised Prescriber pathway. This means a GP or specialist can apply for approval to prescribe Uromune for patients with recurrent UTIs. Once the patient has a form from their doctor documenting this approval, they can order the vaccine directly from the manufacturer.
Antibiotics are the go-to treatment for UTIs – but scientists are looking at options to prevent them in the first place. Photoroyalty/Shutterstock Uromune is not covered under the Pharmaceutical Benefits Scheme, meaning patients must cover the full cost out-of-pocket. The cost of a treatment program is around A$320.
Uromune is similarly available through special access programs in places like the United Kingdom and Europe.
Other options in the pipeline
In addition to Uromune, scientists are exploring other promising UTI vaccines.
Uro-Vaxom is an established immunomodulator, a substance that helps regulate or modify the immune system’s response to bacteria. It’s derived from E. coli proteins and has shown success in reducing UTI recurrences in several studies. Uro-Vaxom is typically prescribed as a daily oral capsule taken for 90 days.
FimCH, another vaccine in development, targets something called the adhesin protein that helps E. coli attach to urinary tract cells. FimCH is typically administered through an injection and early clinical trials have shown promising results.
Meanwhile, StroVac, which is already approved in Germany, contains inactivated strains of bacteria such as E. coli and provides protection for up to 12 months, requiring a booster dose after that. This injection works by stimulating the immune system in the bladder, offering temporary protection against recurrent infections.
These vaccines show promise, but challenges like achieving long-term immunity remain. Research is ongoing to improve these options.
No magic bullet, but there’s reason for optimism
While vaccines such as Uromune may not be an accessible or perfect solution for everyone, they offer real hope for people tired of recurring UTIs and endless rounds of antibiotics.
Although the road to long-term relief might still be a bit bumpy, it’s exciting to see innovative treatments like these giving people more options to take control of their health.
Iris Lim, Assistant Professor in Biomedical Science, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post






-

This Naked Mind – by Annie Grace
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve all read about the many, many, dangers of drinking. We’ve also probably all read about how to make the change to not drinking. Put things out of sight, tell your friends, have this rule, have this excuse (for not drinking) ready to give to people who challenge you, consider a support group, and so on.
What Annie Grace offers in this #1 bestseller is different:
A blend of mostly psychology and sociology, to examine the “liminal thinking” stages that funnel us to drink in the first place… and where that leads, and how to clamber back out of the pitcher plant we weren’t necessarily aware we were sliding into.
While she kicks off citing Jung, from a psychological perspective more of this book is CBTish, as it pertains a lot to examining the process of:
- belief—held and defended, based on the…
- conclusion—drawn, often irrationally, from the…
- experience—that we had upon acting on an…
- observation—often mistaking an illusion for the underlying…
- reality
…and how we can and often do go wrong at each step, and how little of the previous steps we can perceive at any given time.
What does this mean for managing/treating alcoholism or a tendency towards alchoholism?
It means interrupting those processes in a careful, surgically precise fashion, so that suddenly… The thing has no more power over us.
Whether you or a loved one struggle with a tendency to addiction (any addiction, actually, the advice goes the same), or are just curious about the wider factors at hand in the epidemiology of addiction, this book is for you.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Blood-Sugar-Friendly Ice Pops
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This generic food product has so many regional variant names that it’s difficult to get a universal name, but in N. America they’re also known by the genericized brand name of popsicles. Anyway, they’re usually very bad news for blood sugars, being merely frozen juice even if extra sugar wasn’t added. Today’s recipe, on the other hand, makes for a refreshing and nutrient-dense treat that won’t spike your blood glucose!
You will need
- 1 cup fresh blueberries
- 1 can (12oz/400g) coconut milk
- ½ cup yogurt with minimal additives
- 1 tbsp honey (omit if you prefer less sweetness)
- Juice of ¼ lime (increase if you prefer more sourness)
Method
(we suggest you read everything at least once before doing anything)
1) Blend everything
2) Pour into ice pop molds and freeze overnight
3) Serve at your leisure:
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Which Sugars Are Healthier, And Which Are Just The Same?
- 10 Ways To Balance Blood Sugars
- Can Saturated Fats Be Healthy? ← the fats in coconut are a good source of medium-chain triglycerides (MCTs), which are easily broken down as a good energy source and (enjoyed in moderation) thus unlikely to cause any cardiovascular problems, as little to nothing (usually: nothing) of it will be stored.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

To tackle gendered violence, we also need to look at drugs, trauma and mental health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
After several highly publicised alleged murders of women in Australia, the Albanese government this week pledged more than A$925 million over five years to address men’s violence towards women. This includes up to $5,000 to support those escaping violent relationships.
However, to reduce and prevent gender-based and intimate partner violence we also need to address the root causes and contributors. These include alcohol and other drugs, trauma and mental health issues.
Why is this crucial?
The World Health Organization estimates 30% of women globally have experienced intimate partner violence, gender-based violence or both. In Australia, 27% of women have experienced intimate partner violence by a co-habiting partner; almost 40% of Australian children are exposed to domestic violence.
By gender-based violence we mean violence or intentionally harmful behaviour directed at someone due to their gender. But intimate partner violence specifically refers to violence and abuse occurring between current (or former) romantic partners. Domestic violence can extend beyond intimate partners, to include other family members.
These statistics highlight the urgent need to address not just the aftermath of such violence, but also its roots, including the experiences and behaviours of perpetrators.
What’s the link with mental health, trauma and drugs?
The relationships between mental illness, drug use, traumatic experiences and violence are complex.
When we look specifically at the link between mental illness and violence, most people with mental illness will not become violent. But there is evidence people with serious mental illness can be more likely to become violent.
The use of alcohol and other drugs also increases the risk of domestic violence, including intimate partner violence.
About one in three intimate partner violence incidents involve alcohol. These are more likely to result in physical injury and hospitalisation. The risk of perpetrating violence is even higher for people with mental ill health who are also using alcohol or other drugs.
It’s also important to consider traumatic experiences. Most people who experience trauma do not commit violent acts, but there are high rates of trauma among people who become violent.
For example, experiences of childhood trauma (such as witnessing physical abuse) can increase the risk of perpetrating domestic violence as an adult.
Childhood trauma can leave its mark on adults years later. Roman Yanushevsky/Shutterstock Early traumatic experiences can affect the brain and body’s stress response, leading to heightened fear and perception of threat, and difficulty regulating emotions. This can result in aggressive responses when faced with conflict or stress.
This response to stress increases the risk of alcohol and drug problems, developing PTSD (post-traumatic stress disorder), and increases the risk of perpetrating intimate partner violence.
How can we address these overlapping issues?
We can reduce intimate partner violence by addressing these overlapping issues and tackling the root causes and contributors.
The early intervention and treatment of mental illness, trauma (including PTSD), and alcohol and other drug use, could help reduce violence. So extra investment for these are needed. We also need more investment to prevent mental health issues, and preventing alcohol and drug use disorders from developing in the first place.
Early intervention and treatment of mental illness, trauma and drug use is important. Okrasiuk/Shutterstock Preventing trauma from occuring and supporting those exposed is crucial to end what can often become a vicious cycle of intergenerational trauma and violence. Safe and supportive environments and relationships can protect children against mental health problems or further violence as they grow up and engage in their own intimate relationships.
We also need to acknowledge the widespread impact of trauma and its effects on mental health, drug use and violence. This needs to be integrated into policies and practices to reduce re-traumatising individuals.
How about programs for perpetrators?
Most existing standard intervention programs for perpetrators do not consider the links between trauma, mental health and perpetrating intimate partner violence. Such programs tend to have little or mixed effects on the behaviour of perpetrators.
But we could improve these programs with a coordinated approach including treating mental illness, drug use and trauma at the same time.
Such “multicomponent” programs show promise in meaningfully reducing violent behaviour. However, we need more rigorous and large-scale evaluations of how well they work.
What needs to happen next?
Supporting victim-survivors and improving interventions for perpetrators are both needed. However, intervening once violence has occurred is arguably too late.
We need to direct our efforts towards broader, holistic approaches to prevent and reduce intimate partner violence, including addressing the underlying contributors to violence we’ve outlined.
We also need to look more widely at preventing intimate partner violence and gendered violence.
We need developmentally appropriate education and skills-based programs for adolescents to prevent the emergence of unhealthy relationship patterns before they become established.
We also need to address the social determinants of health that contribute to violence. This includes improving access to affordable housing, employment opportunities and accessible health-care support and treatment options.
All these will be critical if we are to break the cycle of intimate partner violence and improve outcomes for victim-survivors.
The National Sexual Assault, Family and Domestic Violence Counselling Line – 1800 RESPECT (1800 737 732) – is available 24 hours a day, seven days a week for any Australian who has experienced, or is at risk of, family and domestic violence and/or sexual assault.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14. In an emergency, call 000.
Siobhan O’Dean, Postdoctoral Research Associate, The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney; Lucinda Grummitt, Postdoctoral Research Fellow, The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney, and Steph Kershaw, Research Fellow, The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: