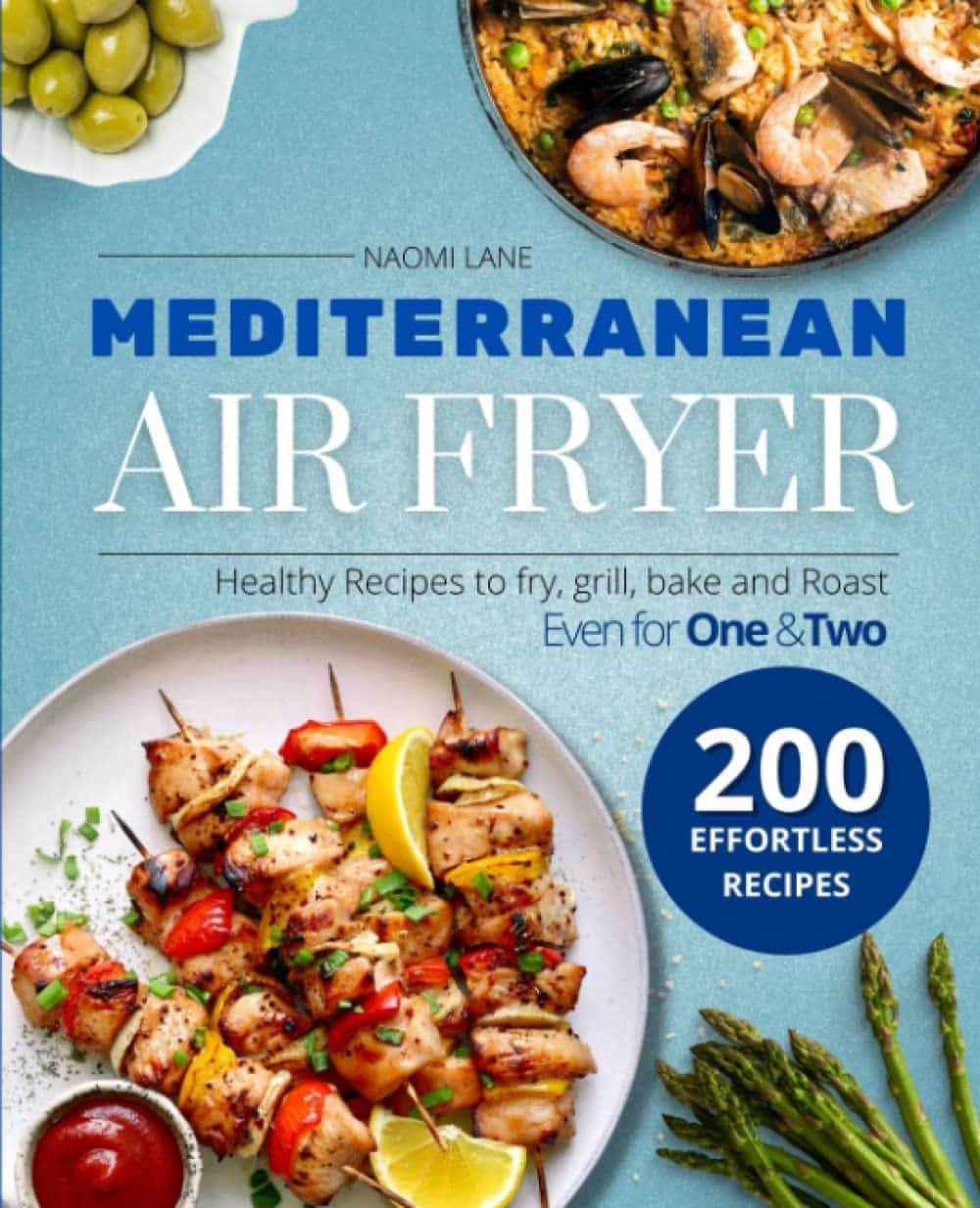
Mediterranean Air Fryer Cookbook – by Naomi Lane
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are Mediterranean Diet cookbooks, and there are air fryer cookbooks. And then there are (a surprisingly large intersection of!) Mediterranean Diet air fryer cookbooks. We wanted to feature one of them in today’s newsletter… And as part of the selection process, looked through quite a stack of them, and honestly, were quite disappointed with many. This one, however, was one of the ones that stood out for its quality of both content and clarity, and after a more thorough reading, we now present it to you:
Naomi Lane is a professional dietician, chef, recipe developer, and food writer… And it shows, on all counts.
She covers what the Mediterranean diet is, and she covers far more than this reviewer knew it was even possible to know about the use of an air fryer. That alone would make the book a worthy purchase already.
The bulk of the book is the promised 200 recipes. They cover assorted dietary requirements (gluten-free, dairy-free, etc) while keeping to the Mediterranean Diet.
The recipes are super clear, just what you need to know, no reading through a nostalgic storytime first to find things. Also no pictures, which will be a plus for some readers and a minus for others. The recipes also come complete with nutritional information for each meal (including sodium), so you don’t have to do your own calculations!
Bottom line: this is the Mediterranean Diet air fryer cook book. Get it, thank us later!
Get your copy of “Mediterranean Air Fryer Cookbook” on Amazon today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How to Stay Sane – by Philippa Perry

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this book is not: a guide of “how to stay sane” in the popular use of the word “sane”, meaning free from serious mental illness of all and any kinds in general, and especially free from psychotic delusions. Alas, this book will not help with those.
What, then, is it? A guide of “how to stay sane” in the more casual sense of resiliently and adaptively managing stress, anxiety, and suchlike. The “light end” of mental health struggles, that nonetheless may not always feel light when dealing with them.
The author, a psychotherapist, draws from her professional experience and training to lay out psychological tools for our use, as well as giving the reader a broader understanding of the most common ills that may ail us.
The writing style is relaxed and personable; it’s not at all like reading a textbook.
The psychotherapeutic style is not tied to one model, and rather hops from one to another, per what is most likely to help for a given thing. This is, in this reviewer’s opinion at least, far better than the (all-too common) attempt made by a lot of writers to try to present their personal favorite model as the cure for all ills, instead of embracing the whole toolbox as this one does.
Bottom line: if your mental health is anywhere between “mostly good” and “a little frayed around the edges but hanging on by at least a few threads”, then this book likely can help you gain/maintain the surer foundation you’re surely seeking.
Share This Post
-

Spoon-Fed – by Dr. Tim Spector
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Spector looks at widespread beliefs about food, and where those often scientifically disproven beliefs come from. Hint, there’s usually some manner of “follow the money”.
From calorie-counting to cholesterol content, from fish to bottled water, to why of all the people who self-report having an allergy, only around half turn out to actually have one when tested, Dr. Spector sets the record straight.
The style is as very down-to-earth and not at all self-aggrandizing; the author acknowledges his own mistakes and limitations along the way. In terms of pushing any particular agenda, his only agenda is clear: inform the public about bad science, so that we demand better science going forwards. Along the way, he gives us lots of information that can inform our personal health choices based on better science than indiscriminate headlines wildly (and sometimes intentionally) misinterpreting results.
Read this book, and you may find yourself clicking through to read the studies for yourself, next time you see a bold headline.
Bottom line: this book looks at a lot of what’s wrong with what a lot of people believe about healthy eating. Regular 10almonds readers might not find a lot that’s new here, but it could be a great gift for a would-be health-conscious friend or relative
Share This Post
-

Fermenting Everything – by Andy Hamilton
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is not justanother pickling book! This is, instead, what it says on the front cover, “fermenting everything”.
Ok, maybe not literally everything, but every kind of thing that can reasonably be fermented, and it’s probably a lot more things than you might think.
From habanero chutney to lacto-lemonade, aioli to kombucha, Ukrainian fermented tomatoes to kvass. We could go on, but we’d soon run out of space. You get the idea. If it’s a fermented product (food, drink, condiment) and you’ve heard of it, there’s probably a recipe in here.
All in all, this is a great way to get in your gut-healthy daily dose of fermented products!
He does also talk safety, and troubleshooting too. And so long as you have a collection of big jars and a fairly normally-furnished kitchen, you shouldn’t need any more special equipment than that, unless you decide to you your fermentation skills for making beer (which does need some extra equipment, and he offers advice on that—our advice as a health science publication is “don’t drink beer”, though).
Bottom line: with this in hand, you can create a lot of amazing foods/drinks/condiments that are not only delicious, but also great for gut health.
Click here to check out Fermenting Everything, and widen your culinary horizons!
Share This Post

-

Boundary-Setting Beyond “No”
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More Than A “No”
A lot of people struggle with boundary-setting, and it’s not always the way you might think.
The person who “can’t say no” to people probably comes to mind, but the problem is more far-reaching than that, and it’s rooted in not being clear over what a boundary actually is.
For example: “Don’t bring him here again!”
Pretty clear, right?
And while it is indeed clear, it’s not a boundary; it’s a command. Which may or may not be obeyed, and at the end of the day, what right have we to command people in general?
Same goes for less dramatic things like “Don’t talk to me about xyz”, which can still be important or trivial, depending on whether the topic of xyz is deeply traumatizing for you, or mildly annoying, or something else entirely.
Why this becomes a problem
It becomes a problem not because of any lack of clarity about your wishes, but rather, because it opens the floor for a debate. The listener may be given to wonder whether your right to not experience xyz is greater or lesser than their right to do/say/etc xyz.
“My right to swing my fist ends where someone else’s nose begins”
…does not help here, firstly because both sides will believe themself (or nobody) to be the injured party; for the fist-swinger, the other person’s nose made a vicious assault on their freedom. Or secondly, maybe there was some higher principle at stake; a reason why violence was justified. And then ten levels of philosophical debate. We see this a lot when it comes to freedom of expression, and vigorous debate over whether this entails freedom from social consequences of one’s words/actions.
How a good boundary-setting works (if this, then that)
Consider two signs:
- No trespassing!
- Trespassers will be shot!
Superficially, the second just seems like a more violent rendition of the first. But in fact, the second is more informationally useful: it explains what will happen if the boundary is not respected, and allows the reader to make their own informed decision with regard to what to do with that information.
We can employ this method (and can even do so gently, if we so wish and hopefully we mostly do wish to be gentle) when it comes to social and interpersonal boundary-setting:
- If you bring him here again, I will refuse you entrance
- If you bring up that topic again, I will ask you to leave
- If you do that, I will never speak to you again
- If you don’t stop drinking, I will divorce you
This “if-this-then-that” model does the very first thing that any good boundary does: make itself clear.
It doesn’t rely on moral arguments; it doesn’t invite debate. For example in that last case, it doesn’t argue that the partner doesn’t have the right to drink—it simply expresses what the speaker will exercise their own right to do, in that eventuality.
(as an aside, the situation that occurs when one is enmeshed with someone who is dependent on a substance is a complex topic, and if you’re interested in that, check out: Codependency Isn’t What Most People Think)
Back on track: boundary-setting is not about what’s right or good—it’s about nothing more nor less than a clear delineation between what we will and won’t accept, and how we’ll enforce that.
We can also, in particularly personal boundary-setting (such as with sexual boundaries’ oft-claimed “gray areas”), fix an improperly-set boundary that forgot to do the above, e.g:
“How about [proposition]?”
“No thank you” ← casually worded answer; contextually reasonable, and yet not a clear boundary per what we discussed above
“Come on, I think you’d like it”
“I said no. No means no. Ask me again and I will [consequences that are appropriate and actionable]”What’s “appropriate and actionable” may vary a lot from one situation to another, but it’s important that it’s something you can do and are prepared to do and will do if the condition for doing it is met.
Anything less than that is not a boundary—it’s just a request.
Note: this does not require that we have power, by the way. If we have zero power in a situation, well, that definitely sucks, but even then we can still express what is actionable, e.g. “I will never trust you again”.
“Price of entry”
You may have wondered, upon reading “boundary-setting is not about what’s right or good—it’s about nothing more nor less than a clear delineation between what we will and won’t accept, and how we’ll enforce that”, can’t that be used to control and manipulate people, essentially coercing them to do or not do things with the threat of consequences (specifically: bad ones)?
And the answer is: yes, yes it can.
But that’s where the flipside comes into play—the other person gets to set their boundaries, too.
For all of us, if we have any boundaries at all, there is a “price of entry” and all who want to be in our lives, or be close to us, have to decide for themselves whether that price of entry is worth it.
- If a person says “do not talk about topic xyz to me or I will leave”, that is a price of entry for being close to them.
- If you are passionate about talking about topic xyz to the point that you are unwilling to shelve it when in their presence, then that is the price of entry for being close to you.
- If one or more of you is not willing to pay the price of entry, then guess what, you’re just not going to be close.
In cases of forced proximity (e.g. workplaces or families) this is likely to get resolved by the workplace’s own rules (i.e. the price of entry that you agreed to when signing a contract to work there), and if something like that doesn’t exist (such as in families), well, that forced proximity is going to reach a breaking point, and somebody may discover it wasn’t enforceable after all.
See also: Family Estrangement: More Common Than Most People Think
…which also details how to fix it, where possible.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The High-Protein, High-Fiber Superfood Salad You’ll Want To Enjoy Daily
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This salad from Nisha Vora at Rainbow Plant Life has 30g protein and takes minutes to prepare, while being tasty enough to look forward to eating each day:
Easy preparation
Prepare the toppings first; you can do a week’s in advance at once:
- Roasted chickpeas:
- Drain, rinse, and dry two cans of chickpeas.
- Toss with olive oil, salt, and pepper.
- Roast at 425°F for 30–35 minutes.
- Roasted walnuts:
- Chop and toss with olive oil, salt, and pepper.
- Roast at 350°F for 12 minutes after chickpeas finish.
As for the salad base:
- Kale:
- Remove tough stems, slice thinly.
- Wash and massage with lemon juice and salt to soften.
- Cabbage:
- Slice thinly with a knife or mandolin.
- Store in a sealed bag in the fridge for up to a week.
Red wine vinaigrette dressing:
- Key ingredients: red wine vinegar, lemon juice, red pepper flakes, garlic, olive oil.
- Can be stored in the fridge for up to 10 days.
Putting it all together:
- Toss kale and cabbage with vinaigrette by hand.
- Add roasted chickpeas and walnuts for crunch.
- Include a protein source like tofu (store-bought curry tofu recommended).
- Mix in fresh vegetables like grated carrots, sliced bell peppers, or beets.
- Add extras like sauerkraut, avocado, pickled onions, and such.
- Top with fresh herbs (she recommends parsley, basil, or dill).
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
21 Most Beneficial Polyphenols & What Foods Have Them
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Roasted chickpeas:
-

16 Overlooked Autistic Traits In Women
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We hear a lot about “autism moms”, but Taylor Heaton is an autistic mom, diagnosed as an adult, and she has insights to share about overlooked autistic traits in women.
The Traits
- Difficulty navigating romantic relationships: often due to misreading signs
- Difficulty understanding things: including the above, but mostly: difficulty understanding subtext, when people leave things as “surely obvious”. Autistic women are likely to be aware of the possible meanings, but unsure which it might be, and may well guess wrongly.
- Masking: one of the reasons for the gender disparity in diagnosis is that autistic women are often better at “masking”, that is to say, making a conscious effort to blend in to allistic society—often as a result of being more societally pressured to do so.
- Honesty: often to a fault
- Copy and paste: related to masking, this is about consciously mirroring others in an effort to put them at ease and be accepted
- Being labelled sensitive and/or gifted: usually this comes at a young age, but the resultant different treatment can have a lifetime effect
- Secret stims: again related to masking, and again for the same reasons that displaying autistic symptoms is often treated worse in women, autistic women’s stims tend to be more subtle.
- Written communication: autistic women are often more comfortable with the written word than the spoken
- Leadership: autistic women will often gravitate to leadership roles, partly as a survival mechanism
- Gaslighting: oneself, e.g. “If this person did this without that, then I can to” (without taking into account that maybe the circumstances are different, or maybe they actually did lean on crutches that you didn’t know were there, etc).
- Inner dialogue: rich inner dialogue, but unable to express it outwardly—often because of the sheer volume of thoughts per second.
- Fewer female friends: often few friends overall, for that matter, but there’s often a gender imbalance towards male friends, or where there isn’t, towards more masculine friends at least.
- Feeling different: often a matter of feeling one does not meet standard expectations in some fashion
- School: autistic women are often academically successful
- Special interests: often more “socially accepted” interests than autistic men’s.
- Flirting: autistic women are often unsure how to flirt or what to do about it, which can result in simple directness instead
For more details on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Related reading:
You might like a main feature of ours from not long back:
Miss Diagnosis: Anxiety, ADHD, & Women
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: