16 Overlooked Autistic Traits In Women
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We hear a lot about “autism moms”, but Taylor Heaton is an autistic mom, diagnosed as an adult, and she has insights to share about overlooked autistic traits in women.
The Traits
- Difficulty navigating romantic relationships: often due to misreading signs
- Difficulty understanding things: including the above, but mostly: difficulty understanding subtext, when people leave things as “surely obvious”. Autistic women are likely to be aware of the possible meanings, but unsure which it might be, and may well guess wrongly.
- Masking: one of the reasons for the gender disparity in diagnosis is that autistic women are often better at “masking”, that is to say, making a conscious effort to blend in to allistic society—often as a result of being more societally pressured to do so.
- Honesty: often to a fault
- Copy and paste: related to masking, this is about consciously mirroring others in an effort to put them at ease and be accepted
- Being labelled sensitive and/or gifted: usually this comes at a young age, but the resultant different treatment can have a lifetime effect
- Secret stims: again related to masking, and again for the same reasons that displaying autistic symptoms is often treated worse in women, autistic women’s stims tend to be more subtle.
- Written communication: autistic women are often more comfortable with the written word than the spoken
- Leadership: autistic women will often gravitate to leadership roles, partly as a survival mechanism
- Gaslighting: oneself, e.g. “If this person did this without that, then I can to” (without taking into account that maybe the circumstances are different, or maybe they actually did lean on crutches that you didn’t know were there, etc).
- Inner dialogue: rich inner dialogue, but unable to express it outwardly—often because of the sheer volume of thoughts per second.
- Fewer female friends: often few friends overall, for that matter, but there’s often a gender imbalance towards male friends, or where there isn’t, towards more masculine friends at least.
- Feeling different: often a matter of feeling one does not meet standard expectations in some fashion
- School: autistic women are often academically successful
- Special interests: often more “socially accepted” interests than autistic men’s.
- Flirting: autistic women are often unsure how to flirt or what to do about it, which can result in simple directness instead
For more details on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Related reading:
You might like a main feature of ours from not long back:
Miss Diagnosis: Anxiety, ADHD, & Women
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Other Alzheimer’s Risk Factor

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The usually-listed 7 known risk factors of dementia (in general, not just Alzheimer’s) do not include today’s item. For a recap, those were:
The 7 Known Risk Factors For Dementia
The bonus risk factor
This idea is not completely novel; it’s been known for a while that traumatic brain injury (TBI) can increase the risk of dementia, but it has generally been chalked up to “if you damage an organ, then that organ does not function so well afterwards”.
However, in the case of Alzheimer’s, it seems there’s something deeper at play. Specifically, a study that found…
❝…traumatic brain injury alters the small vessels in the brain, resulting in an accumulation of amyloid beta—a hallmark of Alzheimer’s disease.
The findings suggest that vascular dysfunction could be an early driver in neurodegenerative disorders rather than being caused by neuronal damage.❞
This association held true even in quite young patients!
The study from Sweden looked at brain tissue from TBI patients (who had had to have brain tissue removed for medical reasons due to bleeding and swelling), and found that the (traumatic) changes to the vascular smooth muscle cells were associated with increased aggregation of amyloid-β.
In terms of establishing cause and effect: since it could be safely concluded the amyloid-β had not caused the TBI (which all had external explanations such as “car crash” or such), it can be deduced that almost* certainly the TBI caused the amyloid-β aggregation.
*because little to nothing in science is every truly certain. As in life in general, really; the difference is that scientists admit it!
You may be wondering: what was the control? It would be a very generous group of citizens indeed who would volunteer bits of their brains that hadn’t needed removing. However, the answer is that the control brain bits came from a biobank, and were from uninjured patients with no history of TBI or neurodegenerative disorders, and who had died from systemic, unrelated causes. Having been dead for a matter of hours, and the fixation time for the brain bits from the living people taking long enough that everybody’s brain bits had been out of their respective living bodies for a similar length of time, this was deemed an acceptable, if imperfect, control.
You can read the study in its entirety here; it is fascinating:
The practical take-away
The practical take-away, of course, is: look after your brain
Not just in the sense of eat fiber, get healthy fats, move more, get good sleep, stay intellectually stimulated, etc*, but also in the sense of “keep your brain physically safe”.
Now, you may think that you already try not to get into car crashes, and perhaps you do not compete in contact sports, but do be aware that one of the leading causes of TBI in older people is, ignominiously, falling down.
And if you think “that only happens to older/other people”, then be aware: there’s a first time for everything and you are not immune. With that in mind, do check out:
Fall Special! ← the seasonal title notwithstanding, this is about not falling down in the first place, and being less injurable if you do fall down
*This was a modest and vague list for brevity’s sake, so for much more detail, enjoy:
How To Reduce Your Alzheimer’s Risk ← this is rather more comprehensive
Want to know more?
Here you can read about the largest study of its kind into lifestyle factors and Alzheimer’s disease:
Alzheimer’s Causative Factors To Avoid ← the methods and conclusions of Dr. David Snowdon’s famous “Nun Study”
Take care!
Share This Post
-
What is mantle cell lymphoma? Magda Szubanski’s ‘rare and fast-moving’ cancer, explained
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Beloved Australian actor, Magda Szubanski, has revealed she’s been diagnosed with a “very rare, very aggressive, very serious” blood cancer called mantle cell lymphoma.
In a post on social media on Thursday, Szubanski said she would be starting treatment in a few weeks for the stage 4 cancer, which she called “one of the nasty ones, unfortunately”.
So, what is mantle cell lymphoma? And how is it treated?

Lisa Maree Williams/Getty What is mantle cell lymphoma?
There are more than 100 subtypes of blood cancers, but they are commonly divided into one of two groups. These are based on where they originate: leukaemias develop in the bone marrow, and lymphomas develop in the lymphatic system.
Lymphomas develop from white blood cells (lymphocytes), which circulate in the blood and lymphatic system and help fight infection.
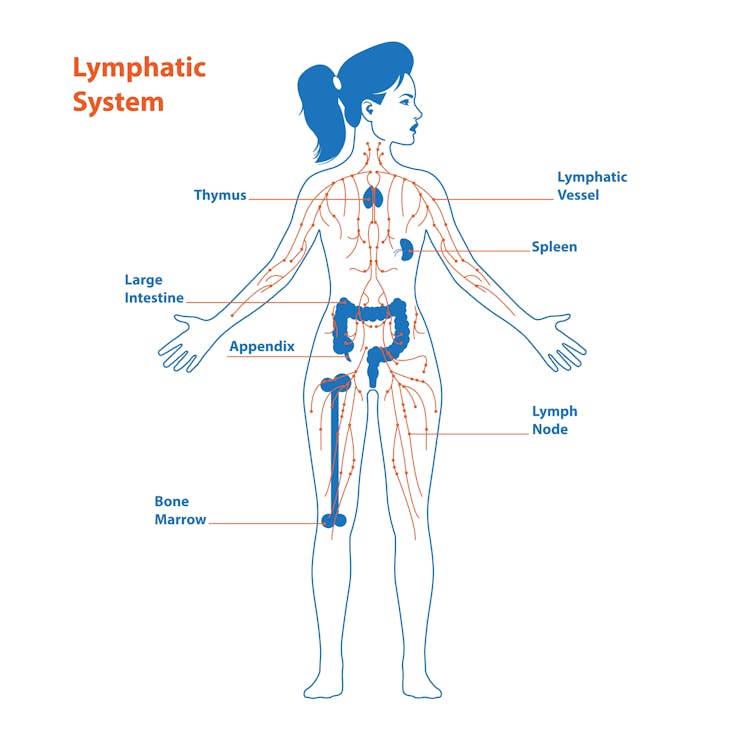
You may not have heard of the lymphatic system, but it plays a key role in your immune response.
The lymphatic circulatory system is responsible for transporting fluids (lymph) around your body. Lymph comes from blood plasma, and helps remove waste from your tissues.
As part of the lymphatic system, tissues like the spleen and thymus help produce many of the immune cells you use to fight infections.
These cells are then housed in specialised organs called lymph nodes – small pea-sized glands located throughout your body.
The lymphatic system plays a key role in your body’s immune response. Clash_Gene/Shutterstock Lymph nodes are kind of like the “war room” of your immune system.
Your body contains hundreds of lymph nodes, and each contains millions of lymphocytes. These include the T and B cells – the main fighting cells in adaptive immunity.
If B cells in an area of the lymph node known as the “mantle zone” become cancerous, it is called mantle cell lymphoma.
How rare is it?
In 2020, there were 330 cases of mantle cell lymphoma diagnosed in Australia, accounting for a small fraction (5%) of lymphoma cases.
Overall, lymphomas account for around one in twenty new cancer diagnoses. This makes mantle cell lymphoma quite rare.
Mantle cell lymphoma is about three times more common in men than in women, and mostly affects people over the age of 60.
Is there a cure?
Unfortunately, mantle cell lymphoma is largely considered incurable with the therapies currently available.
Like many cancers, mantle cell lymphoma can vary in how quickly it develops and its severity.
As Szubanski’s cancer has been described as “fast-moving” and is already stage 4, it appears that it is a more serious case.
Stage 4 is the most advanced stage – meaning the cancer has spread (metastasised) to other tissues.
Treatment at this stage can be more complicated than when the cancer is caught earlier. But treatment can still help people go on to live for many years.
What does treatment involve?
In her social media post, Szubanski said she will be receiving “one of the best treatments available (the Nordic protocol)”.
This is one of the most common treatments for an aggressive lymphoma.
The main component is “R-CHOP” – a combination therapy. It involves a mixture of different drugs, including chemotherapy, to attack the cancer from multiple angles at the same time.
Different strengths of the drugs can be used (the maximum strength is sometimes called R-maxi-CHOP).
A stem cell transplantation may also be included in the regimen.
How effective this treatment is will depend on many different factors, including the type and stage of the lymphoma.
The aim is to kill as many cancer cells as possible, and therefore extend a patient’s life for as long as possible.
Therapy also focuses on providing a high quality-of-life for patients.
How is it diagnosed?
Szubanski’s mantle cell lymphoma was detected during a breast cancer screen where, she says, “they found my lymph nodes were up”.
Imaging techniques, such as a mammogram or MRI, may detect tell-tale signs of lymphoma, such as swollen lymph nodes.
However a biopsy – a small sample of tissue from the affected area – would then be required to confirm the presence of cancer cells and identify what type.
Blood cancer symptoms can be vague, but it’s good to know what to look for.
As well as swollen lymph nodes, symptoms of lymphoma include nausea, tiredness, loss of appetite, fevers, gastrointestinal issues, unexplained weight loss, and night sweats.
If you have any concerns, you should consult a doctor.
John (Eddie) La Marca, Senior Research Officer, Blood Cells and Blood Cancer, WEHI (Walter and Eliza Hall Institute of Medical Research) and Sarah Diepstraten, Senior Research Officer, Blood Cells and Blood Cancer Division, WEHI (Walter and Eliza Hall Institute of Medical Research)
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Unwell Women – by Dr. Elinor Cleghorn
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For a demographic that makes up a little over half of the world’s population, women are paradoxically marginalized in healthcare. And in other ways too, but this book is about health.
Dr. Cleghorn had to fight for seven (!) years to get her own lupus condition recognized as such, and continues to have to fight for it to be taken seriously on an ongoing basis. And yet, 95% of the book is not about her and her experiences, but rather, the bigger picture.
The book is divided into sections, by period in history. From Hippocrates to the modern day, Dr. Cleghorn gives us a well-researched, incredibly well-referenced overview of the marginalization of women’s health. Far from being a dry history book in the early parts though, it’s fascinating and engaging throughout.
The modern day sections are part shining a light into dark areas, part practical information-and-advice “did you know this happens, and you can do this about it”, and part emphatic call-to-action to demand better.
Bottom line: this book is in this reviewer’s “top 5 books read this year”, and we highly recommend it to you.
Share This Post


Related Posts
-
Almonds vs Pecans – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing almonds to pecans, we picked the almonds.
Why?
In terms of macros, almonds have more protein, carbs, and fiber, as well as the lower glycemic index. A strong start for almonds here, though pecans have more fat (and the healthy blend of fats is quite comparable from one nut to the other).
In the category of vitamins, almonds have more of vitamins B2, B3, B9, E, and choline, while pecans have more of vitamins A, B1, B5, B6, and K. Numerically that’s a tie, though the biggest margins of difference are for vitamins A and E, respectively, and we might want to prioritize almonds’ extra vitamin E, over pecans’ extra vitamin A, given that vitamin A is more easily found in large quantities in many foods, whereas vitamin E is not quite so abundant generally. So in short, either a tie or a slight win for almonds here.
When it comes to minerals, both contain a lot of goodness, but almonds have more calcium, iron, magnesium, phosphorus, potassium, and selenium, while pecans have more copper, manganese, and zinc. A clear win for almonds, though as we say, pecans are also great for this, just not as great as almonds.
As a side-note, both of these nuts have been found to have anticancer properties against breast cancer cell lines. In all likelihood this means they help against other cancers too, but breast cancer is what the extant research has been for.
So, naturally, enjoy either or both (in fact, both is ideal). But if you want to choose one for nutritional density, it’s almonds.
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Low-Carb Fraud by Dr. T. Colin Campbell & Dr. Howard Jacobson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The first-named author is most well-known for “The China Study”, and the work here is consistent with that, albeit from the opposite angle.
While critical of low-carb diets in general (as low-carb diets tend to be de facto low-fiber diets—they don’t have to be, but the way most people do them, they are*), it’s quite clear that one of the main purposes of this book was to serve as a rebuttal—refutation, even—of the paleo diet.
*This is, as presented, the low-carb paradox. People promote low-carb diets because high-carb foods with minimal fiber will zip straight through the digestive system and set up camp in the liver and visceral fat, but the problem is that if a low-carb diet is pursued without adequate fiber (and usually with too much saturated fat), this will not be an improvement. Thus, per Drs. Campbell & Johnson, the answer is not avoiding carbs, but rather, prioritizing fiber (which almost always comes with carbs, while low-carb foods usually have quite little, or in the case of animal products, none).
The style is old-school pop-science, but the science itself is sound, and referenced heavily with a proportional bibliography. Speaking of proportions, it’s worth mentioning that this book is one fifth the size of The China Study, making it a much quicker read.
Bottom line: if you’re considering a low-carb diet and want to know the counterarguments without investing a lot of time into it, then this light book will present it for you clearly and in a well-sourced fashion.
Click here to check out The Low-Carb Fraud, and enjoy the right carbs instead!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Want the health benefits of strength training but not keen on the gym? Try ‘exercise snacking’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The science is clear: resistance training is crucial to ageing well. Lifting weights (or doing bodyweight exercises like lunges, squats or push-ups) can help you live independently for longer, make your bones stronger, reduce your risk of diseases such as diabetes, and may even improve your sleep and mental health.
But not everyone loves the gym. Perhaps you feel you’re not a “gym person” and never will be, or you’re too old to start. Being a gym-goer can be expensive and time-consuming, and some people report feeling unwelcome or awkward at the gym.
The good news is you don’t need the gym, or lots of free time, to get the health benefits resistance training can offer.
You can try “exercise snacking” instead.
Pressmaster/Shutterstock What is exercise snacking?
Exercise snacking involves doing multiple shorter bouts (as little as 20 seconds) of exercise throughout the day – often with minimal or no equipment. It’s OK to have several hours of rest between.
You could do simple bodyweight exercises such as:
- chair sit-to-stand (squats)
- lunges
- box step-ups
- calf raises
- push-ups.
Exercise snacking like this can help improve muscle mass, strength and physical function.
It’s OK to hold onto a nearby object for balance, if you need. And doing these exercises regularly will also improve your balance. That, in turn, reduces your risk of falls and fractures.
OK I have done all those, now what?
Great! You can also try using resistance bands or dumbbells to do the previously mentioned five exercises as well as some of the following exercises:
When using resistance bands, make sure you hold them tightly and that they’re securely attached to an immovable object.
Exercise snacking works well when you pair it with an activity you do often throughout the day. Perhaps you could:
- do a few extra squats every time you get up from a bed or chair
- do some lunges during a TV ad break
- chuck in a few half squats while you’re waiting for your kettle to boil
- do a couple of elevated push-ups (where you support your body with your hands on a chair or a bench while doing the push-up) before tucking into lunch
- sneak in a couple of calf raises while you’re brushing your teeth.
Exercise snacking involves doing multiple shorter bouts (as little as 20 seconds) of exercise throughout the day. Cavan-Images/Shutterstock What does the evidence say about exercise snacking?
One study had older adults without a history of resistance training do exercise snacks at home twice per day for four weeks.
Each session involved five simple bodyweight exercises (chair sit-to-stand, seated knee extension, standing knee bends, marching on the spot, and standing calf raises). The participants did each exercise continuously for one minute, with a one-minute break between exercises.
These short and simple exercise sessions, which lasted just nine minutes, were enough to improve a person’s ability to stand up from a chair by 31% after four weeks (compared to a control group who didn’t exercise). Leg power and thigh muscle size improved, too.
Research involving one of us (Jackson Fyfe) has also shown older adults found “exercise snacking” feasible and enjoyable when done at home either once, twice, or three times per day for four weeks.
Exercise snacking may be a more sustainable approach to improve muscle health in those who don’t want to – or can’t – lift heavier weights in a gym.
A little can yield a lot
We know from other research that the more you exercise, the more likely it is you will keep exercising in future.
Very brief resistance training, albeit with heavier weights, may be more enjoyable than traditional approaches where people aim to do many, many sets.
We also know brief-and-frequent exercise sessions can break up periods of sedentary behaviour (which usually means sitting too much). Too much sitting increases your risk of chronic diseases such as diabetes, whereas exercise snacking can help keep your blood sugar levels steady.
Of course, longer-term studies are needed. But the evidence we do have suggests exercise snacking really helps.
Just a few short exercise sessions can do you a world of good. eggeegg/Shutterstock Why does any of this matter?
As you age, you lose strength and mass in the muscles you use to walk, or stand up. Everyday tasks can become a struggle.
All this contributes to disability, hospitalisation, chronic disease, and reliance on community and residential aged care support.
By preserving your muscle mass and strength, you can:
- reduce joint pain
- get on with activities you enjoy
- live independently in your own home
- delay or even eliminate the need for expensive health care or residential aged care.
What if I walk a lot – is that enough?
Walking may maintain some level of lower body muscle mass, but it won’t preserve your upper body muscles.
If you find it difficult to get out of a chair, or can only walk short distances without getting out of breath, resistance training is the best way to regain some of the independence and function you’ve lost.
It’s even more important for women, as muscle mass and strength are typically lower in older women than men. And if you’ve been diagnosed with osteoporosis, which is more common in older women than men, resistance exercise snacking at home can improve your balance, strength, and bone mineral density. All of this reduces the risk of falls and fractures.
You don’t need heavy weights or fancy equipment to benefit from resistance training.
So, will you start exercise snacking today?
Justin Keogh, Associate Dean of Research, Faculty of Health Sciences and Medicine, Bond University and Jackson Fyfe, Senior Lecturer, Strength and Conditioning Sciences, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: