Women’s Strength Training Anatomy – by Frédéric Delavier
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fitness guides for women tend to differ from fitness guides for men, in the wrong ways:
“Do some squats and jumping jacks, and here’s a exercise for your abs; you too can look like our model here”
In those other books we are left wonder: where’s the underlying information? Where are the explanations that aren’t condescending? Where, dare we ask, is the understanding that a woman might ever lift something heavier than a baby?
Delavier, in contrast, delivers. With 130 pages of detailed anatomical diagrams for all kinds of exercises to genuinely craft your body the way you want it for you. Bigger here, smaller there, functional strength, you decide.
And rest assured: no, you won’t end up looking like Arnold Schwarzenegger unless you not only eat like him, but also have his genes (and possibly his, uh, “supplement” regime).
What you will get though, is a deep understanding of how to tailor your exercise routine to actually deliver the personalized and specific results that you want.
Pick Up Today’s Book on Amazon!
Not looking for a feminine figure? You may like the same author’s book for men:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Could the shingles vaccine lower your risk of dementia?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A recent study has suggested Shingrix, a relatively new vaccine given to protect older adults against shingles, may delay the onset of dementia.
This might seem like a bizarre link, but actually, research has previously shown an older version of the shingles vaccine, Zostavax, reduced the risk of dementia.
In this new study, published last week in the journal Nature Medicine, researchers from the United Kingdom found Shingrix delayed dementia onset by 17% compared with Zostavax.
So how did the researchers work this out, and how could a shingles vaccine affect dementia risk?

Melinda Nagy/Shutterstock From Zostavax to Shingrix
Shingles is a viral infection caused by the varicella-zoster virus. It causes painful rashes, and affects older people in particular.
Previously, Zostavax was used to vaccinate against shingles. It was administered as a single shot and provided good protection for about five years.
Shingrix has been developed based on a newer vaccine technology, and is thought to offer stronger and longer-lasting protection. Given in two doses, it’s now the preferred option for shingles vaccination in Australia and elsewhere.
In November 2023, Shingrix replaced Zostavax on the National Immunisation Program, making it available for free to those at highest risk of complications from shingles. This includes all adults aged 65 and over, First Nations people aged 50 and older, and younger adults with certain medical conditions that affect their immune systems.
What the study found
Shingrix was approved by the US Food and Drugs Administration in October 2017. The researchers in the new study used the transition from Zostavax to Shingrix in the United States as an opportunity for research.
They selected 103,837 people who received Zostavax (between October 2014 and September 2017) and compared them with 103,837 people who received Shingrix (between November 2017 and October 2020).
By analysing data from electronic health records, they found people who received Shingrix had a 17% increase in “diagnosis-free time” during the follow-up period (up to six years after vaccination) compared with those who received Zostavax. This was equivalent to an average of 164 extra days without a dementia diagnosis.
The researchers also compared the shingles vaccines to other vaccines: influenza, and a combined vaccine for tetanus, diphtheria and pertussis. Shingrix and Zostavax performed around 14–27% better in lowering the risk of a dementia diagnosis, with Shingrix associated with a greater improvement.
The benefits of Shingrix in terms of dementia risk were significant for both sexes, but more pronounced for women. This is not entirely surprising, because we know women have a higher risk of developing dementia due to interplay of biological factors. These include being more sensitive to certain genetic mutations associated with dementia and hormonal differences.
Why the link?
The idea that vaccination against viral infection can lower the risk of dementia has been around for more than two decades. Associations have been observed between vaccines, such as those for diphtheria, tetanus, polio and influenza, and subsequent dementia risk.
Research has shown Zostavax vaccination can reduce the risk of developing dementia by 20% compared with people who are unvaccinated.
But it may not be that the vaccines themselves protect against dementia. Rather, it may be the resulting lack of viral infection creating this effect. Research indicates bacterial infections in the gut, as well as viral infections, are associated with a higher risk of dementia.
Notably, untreated infections with herpes simplex (herpes) virus – closely related to the varicella-zoster virus that causes shingles – can significantly increase the risk of developing dementia. Research has also shown shingles increases the risk of a later dementia diagnosis.
This isn’t the first time research has suggested a vaccine could reduce dementia risk. ben bryant/Shutterstock The mechanism is not entirely clear. But there are two potential pathways which may help us understand why infections could increase the risk of dementia.
First, certain molecules are produced when a baby is developing in the womb to help with the body’s development. These molecules have the potential to cause inflammation and accelerate ageing, so the production of these molecules is silenced around birth. However, viral infections such as shingles can reactivate the production of these molecules in adult life which could hypothetically lead to dementia.
Second, in Alzheimer’s disease, a specific protein called Amyloid-β go rogue and kill brain cells. Certain proteins produced by viruses such as COVID and bad gut bacteria have the potential to support Amyloid-β in its toxic form. In laboratory conditions, these proteins have been shown to accelerate the onset of dementia.
What does this all mean?
With an ageing population, the burden of dementia is only likely to become greater in the years to come. There’s a lot more we have to learn about the causes of the disease and what we can potentially do to prevent and treat it.
This new study has some limitations. For example, time without a diagnosis doesn’t necessarily mean time without disease. Some people may have underlying disease with delayed diagnosis.
This research indicates Shingrix could have a silent benefit, but it’s too early to suggest we can use antiviral vaccines to prevent dementia.
Overall, we need more research exploring in greater detail how infections are linked with dementia. This will help us understand the root causes of dementia and design potential therapies.
Ibrahim Javed, Enterprise and NHMRC Emerging Leadership Fellow, UniSA Clinical & Health Sciences, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Are You A Calorie-Burning Machine?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Burn, Calorie, Burn

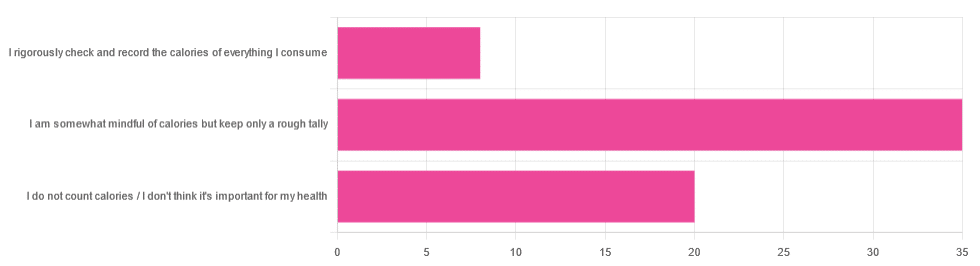
In Tuesday’s newsletter, we asked you whether you count calories, and got the above-depicted, below-described set of answers:
- About 56% said “I am somewhat mindful of calories but keep only a rough tally”
- About 32% said “I do not count calories / I don’t think it’s important for my health”
- About 13% said “I rigorously check and record the calories of everything I consume”
So what does the science say, about the merits of all these positions?
A food’s calorie count is a good measure of how much energy we will, upon consuming the food, have to use or store: True or False?
False, broadly. It can be, at best, a rough guideline. Do you know what a calorie actually is, by the way? Most people don’t.
One thing to know before we get to that: there’s “cal” vs “kcal”. The latter is generally used when it comes to foodstuffs, and it’s what we’ll be meaning whenever we say “calorie” here. 1cal is 1/1000th of a kcal, that’s all.
Now, for what a calorie actually is:
A calorie is the amount of energy needed to raise the temperature of 1 liter of water by 1℃
Question: so, how to we measure how much food is needed to do that?
Answer: by using a bomb calorimeter! Which is the exciting name for the apparatus used to literally burn food and capture the heat produced to indeed raise the temperature of 1 liter of water by 1℃.
If you’re having trouble imagining such equipment, here it is:
Bomb Calorimeter: Definition, Construction, & Operation (with diagram and FAQs)
The unfortunate implication of the above information
A kilogram of sawdust contains about a 1000 kcal, give or take what wood was used and various other conditions.
However, that does not mean you can usefully eat the sawdust. In other words:
Calorie count tells us only how good something is at raising the temperature of water if physically burned.
Now do you see why oils and sugars have such comparably high calorie counts?
And while we may talk about “burning calories” as a metaphor, we do not, in fact, have a little wood stove inside us burning the food we eat.
A calorie is a calorie: True or False?
Definitely False! Building on from the above… We will get very little energy from sawdust; it’s not just that we can’t use it; we can’t store it either; it’ll mostly pass through as fiber.
(however, please do not use sawdust to get your daily dose of fiber either, as it is not safe for human consumption and may give you diseases, depending on what is lurking in it)
But let’s look at oil and sugar, two very high-calorie categories of food, because they’re really easy to physically burn and they give off a good flame.
A bomb calorimeter may treat them quite equally, but to our body, they are metabolically very different indeed.
For a start, most sugars will get absorbed and processed much more quickly than most oils, and that can overwhelm the liver (responsible for glycogen management), and lead to non-alcoholic fatty liver disease, diabetes, and more. Metabolic syndrome in general, and if you keep it up too much and you may find it’s now a lottery between dying of NAFLD, diabetes, or heart disease (it’ll usually be the heart disease that kills).
See also:
- Which Sugars Are Healthier, And Which Are Just The Same?
- 10 Ways To Balance Blood Sugars
- How To Unfatty A Fatty Liver
Meanwhile, we know all about the different kinds of nutritional profiles that oils can have, and some can promote having high energy without putting on fat, while others can strain the heart. Not even “a fat is a fat”, so “a calorie is a calorie” doesn’t get much mileage outside of a bomb calorimeter!
See also:
A calorie-controlled / calorie-restricted diet is an effective weight loss strategy: True or False?
True, usually! Surprise!
- On the one hand: calories are a wildly imprecise way to reckon the value of food, and using them as a guide to health can be dangerously misleading
- On the other hand: the very activity of calorie-counting itself promotes mindful eating, which is very good for the health
There is a strong difference between the mind of somebody who is carefully logging their pre-bedtime piece of chocolate and reflecting on its nutritional value, vs someone who isn’t sure whether this is their second or third glass of wine, nor how much the glass contained.
So if you want to get most of the benefits of a calorie-controlled diet without counting calories, you may try taking a “mindful eating” approach to diet.
However! If you want to do this for weight loss, be aware, that you will have to practice it all the time, not just for one meal here and there.
You can read more on how to do “mindful eating” here:
Dr. Rupy Aujla: The Kitchen Doctor | Mindful Eating & Interoception
Take care!
Share This Post
-

“Slugging” Skin Care Routine (Tips From A Dermatologist)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dermatologist Dr. Jenny Liu weighs in with advice!
Sometimes simplest is best
Slugging is a skincare trend involving applying petrolatum (e.g. Vaseline) as the final step to lock in hydration and repair the skin barrier. It’s particularly useful for dry, sensitive, or eczema-prone skin, and/or damaged skin barriers from overuse of actives or harsh conditions.
How it works: the waterproof layer reduces water loss (up to 99%) and facilitates repair the skin barrier. Thus, it indirectly hydrates the skin, supports natural exfoliation, and reduces fine lines. Best of all, it’s non-irritating, non-comedogenic, and safe for all skin types.
How to do it:
- Cleanse thoroughly to remove makeup and impurities.
- Apply a moisturizer or serum with humectants (e.g. glycerin, hyaluronic acid).
- Seal with petrolatum (e.g. Vaseline or similar).
- Skip areas with stronger active ingredients (e.g. retinoids) and active acne areas.
- Apply 30–60 minutes before bed to reduce product transfer.
- Use a gentle cleanser in the morning to remove residue.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Castor Oil: All-Purpose Life-Changer, Or Snake Oil? ← skincare is one of the things it definitely does work well for, and can be used for slugging also.
Take care!
Share This Post




Related Posts
-
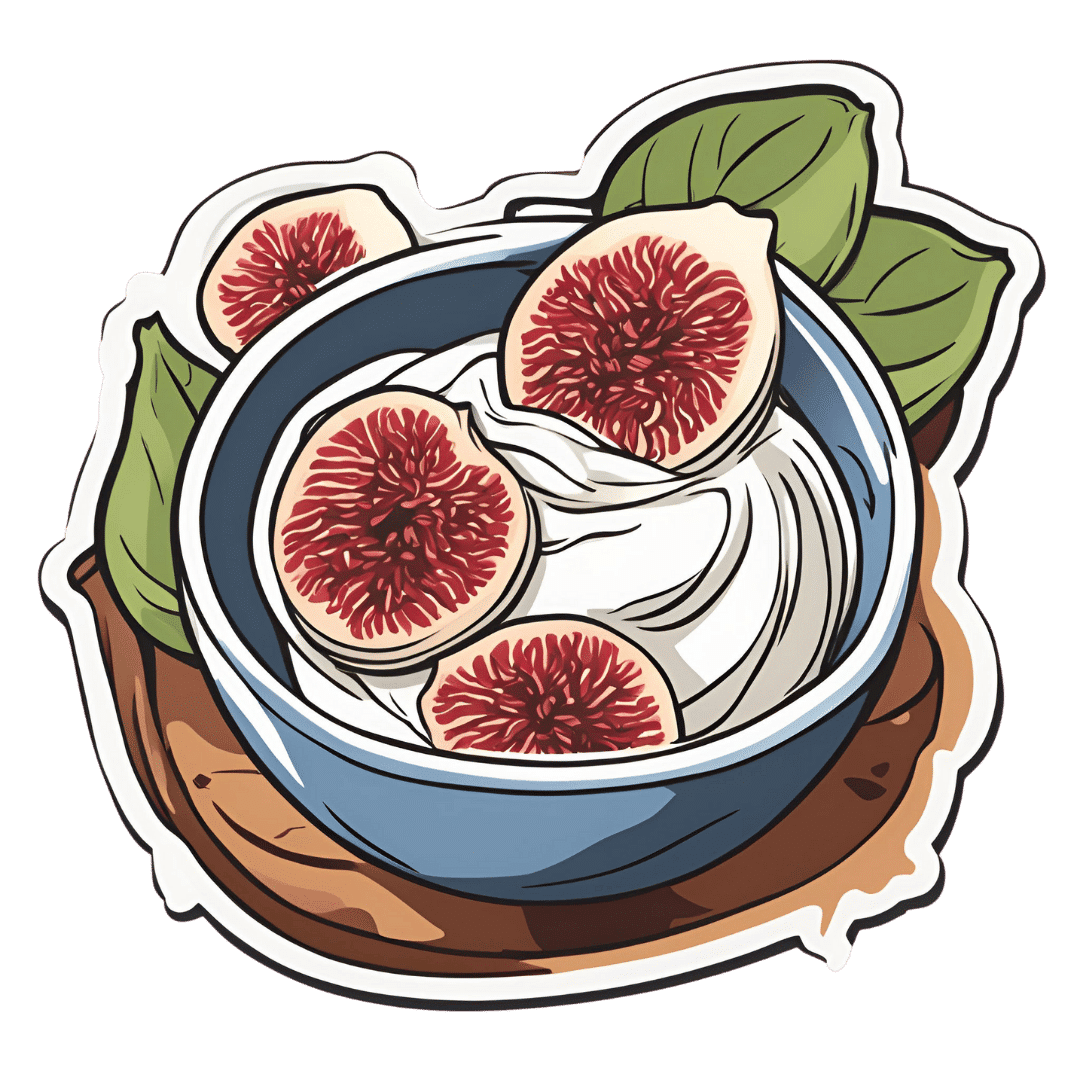
The Gut-Healthiest Yogurt
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Not only is this yogurt, so it’s winning from the start with its probiotic goodness, but also it’s full of several kinds of fiber, and gut-healthy polyphenols too. Plus, it’s delicious. The perfect breakfast, but don’t let us stop you from enjoying it at any time of day!
You will need
- 1 cup yogurt with minimal additives. Live Greek yogurt is a top-tier choice, and plant-based varieties are fine too (just watch out, again, for needless additives)
- 7 dried figs, roughly chopped
- 6 fresh figs, thinly sliced
- 5 oz chopped pitted dates
- 4 tbsp mixed seeds (pumpkin, sunflower, and chia are a great combination)
Method
(we suggest you read everything at least once before doing anything)
1) Soak the dried figs, the dates, and half the seeds in hot water for at least 5 minutes. Drain (be careful not to lose the chia seeds) and put in a blender with ¼ cup cold water.
2) Blend the ingredients from the last step into a purée (you can add a little more cold water if it needs it).
3) Mix this purée into the yogurt in a bowl, and add in the remaining seeds, mixing them in thoroughly.
4) Top with the sliced figs, and serve (or refrigerate, up to a few days, until needed).

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Making Friends With Your Gut (You Can Thank Us Later)
- Dates vs Figs – Which is Healthier?
- The Tiniest Seeds With The Most Value
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Demystifying Cholesterol
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
All About Cholesterol
When it comes to cholesterol, the most common lay understanding (especially under a certain age) is “it’s bad”.
A more informed view (and more common after a certain age) is “LDL cholesterol is bad; HDL cholesterol is good”.
A more nuanced view is “LDL cholesterol is established as significantly associated with (and almost certainly a causal factor of) atherosclerotic cardiovascular disease and related mortality in men; in women it is less strongly associated and may or may not be a causal factor”
You can read more about that here:
Statins: His & Hers? ← we highly recommend reading this, especially if you are a woman and/or considering/taking statins. To be clear, we’re not saying “don’t take statins!”, because they might be the right medical choice for you and we’re not your doctors. But we are saying: here’s something to at least know about and consider.
Beyond HDL & LDL
There is also VLDL cholesterol, which as you might have guessed, stands for “very low-density lipoprotein”. It has a high, unhealthy triglyceride content, and it increases atherosclerotic plaque. In other words, it hardens your arteries more quickly.
The term “hardening the arteries” is an insufficient descriptor of what’s happening though, because while yes it is hardening the arteries, it’s also narrowing them. Because minerals and detritus passing through in the blood (the latter sounds bad, but there is supposed to be detritus passing through in the blood; it’s got to get out of the body somehow, and it’s off to get filtered and excreted) get stuck in the cholesterol (which itself is a waxy substance, by the way) and before you know it, those minerals and other things have become a solid part of the interior of your artery wall, like a little plastering team came and slapped plaster on the inside of the walls, then when it hardened, slapped more plaster on, and so on. Macrophages (normally the body’s best interior clean-up team) can’t eat things much bigger than themselves, so that means they can’t tackle the build-up of plaque.
Impact on the heart
Narrower less flexible arteries means very poor circulation, which means that organs can start having problems, which obviously includes your heart itself as it is not only having to do a harder job to keep the blood circulating through the narrower blood vessels, but also, it is not immune to also being starved of oxygen and nutrients along with the rest of the body when the circulation isn’t good enough. It’s a catch 22.
What if LDL is low and someone is getting heart disease anyway?
That’s often a case of apolipoprotein B, and unlike lipoprotein A, which is bound to LDL so usually* isn’t a problem if LDL is in “safe” ranges, Apo-B can more often cause problems even when LDL is low. Neither of these are tested for in most standard cholesterol tests by the way, so you might have to ask for them.
*Some people, around 1 in 20 people, have hereditary extra risk factors for this.
What to do about it?
Well, get those lipids tests! Including asking for the LpA and Apo-B tests, especially if you have a history of heart disease in your family, or otherwise know you have a genetic risk factor.
With or without extra genetic risks, it’s good to get lipids tests done annually from 40 onwards (earlier, if you have extra risk factors).
See also: Understanding your cholesterol numbers
Wondering whether you have an increased genetic risk or not?
Genetic Testing: Health Benefits & Methods ← we think this is worth doing; it’s a “one-off test tells many useful things”. Usually done from a saliva sample, but some companies arrange a blood draw instead. Cost is usually quite affordable; do shop around, though.
Additionally, talk to your pharmacist to check whether any of your meds have contraindications or interactions you should be aware of in this regard. Pharmacists usually know contraindications/interactions stuff better than doctors, and/but unlike doctors, they don’t have social pressure on them to know everything, which means that if they’re not sure, instead of just guessing and reassuring you in a confident voice, they’ll actually check.
Lastly, shocking nobody, all the usual lifestyle medicine advice applies here, especially get plenty of moderate exercise and eat a good diet, preferably mostly if not entirely plant-based, and go easy on the saturated fat.
Note: while a vegan diet contains zero dietary cholesterol (because plants don’t make it), vegans can still get unhealthy blood lipid levels, because we are animals and—like most animals—our body is perfectly capable of making its own cholesterol (indeed, we do need some cholesterol to function), and it can make its own in the wrong balance, if for example we go too heavy on certain kinds of (yes, even some plant-based) saturated fat.
Read more: Can Saturated Fats Be Healthy? ← see for example how palm oil and coconut oil are both plant-based, and both high in saturated fat, but palm oil’s is heart-unhealthy on balance, while coconut oil’s is heart-healthy on balance (in moderation).
Want to know more about your personal risk?
Try the American College of Cardiology’s ASCVD risk estimator (it’s free)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Pregnant women can now get a free RSV shot. What other vaccines do you need when you’re expecting?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From today, February 3, pregnant women in Australia will be eligible for a free RSV vaccine under the National Immunisation Program.
This vaccine is designed to protect young infants from severe RSV (respiratory syncytial virus). It does so by generating the production of antibodies against RSV in the mother, which then travel across the placenta to the baby.
While the RSV vaccine is a new addition to the National Immunisation Program, it’s one of three vaccines provided free for pregnant women under the program, alongside ones for influenza and whooping cough. Each offers important protection for newborn babies.
voronaman/Shutterstock The RSV vaccine
RSV is the most common cause of lower respiratory infections (bronchiolitis and pneumonia) in infants. It’s estimated that of every 100 infants born in Australia each year, at least two will be hospitalised with RSV by six months of age.
RSV infection is most common roughly between March and August in the southern hemisphere, but infection can occur year-round, especially in tropical areas.
The vaccine works by conferring passive immunity (from the mother) as opposed to active immunity (the baby’s own immune response). By the time the baby is born, their antibodies are sufficient to protect them during the first months of life when they are most vulnerable to severe RSV disease.
The RSV vaccine registered for use in pregnant women in Australia, Abrysvo, has been used since 2023 in the Americas and Europe. Real-world experience there shows it’s working well.
For example, over the 2024 RSV season in Argentina, it was found to prevent 72.7% of lower respiratory tract infections caused by RSV and requiring hospitalisation in infants aged 0–3 months, and 68% among those aged 0–6 months. This research noted three deaths from RSV, all in infants whose mothers did not receive the RSV vaccine during pregnancy.
This was similar to protection seen in a large multinational clinical trial that compared babies born to mothers who received this RSV vaccine with babies born to mothers who received a placebo. This study found the vaccine prevented 82.4% of severe cases of RSV in infants aged under three months, and 70% under six months, and that the vaccine was safe.
Vaccinating mothers during pregnancy protects the newborn baby. StoryTime Studio/Shutterstock In addition to the maternal vaccine, nirsevimab, a long-acting monoclonal antibody, provides effective protection against severe RSV disease. It’s delivered to the baby by an intramuscular injection, usually in the thigh.
Nirsevimab is recommended for babies born to women who did not receive an RSV vaccine during pregnancy, or who are born within two weeks of their mother having received the shot (most likely if they’re born prematurely). It may also be recommended for babies who are at higher risk of RSV due to a medical condition, even if their mother was vaccinated.
Nirsevimab is not funded under the National Immunisation Program, but is covered under various state and territory-based programs for infants of mothers who fall into the above categories.
But now we have a safe and effective RSV vaccine for pregnancy, all pregnant women should be encouraged to receive it as the first line of prevention. This will maximise the number of babies protected during their first months of life.
Flu and whooping cough
It’s also important pregnant women continue to receive flu and whooping cough vaccines in 2025. Like the RSV vaccine, these protect infants by passing antibodies from mother to baby.
There has been a large whooping cough outbreak in Australia in recent months, including a death of a two-month-old infant in Queensland in November 2024.
The whooping cough vaccine, given in combination with diphtheria and tetanus, prevents more than 90% of whooping cough cases in babies too young to receive their first whooping cough vaccine dose.
Similarly, influenza can be deadly in young babies, and maternal flu vaccination substantially reduces hospital visits associated with influenza for babies under six months. Flu can also be serious for pregnant women, so the vaccine offers important protection for the mother as well.
COVID vaccines are safe in pregnancy, but unless a woman is otherwise eligible, they’re not routinely recommended. You can discuss this with your health-care provider.
When and where can you get vaccinated?
Pregnant women can receive these vaccines during antenatal visits through their GP or in a specialised antenatal clinic.
The flu vaccine is recommended at any time during pregnancy, the whooping cough vaccine from 20 weeks (ideally before 32 weeks), and the RSV vaccine from 28 weeks (before 36 weeks).
It’s safe to receive multiple vaccinations at the same clinic visit.
The RSV vaccine is now available for pregnant women under the National Immunisation Program. Olga Rolenko/Shutterstock We know vaccination rates have declined in a variety of groups since the pandemic, and there’s evidence emerging that suggests this trend has occurred in pregnant women too.
A recent preprint (a study yet to be peer-reviewed) found a decrease of nearly ten percentage points in flu vaccine coverage among pregnant women in New South Wales, from 58.8% in 2020 to 49.1% in 2022. The research showed a smaller drop of 1.4 percentage points for whooping cough, from 79% in 2020 to 77.6% in 2022.
It’s important to work to improve vaccination rates during pregnancy to give babies the best protection in their first months of life.
We know pregnant women would like to receive information about new and routine maternal vaccines early in pregnancy. In particular, many pregnant women want to understand how vaccines are tested for safety, and their effectiveness, which was evident during COVID.
GPs and midwives are trusted sources of information on vaccines in pregnancy. There’s also information available online on Sharing Knowledge About Immunisation, a collaboration led by the National Centre for Immunisation Research and Surveillance.
Archana Koirala, Paediatrician and Infectious Diseases Specialist, University of Sydney; Bianca Middleton, Senior Research Fellow, Menzies School of Health Research; Margie Danchin, Professor of Paediatrics and vaccinologist, Royal Childrens Hospital, University of Melbourne and Murdoch Childrens Research Institute (MCRI); Associate Dean International, University of Melbourne, Murdoch Children’s Research Institute; Peter McIntyre, Professor in Women’s and Children’s Health, University of Otago, and Rebecca Doyle, Adjunct Research Fellow, School of Nursing, Midwifery and Social Work, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: