

90% Of People Skip This Essential Exercise—Are You One Of Them?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Single-leg strengthening is essential for joint health at any age (unless you want to bunny-hop up and down the stairs with both feet at once, for example), yet many people overlook it. This neglect often leads to pain, stiffness, and a higher risk of injury.
Dr. Alyssa Kuhn, arthritis specialist, explains how to do it:
On the rise
In this video, different exercise variations—beginner, intermediate, and advanced—are presented to help you build strength at your own pace:
Beginner: start by using a chair, adding a cushion for support if needed. Sit at the edge and position one foot slightly in front of the other in a staggered stance. Stand up and sit down in a controlled manner, allowing the back leg to bear more weight and work harder than the front leg. Do 8–10 repetitions per side and pay attention to whether one side feels weaker. To build strength, incorporate this movement into daily activities, such as standing up from the couch. Master this variation before progressing, to avoid knee injury.
Intermediate: to make the exercise more challenging, you can either use a lower chair, or extend your front foot further out, shifting more weight to your back leg. Only modify one variable at a time to maintain control. Do 8–10 repetitions per side, ensuring proper form. A common mistake is allowing the back knee to move inward, which can cause knee stress. To prevent this, use a mirror to check your form and keep the knee and ankle aligned during movement.
Advanced: when you’re ready, extend your front leg completely with the heel on the ground and toes up, removing its stability and forcing the back leg to work even harder. Maintain controlled movement while keeping your knee and ankle aligned. Repeat the exercise on both sides, focusing extra effort on the weaker leg to build balanced strength.
For more on each of these, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Secret To Better Squats: Foot, Knee, & Ankle Mobility
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between vegan and vegetarian?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
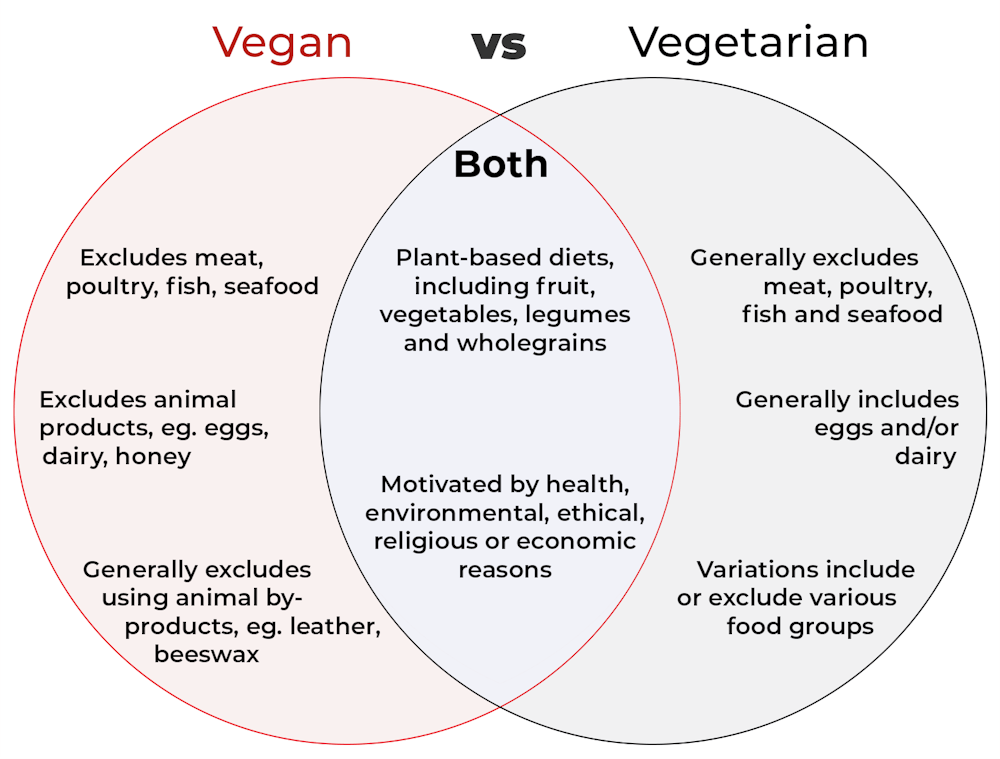
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?

Creative Cat Studio/Shutterstock What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.
More than a diet: veganism can form part of someone’s identity. Shutterstock So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Optimal Morning Routine, Per Neuroscience
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Andrew Huberman, neuroscientist and professor of neurobiology, has insights:
The foundations of a good day
Here are some key things to consider:
- The role of light: get sunlight exposure within an hour of waking to anchor your body’s cortisol pulse, set your circadian rhythm, and boost mood-regulating dopamine. Light exposure on the skin also boost hormone levels like testosterone and estrogen, contributing to energy, motivation, and overall wellbeing.
- The role of caffeine: delay caffeine intake for 60–90 minutes after waking to allow adenosine to clear naturally, preventing afternoon energy crashes. Otherwise, caffeine will block the adenosine for 4–8 hours, causing the wave of adenosine-induced sleepiness to resurge later.
- The role of exercise: morning exercise helps clear adenosine, raise core body temperature, and improve wakefulness
- The role of cold: cold showers or ice baths trigger adrenaline and dopamine surges, enhancing mood and drive for hours.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Morning Routines That Just Flow
Take care!
Share This Post
-
Red Cabbage vs Red Lettuce – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing red cabbage to red lettuce, we picked the red cabbage.
Why?
It was close! But…
In terms of macros, red cabbage has more than 2x the fiber, more than 2x the carbs, and slightly more protein, making for an easy win for red cabbage in this round.
Note: this happens often, by the way, that something has the same numerical (factorial) increase in fiber and carbs, and we declare it the winner; it’s important to understand that these things do not cancel each other out when they’re scaling equally. By this we mean: if we say fiber is good, carbs are bad (the latter isn’t true; we need carbs to live, but carbs without fiber can indeed be bad), then let’s look at how much we need of each. Different advisory bodies say we need anywhere from 25g/day fiber to 40g/day fiber. Suffice it to say, we need a lot more than 40g/day carbs for regular maintenance of life. Which means that if carbs and fiber in a food are increased by the same amount, gram for gram, then this is increasingly good, because we’ll reach the daily requirement for fiber a lot sooner than we’ll reach the daily requirement for carbs.
Another way of looking at it would be if instead of looking at the grams of fiber or carbs, we look at how much each food provides of the RDA, then it becomes very clear very quickly why we prioritize the fiber figure, because each gram increase of fiber is a much bigger %-of-RDA increase, than the equivalent per-gram figure for carbs. Thus, much more relevant for health considerations.
Ok, back to the usual format of comparisons:
Moving on to the vitamins next, red cabbage has more of vitamins B3, B5, B6, C, and choline, while red lettuce has more of vitamins A, B2, B9, E, and K. That’s a 5:5 tie with a similar average margin of difference, so we’ll call this round a respectable tie and point to them both having very good, but different, merits.
Looking at minerals, red cabbage mas more calcium, magnesium, manganese, and potassium, while red lettuce has more copper, iron, and selenium. A marginal win for red cabbage here.
When it comes to phytochemicals, they each boast a comparable array of polyphenols, so it’s a tie in this round.
Adding up the sections makes for an overall win for red cabbage, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Share This Post



-
Cabbage vs Zucchini – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cabbage to zucchini, we picked the cabbage.
Why?
In terms of macros, cabbage has 2.5x the fiber, as well as slightly more protein and carbs, making it the more nutrient-dense option in the macronutrient category.
In the category of vitamins, cabbage has more of vitamins B1, B5, B7, B9, C, E, and K, while zucchini has more of vitamins A, B2, B3, and B6, yielding a 7:4 win to cabbage in this round.
Looking at minerals next, cabbage has more calcium and iron, while zucchini has more copper, magnesium, phosphorus, potassium, and zinc, winning a round finally.
In other considerations, cabbages also have notably more polyphenols, so that’s another round in their favor.
Adding up the sections makes for a clear overall win for cabbages, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
Super-Nutritious Shchi ← for what to do with that cabbage
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Cuddle therapy sounds like what we all need right now – but will it actually help?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cuddle therapy is having a moment. The idea for this emerging therapy is for you to book in a specified time with a “professional cuddler”.
Websites promote cuddle therapists as specialists in platonic touch, offering a service to people who wish to cuddle for friendship, to relax or manage emotional challenges.
The aim is to find connection and improve your mental health and wellbeing.
But does it actually work?
Here’s what you need to think about before booking in.
RDNE Stock project/Pexels What is cuddle therapy?
Cuddle therapists offer consensual, non-sexual cuddles in a structured and safe environment, designed to be free from criticism, bias, conflict and any behaviour or conversation that may feel unsafe or threatening.
Cuddle therapists are not official or regulated professionals. There do not appear to be any accredited training programs or professional bodies that oversee and regulate cuddle therapy.
However, there are numerous people who promote themselves as professional cuddlers, and whose services are said to offer a range of psychological and physiological benefits.
These include reductions in depression, anxiety and loneliness, improvements in social skills and immune functioning, lowered blood pressure and a decreased risk of heart disease.
Providers suggest cuddle therapy can also lessen symptoms of post‑traumatic stress disorder, enhance a person’s capacity to recover from experiences of sexual or physical abuse, and reduce cravings associated with substance use.
Comforting claims, sparse science
Despite such claims, there do not appear to be any published peer‑reviewed studies that directly examine the psychological or physiological effects of engaging a professional cuddler.
There is, however, a broader body of research exploring the benefits of non‑sexual physical touch, including hugging and gentle, sustained contact.
Such touch has been associated with reductions in daily stress and improvements in overall wellbeing. Physical touch has also been identified as a way of conveying empathy, social bonding, and care.
Most of this research focuses on touch in close relationships – such as with partners, parents or friends – rather than touch delivered by a practitioner as part of a paid service. So, we don’t know if these findings translate to cuddle therapy.
There are however, known impacts of physical touch, including prompting the release of the hormone oxytocin. Oxytocin interacts with other neurochemicals, most notably dopamine, which supports feelings of comfort and connection.
Together, these neurochemical responses help explain why sustained touch can have a calming and soothing effect.
Professional cuddles need professional boundaries
Because cuddle therapy involves physical touch, emotional vulnerability and power dynamics between therapist and client, it raises a number of important ethical and professional issues.
1. Provide informed consent
If you’re thinking about cuddle therapy, ask what the service does and does not involve. Get a clear explanation about the boundaries of the service, where touch is and is not permitted, and the structure of the session.
You’ll need to provide explicit and informed consent before proceeding, and you can withdraw consent at any time.
2. Professional boundaries must be clear
A cuddle therapy relationship should remain professional at all times.
It is not OK for your cuddle therapist to express personal or romantic interest, or that the connection is becoming “special” or exclusive in ways that go beyond the agreed‑upon service.
Likewise, a practitioner should never pressure you to share personal information or disclose more than you are comfortable with.
Maintaining firm boundaries helps ensure the interaction remains safe, respectful and centred on your wellbeing rather than blurring into a personal relationship.
3. Watch you’re not becoming dependent
You may seek cuddle therapy because you are vulnerable, including but not limited to being lonely, depressed or in emotional pain. It is understandable that a touch‑based session may help you feel cared for, grounded or safe in the moment.
However, you should also watch for signs you are becoming dependent on a practitioner for emotional stability or comfort. This might include believing you can only feel calm, safe or OK after seeing that specific practitioner or wanting increasing contact or more cuddle therapy sessions.
4. It’s no cure for complex issues
Similarly, while cuddle therapy can offer temporary relief and a sense of connection, it is not designed to resolve underlying psychological issues or replace professional mental health care.
So cuddle therapy should be viewed as a supportive experience, but not a cure for broader or more complex emotional challenges.
Key takeaways
Taken together, cuddle therapy is an emerging practice centred on consensual, non‑sexual physical touch delivered in a structured environment. It’s promoted online as a way to reduce distress and enhance emotional wellbeing.
Cuddle therapy remains unregulated, with no formal training pathways or governing bodies overseeing professional standards. So service providers, rather than empirical evidence, largely shape public information about cuddle therapy.
Evidence suggests a range of benefits of physical touch. However, if you do pursue cuddle therapy you should ensure there are clear boundaries, you provide informed consent, and know you can withdraw that consent at any time.
Glen Hosking, Clinical Psychologist and Associate Professor of Psychology, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
When They Don’t Recognize You Anymore
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It happened more than a decade ago, but the moment remains with her.
Sara Stewart was talking at the dining room table with her mother, Barbara Cole, 86 at the time, in Bar Harbor, Maine. Stewart, then 59, a lawyer, was making one of her extended visits from out of state.
Two or three years earlier, Cole had begun showing troubling signs of dementia, probably from a series of small strokes. “I didn’t want to yank her out of her home,” Stewart said.
So with a squadron of helpers — a housekeeper, regular family visitors, a watchful neighbor, and a meal delivery service — Cole remained in the house she and her late husband had built 30-odd years earlier.
She was managing, and she usually seemed cheerful and chatty. But this conversation in 2014 took a different turn.
“She said to me: ‘Now, where is it we know each other from? Was it from school?’” her daughter and firstborn recalled. “I felt like I’d been kicked.”
Stewart remembers thinking, “In the natural course of things, you were supposed to die before me. But you were never supposed to forget who I am.” Later, alone, she wept.
People with advancing dementia do regularly fail to recognize beloved spouses, partners, children, and siblings. By the time Stewart and her youngest brother moved Cole into a memory-care facility a year later, she had almost completely lost the ability to remember their names or their relationship to her.
“It’s pretty universal at the later stages” of the disease, said Alison Lynn, director of social work at the Penn Memory Center, who has led support groups for dementia caregivers for a decade.
She has heard many variations of this account, a moment described with grief, anger, frustration, relief, or some combination thereof.
These caregivers “see a lot of losses, reverse milestones, and this is one of those benchmarks, a fundamental shift” in a close relationship, she said. “It can throw people into an existential crisis.”
It’s hard to determine what people with dementia — a category that includes Alzheimer’s disease and many other cognitive disorders — know or feel. “We don’t have a way of asking the person or looking at an MRI,” Lynn noted. “It’s all deductive.”
But researchers are starting to investigate how family members respond when a loved one no longer appears to know them. A qualitative study recently published in the journal Dementia analyzed in-depth interviews with adult children caring for mothers with dementia who, at least once, did not recognize them.
“It’s very destabilizing,” said Kristie Wood, a clinical research psychologist at the University of Colorado Anschutz Medical Campus and co-author of the study. “Recognition affirms identity, and when it’s gone, people feel like they’ve lost part of themselves.”
Although they understood that nonrecognition was not rejection but a symptom of their mothers’ disease, she added, some adult children nevertheless blamed themselves.
“They questioned their role. ‘Was I not important enough to remember?’” Wood said. They might withdraw or visit less often.
Pauline Boss, the family therapist who developed the theory of “ambiguous loss” decades ago, points out that it can involve physical absence — as when a soldier is missing in action — or psychological absence, including nonrecognition because of dementia.
Society has no way to acknowledge the transition when “a person is physically present but psychologically absent,” Boss said. There is “no death certificate, no ritual where friends and neighbors come sit with you and comfort you.”
“People feel guilty if they grieve for someone who’s still alive,” she continued. “But while it’s not the same as a verified death, it is a real loss and it just keeps coming.”
Nonrecognition takes different forms. Some relatives report that while a loved one with dementia can no longer retrieve a name or an exact relationship, they still seem happy to see them.
“She stopped knowing who I was in the narrative sense, that I was her daughter Janet,” Janet Keller, 69, an actress in Port Townsend, Washington, said in an email about her late mother, diagnosed with Alzheimer’s. “But she always knew that I was someone she liked and wanted to laugh with and hold hands with.”
It comforts caregivers to still feel a sense of connection. But one of the respondents in the Dementia study reported that her mother felt like a stranger and that the relationship no longer provided any emotional reward.
“I might as well be visiting the mailman,” she told the interviewer.
Larry Levine, 67, a retired health care administrator in Rockville, Maryland, watched his husband’s ability to recognize him shift unpredictably.
He and Arthur Windreich, a couple for 43 years, had married when Washington, D.C., legalized same-sex marriage in 2010. The following year, Windreich received a diagnosis of early-onset Alzheimer’s.
Levine became his caregiver until his death at 70, in late 2023.
“His condition sort of zigzagged,” Levine said. Windreich had moved into a memory-care unit. “One day, he’d call me ‘the nice man who comes to visit’,” Levine said. “The next day he’d call me by name.”
Even in his final years when, like many dementia patients, Windreich became largely nonverbal, “there was some acknowledgment,” his husband said. “Sometimes you could see it in his eyes, this sparkle instead of the blank expression he usually wore.”
At other times, however, “there was no affect at all.” Levine often left the facility in tears.
He sought help from his therapist and his sisters, and recently joined a support group for LGBTQ+ dementia caregivers even though his husband has died. Support groups, in person or online, “are medicine for the caregiver,” Boss said. “It’s important not to stay isolated.”
Lynn encourages participants in her groups to also find personal rituals to mark the loss of recognition and other reverse milestones. “Maybe they light a candle. Maybe they say a prayer,” she said.
Someone who would sit shiva, part of the Jewish mourning ritual, might gather a small group of friends or family to reminisce and share stories, even though the loved one with dementia hasn’t died.
“To have someone else participate can be very validating,” Lynn said. “It says, ‘I see the pain you’re going through.’”
Once in a while, the fog of dementia seems to lift briefly.
Researchers at Penn and elsewhere have pointed to a startling phenomenon called “paradoxical lucidity.” Someone with severe dementia, after being noncommunicative for months or years, suddenly regains alertness and may come up with a name, say a few appropriate words, crack a joke, make eye contact, or sing along with a radio.
Though common, these episodes generally last only seconds and don’t mark a real change in the person’s decline. Efforts to recreate the experiences tend to fail.
“It’s a blip,” Lynn said. But caregivers often respond with shock and joy; some interpret the episode as evidence that despite deepening dementia, they are not truly forgotten.
Stewart encountered such a blip a few months before her mother died. She was in her mother’s apartment when a nurse asked her to come down the hall.
“As I left the room, my mother called out my name,” she said. Though Cole usually seemed pleased to see her, “she hadn’t used my name for as long as I could remember.”
It didn’t happen again, but that didn’t matter. “It was wonderful,” Stewart said.
The New Old Age is produced through a partnership with The New York Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:



