12 Things Your Urine Says About Your Health (Test At Home)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Urine has been used to assess health since Ancient Egypt (fun fact: because of Egyptian language having multiple sounds that get transliterated to “a” in English, the condition of passing blood in one’s urine was known as “Aaaaa” ← this word has three syllables; “Aa-a-aa”).
Modern techniques are more advanced than those of times past (for example, diabetes is no longer diagnosed by a urine taste-test), but basic urine inspection is still a very useful indicator of many things. Recognizing changes in urine can even help detect life-threatening conditions early:
Traffic lights?
How urine works: water that we consume is absorbed into the bloodstream and filtered by the kidneys. Urine is essentially blood with actual the blood cells filtered out and/or broken down. The yellow color comes from urochrome, produced during red blood cell breakdown. Here’s how things can happen a little differently:
- Fluorescent yellow: caused by excess vitamin B2 from supplements; harmless.
- Red urine: can indicate blood (bladder cancer, UTIs), hemoglobin, or myoglobin; seek medical attention.
- Dark brown/tea-colored urine: may result from muscle damage or blood cell destruction; requires evaluation.
- Orange urine: caused by dehydration, medications, or liver/bile duct issues (if paired with pale stools).
- Purple urine: UTI bacteria produce pigments that can cause this; treatable with antibiotics.
- Green urine: rare; caused by medications or dyes like methylene blue.
- Frothy/foamy urine: indicates high protein levels, often from kidney damage (e.g. per diabetes and/or hypertension).
- Crystal-clear urine: suggests overhydration, which can dangerously lower sodium levels.
- Dark yellow/amber urine: may mean dehydration; drink more water to maintain a light yellow color.
- Not peeing enough: may indicate severe dehydration or kidney failure; urgent medical attention needed.
- Peeing too much: often linked to diabetes or excessive water intake; can lead to dehydration or low sodium.
- Color-changing urine: port wine color signals porphyria; black urine indicates alkaptonuria (oxidation of homogentisic acid). Both are serious.
Bonus: if you eat a lot of beetroot and then your urine is pink/red/purple, that’s probably just the pigments passing through. If it persists though, then of course, see above.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Why You Don’t Need 8 Glasses Of Water Per Day
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

16/8 Intermittent Fasting For Beginners

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Health Insider explains in super-simple fashion why and how to do Intermittent Fasting (IF), which is something that can sound complicated at first, but becomes very simple and easy once understood.
What do we need to know?
Intermittent fasting (IF) is a good, well-evidenced way to ease your body’s metabolic load, and
give your organs a chance to recover from the strain of digestion and its effects. That’s not just your gastrointestinal organs! It’s your pancreas and liver too, amongst others—this is about glucose metabolism as much as it is about digestion.This, in turn, allows your body some downtime to do its favorite thing, which is: maintenance!
This maintenance takes the form of enhanced cellular apoptosis and autophagy, helping to keep cells young and cancer-free.
In other words, with well-practised intermittent fasting, we can reduce our risk of metabolic disease (including heart disease and diabetes) as well as cancer and neurodegeneration.
You may be wondering: this sounds miraculous; what’s the catch? There are a couple:
- While fasting from food, the body’s enhanced metabolism requires more water, so you’ll need to take extra care keep on top of your hydration (this is one reason why Ramadan fasting, while healthy for most people, is not as healthy as IF—because Ramadan fasting means abstaining from water, too).
- If you are diabetic, and especially if you have Type 1 Diabetes, fasting may not be a safe option for you, since if you get a hypo in the middle of your fasting period, it’s obviously not a good idea to wait another many hours before fixing it.
Extra note on that last one: it’s easy to think “can’t I just lower my bolus insulin instead of eating?” and while superficially yes that will raise your blood sugar levels, it’s because the sugar will be sticking around in your blood, and not actually getting released into the organs that need it. So while your blood glucose monitor may say you’re fine, you will be starving your organs and if you keep it up they may suffer serious damage.
Disclaimer: our standard legal/medical disclaimer applies, and this is intended for educational purposes only; please do speak with your endocrinologist before changing anything you usually do with regard to your blood sugar maintenance.
Ok, back onto the cheerier topic at hand:
Aside from the above: for most people, IF is a remarkably healthful practice in very many ways.
For more on the science, practicalities, and things to do/avoid, enjoy this short (4:53) video:
Click Here If The Embedded Video Doesn’t Load Automatically
Want to know more?
Check out our previous main feature on this topic:
Intermittent Fasting: Mythbusting Edition
Enjoy!
Share This Post
-

Anti-Inflammatory Brownies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Brownies are usually full of sugar, butter, and flour. These ones aren’t! Instead, they’re full of fiber (good against inflammation), healthy fats, and anti-inflammatory polyphenols:
You will need
- 1 can chickpeas (keep half the chickpea water, also called aquafaba, as we’ll be using it)
- 4 oz of your favorite nut butter (substitute with tahini if you’re allergic to nuts)
- 3 oz rolled oats
- 2 oz dark chocolate chips (or if you want the best quality: dark chocolate, chopped into very small pieces)
- 3 tbsp of your preferred plant milk (this is an anti-inflammatory recipe and unfermented dairy is inflammatory)
- 2 tbsp cocoa powder (pure cacao is best)
- 1 tbsp glycine (if unavailable, use 2 tbsp maple syrup, and skip the aquafaba)
- 2 tsp vanilla extract
- ½ tsp baking powder
- ¼ tsp low-sodium salt
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 350℉ / 180℃, and line a 7″ cake tin with baking paper.
2) Blend the oats in a food processor, until you have oat flour.
3) Add all the remaining ingredients except the dark chocolate chips, and process until the mixture resembles cookie dough.
3) Transfer to a bowl, and fold in the dark chocolate chips, distributing evenly.
4) Add the mixture to the cake tin, and smooth the surface down so that it’s flat and even. Bake for about 25 minutes, and let them cool in the tin for at least 10 minutes, but longer is better, as they will firm up while they cool. Cut into cubes when ready to serve:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
- Cacao vs Carob – Which is Healthier?
- Keep Inflammation At Bay
- The Sweet Truth About Glycine
- The Best Kind Of Fiber For Overall Health?
Take care!
Share This Post
-

The first pig kidney has been transplanted into a living person. But we’re still a long way from solving organ shortages
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In a world first, we heard last week that US surgeons had transplanted a kidney from a gene-edited pig into a living human. News reports said the procedure was a breakthrough in xenotransplantation – when an organ, cells or tissues are transplanted from one species to another. https://www.youtube.com/embed/cisOFfBPZk0?wmode=transparent&start=0 The world’s first transplant of a gene-edited pig kidney into a live human was announced last week.
Champions of xenotransplantation regard it as the solution to organ shortages across the world. In December 2023, 1,445 people in Australia were on the waiting list for donor kidneys. In the United States, more than 89,000 are waiting for kidneys.
One biotech CEO says gene-edited pigs promise “an unlimited supply of transplantable organs”.
Not, everyone, though, is convinced transplanting animal organs into humans is really the answer to organ shortages, or even if it’s right to use organs from other animals this way.
There are two critical barriers to the procedure’s success: organ rejection and the transmission of animal viruses to recipients.
But in the past decade, a new platform and technique known as CRISPR/Cas9 – often shortened to CRISPR – has promised to mitigate these issues.
What is CRISPR?
CRISPR gene editing takes advantage of a system already found in nature. CRISPR’s “genetic scissors” evolved in bacteria and other microbes to help them fend off viruses. Their cellular machinery allows them to integrate and ultimately destroy viral DNA by cutting it.
In 2012, two teams of scientists discovered how to harness this bacterial immune system. This is made up of repeating arrays of DNA and associated proteins, known as “Cas” (CRISPR-associated) proteins.
When they used a particular Cas protein (Cas9) with a “guide RNA” made up of a singular molecule, they found they could program the CRISPR/Cas9 complex to break and repair DNA at precise locations as they desired. The system could even “knock in” new genes at the repair site.
In 2020, the two scientists leading these teams were awarded a Nobel prize for their work.
In the case of the latest xenotransplantation, CRISPR technology was used to edit 69 genes in the donor pig to inactivate viral genes, “humanise” the pig with human genes, and knock out harmful pig genes. https://www.youtube.com/embed/UKbrwPL3wXE?wmode=transparent&start=0 How does CRISPR work?
A busy time for gene-edited xenotransplantation
While CRISPR editing has brought new hope to the possibility of xenotransplantation, even recent trials show great caution is still warranted.
In 2022 and 2023, two patients with terminal heart diseases, who were ineligible for traditional heart transplants, were granted regulatory permission to receive a gene-edited pig heart. These pig hearts had ten genome edits to make them more suitable for transplanting into humans. However, both patients died within several weeks of the procedures.
Earlier this month, we heard a team of surgeons in China transplanted a gene-edited pig liver into a clinically dead man (with family consent). The liver functioned well up until the ten-day limit of the trial.
How is this latest example different?
The gene-edited pig kidney was transplanted into a relatively young, living, legally competent and consenting adult.
The total number of gene edits edits made to the donor pig is very high. The researchers report making 69 edits to inactivate viral genes, “humanise” the pig with human genes, and to knockout harmful pig genes.
Clearly, the race to transform these organs into viable products for transplantation is ramping up.
From biotech dream to clinical reality
Only a few months ago, CRISPR gene editing made its debut in mainstream medicine.
In November, drug regulators in the United Kingdom and US approved the world’s first CRISPR-based genome-editing therapy for human use – a treatment for life-threatening forms of sickle-cell disease.
The treatment, known as Casgevy, uses CRISPR/Cas-9 to edit the patient’s own blood (bone-marrow) stem cells. By disrupting the unhealthy gene that gives red blood cells their “sickle” shape, the aim is to produce red blood cells with a healthy spherical shape.
Although the treatment uses the patient’s own cells, the same underlying principle applies to recent clinical xenotransplants: unsuitable cellular materials may be edited to make them therapeutically beneficial in the patient.

CRISPR technology is aiming to restore diseased red blood cells to their healthy round shape. Sebastian Kaulitzki/Shutterstock We’ll be talking more about gene-editing
Medicine and gene technology regulators are increasingly asked to approve new experimental trials using gene editing and CRISPR.
However, neither xenotransplantation nor the therapeutic applications of this technology lead to changes to the genome that can be inherited.
For this to occur, CRISPR edits would need to be applied to the cells at the earliest stages of their life, such as to early-stage embryonic cells in vitro (in the lab).
In Australia, intentionally creating heritable alterations to the human genome is a criminal offence carrying 15 years’ imprisonment.
No jurisdiction in the world has laws that expressly permits heritable human genome editing. However, some countries lack specific regulations about the procedure.
Is this the future?
Even without creating inheritable gene changes, however, xenotransplantation using CRISPR is in its infancy.
For all the promise of the headlines, there is not yet one example of a stable xenotransplantation in a living human lasting beyond seven months.
While authorisation for this recent US transplant has been granted under the so-called “compassionate use” exemption, conventional clinical trials of pig-human xenotransplantation have yet to commence.
But the prospect of such trials would likely require significant improvements in current outcomes to gain regulatory approval in the US or elsewhere.
By the same token, regulatory approval of any “off-the-shelf” xenotransplantation organs, including gene-edited kidneys, would seem some way off.
Christopher Rudge, Law lecturer, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-

Missing Microbes – by Dr. Martin Blaser
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You probably know that antibiotic resistance is a problem, but you might not realize just what a many-headed beast antibiotic overuse is.
From growing antibiotic superbugs, to killing the friendly bacteria that normally keep pathogens down to harmless numbers (resulting in death of the host, as the pathogens multiply unopposed), to multiple levels of dangers in antibiotic overuse in the farming of animals, this book is scary enough that you might want to save it for Halloween.
But, Dr. Blaser does not argue against antibiotic use when it’s necessary; many people are alive because of antibiotics—he himself recovered from typhoid because of such.
The style of the book is narrative, but information-dense. It does not succumb to undue sensationalization, but it’s also far from being a dry textbook.
Bottom line: if you’d like to understand the real problems caused by antibiotics, and how we can combat that beyond merely “try not to take them unnecessarily”, this book is very worthy reading.
Click here to check out Missing Microbes, and learn more about yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A Statin-Free Life – by Dr. Aseem Malhotra
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Here at 10almonds, we’ve written before about the complexities of statins, and their different levels of risk/benefit for men and women, respectively. It’s a fascinating topic, and merits more than an article of the size we write here!
So, in the spirit of giving pointers of where to find a lot more information, this book is a fine choice.
Dr. Malhotra, a consultant cardiologist and professor of evidence-based medicine, talks genes and lifestyle, drugs and blood. He takes us on a tour of the very many risk factors for heart disease, and how cholesterol levels may be at best an indicator, but less likely a cause, of heart disease, especially for women. Further and even better, he discusses various more reliable indicators and potential causes, too.
Rather than be all doom and gloom, he does offer guidance on how to reduce each of one’s personal risk factors and—which is important—keep on top of the various relevant measures of heart health (including some less commonly tested ones, like the coronary calcium score).
The style is light reading andyet with a lot of reference to hard science, so it’s really the best of both worlds in that regard.
Bottom line: if you’re considering statins, or are on statins and are reconsidering that choice, then this book will (notwithstanding its own bias in its conclusion) help you make a more-informed decision.
Click here to check out A Statin-Free Life, and make the best choice for you!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

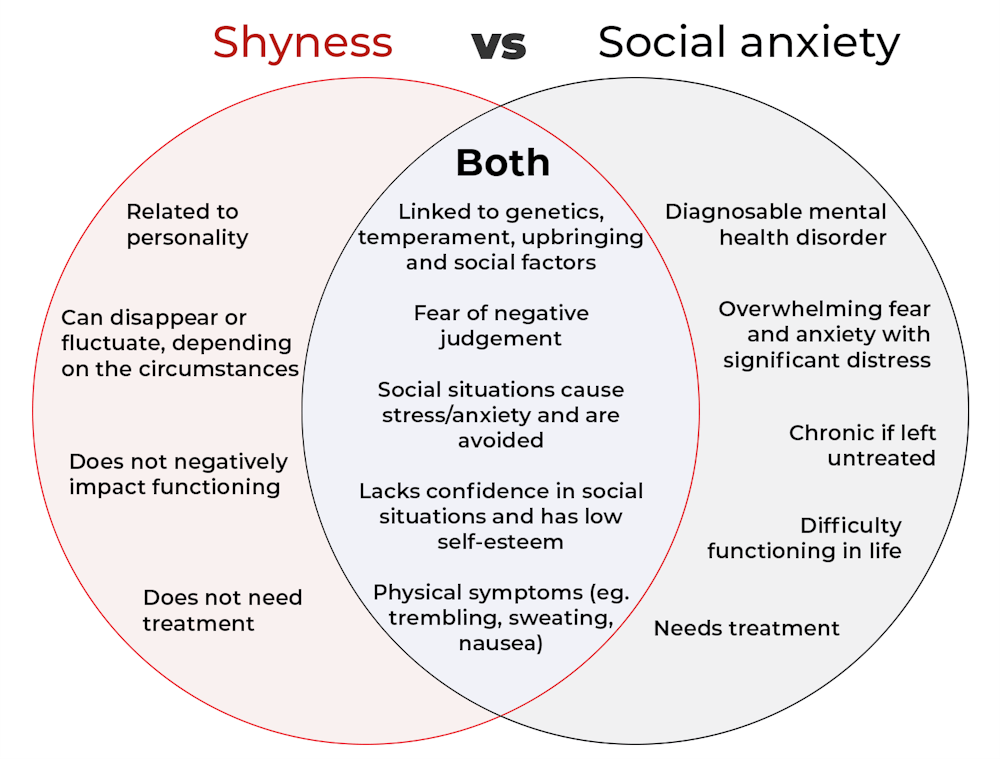
What’s the difference between shyness and social anxiety?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
The terms “shyness” and “social anxiety” are often used interchangeably because they both involve feeling uncomfortable in social situations.
However, feeling shy, or having a shy personality, is not the same as experiencing social anxiety (short for “social anxiety disorder”).
Here are some of the similarities and differences, and what the distinction means.
pathdoc/Shutterstock How are they similar?
It can be normal to feel nervous or even stressed in new social situations or when interacting with new people. And everyone differs in how comfortable they feel when interacting with others.
For people who are shy or socially anxious, social situations can be very uncomfortable, stressful or even threatening. There can be a strong desire to avoid these situations.
People who are shy or socially anxious may respond with “flight” (by withdrawing from the situation or avoiding it entirely), “freeze” (by detaching themselves or feeling disconnected from their body), or “fawn” (by trying to appease or placate others).
A complex interaction of biological and environmental factors is also thought to influence the development of shyness and social anxiety.
For example, both shy children and adults with social anxiety have neural circuits that respond strongly to stressful social situations, such as being excluded or left out.
People who are shy or socially anxious commonly report physical symptoms of stress in certain situations, or even when anticipating them. These include sweating, blushing, trembling, an increased heart rate or hyperventilation.
How are they different?
Social anxiety is a diagnosable mental health condition and is an example of an anxiety disorder.
For people who struggle with social anxiety, social situations – including social interactions, being observed and performing in front of others – trigger intense fear or anxiety about being judged, criticised or rejected.
To be diagnosed with social anxiety disorder, social anxiety needs to be persistent (lasting more than six months) and have a significant negative impact on important areas of life such as work, school, relationships, and identity or sense of self.
Many adults with social anxiety report feeling shy, timid and lacking in confidence when they were a child. However, not all shy children go on to develop social anxiety. Also, feeling shy does not necessarily mean a person meets the criteria for social anxiety disorder.
People vary in how shy or outgoing they are, depending on where they are, who they are with and how comfortable they feel in the situation. This is particularly true for children, who sometimes appear reserved and shy with strangers and peers, and outgoing with known and trusted adults.
Individual differences in temperament, personality traits, early childhood experiences, family upbringing and environment, and parenting style, can also influence the extent to which people feel shy across social situations.
Not all shy children go on to develop social anxiety. 249 Anurak/Shutterstock However, people with social anxiety have overwhelming fears about embarrassing themselves or being negatively judged by others; they experience these fears consistently and across multiple social situations.
The intensity of this fear or anxiety often leads people to avoid situations. If avoiding a situation is not possible, they may engage in safety behaviours, such as looking at their phone, wearing sunglasses or rehearsing conversation topics.
The effect social anxiety can have on a person’s life can be far-reaching. It may include low self-esteem, breakdown of friendships or romantic relationships, difficulties pursuing and progressing in a career, and dropping out of study.
The impact this has on a person’s ability to lead a meaningful and fulfilling life, and the distress this causes, differentiates social anxiety from shyness.
Children can show similar signs or symptoms of social anxiety to adults. But they may also feel upset and teary, irritable, have temper tantrums, cling to their parents, or refuse to speak in certain situations.
If left untreated, social anxiety can set children and young people up for a future of missed opportunities, so early intervention is key. With professional and parental support, patience and guidance, children can be taught strategies to overcome social anxiety.
Why does the distinction matter?
Social anxiety disorder is a mental health condition that persists for people who do not receive adequate support or treatment.
Without treatment, it can lead to difficulties in education and at work, and in developing meaningful relationships.
Receiving a diagnosis of social anxiety disorder can be validating for some people as it recognises the level of distress and that its impact is more intense than shyness.
A diagnosis can also be an important first step in accessing appropriate, evidence-based treatment.
Different people have different support needs. However, clinical practice guidelines recommend cognitive-behavioural therapy (a kind of psychological therapy that teaches people practical coping skills). This is often used with exposure therapy (a kind of psychological therapy that helps people face their fears by breaking them down into a series of step-by-step activities). This combination is effective in-person, online and in brief treatments.
Treatment is available online as well as in-person. ImYanis/Shutterstock For more support or further reading
Online resources about social anxiety include:
- This Way Up’s online program for managing excessive shyness and fear of social situations
- Beyond Blue’s resources on social anxiety
- a guide to looking after yourself if you have social anxiety, from the Western Australian health department
- social anxiety online program for children and teens from the University of Queensland
- inroads, a self-guided online program for young adults who drink alcohol to manage their anxiety.
We thank the Black Dog Institute Lived Experience Advisory Network members for providing feedback and input for this article and our research.
Kayla Steele, Postdoctoral research fellow and clinical psychologist, UNSW Sydney and Jill Newby, Professor, NHMRC Emerging Leader & Clinical Psychologist, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: