Macadamia Nuts vs Brazil Nuts – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing macadamia nuts to Brazil nuts, we picked the Brazil nuts.
Why?
They’re a lot more nutrient dense! But watch out…
First, to do due diligence in terms of macros: Brazil nuts have twice as much protein and less fat, as well as being a little higher in fiber and slightly lower in carbs.
In terms of vitamins, Brazil nuts are about 10x higher in vitamin E, while macadamias are somewhat higher in several B-vitamins.
The category of minerals is where it gets interesting. Macadamia nuts are a little higher in iron and considerably higher in Manganese. But… Brazil nuts are a lot higher in calcium, copper, magnesium, phosphorus, potassium, selenium, and zinc.
About that selenium… Specifically, it’s more than 5,000x higher, and a cup of Brazil nuts would give nearly 10,000x the recommended daily amount of selenium. Now, selenium is an essential mineral (needed for thyroid hormone production, for example), and at the RDA it’s good for good health. Your hair will be luscious and shiny. However, go much above that, and selenium toxicity becomes a thing, you may get sick, and it can cause your (luscious and shiny) hair to fall out. For this reason, it’s recommended to eat no more than 3–4 Brazil nuts per day.
In short… Brazil nuts are much more nutrient dense in general, and thus come out on top here. But, they’re so nutrient dense in the case of selenium, that careful moderation is advised.
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Seed Saving Secrets – by Alice Mirren

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We all know that home-grown is best, and yet many of us are not exactly farmers (this reviewer tries with mixed results—hardy crops survive; others, not so much). While it’s easy to blame the acidic soil, the harsh climate, or not having enough time and money (this reviewer blames all of the above), the fact remains that a skilled gardener can produce a good crop in any conditions.
That’s where this book helps; right from the beginning, from the seeds. Have you ever bought a pack of seeds, excitedly sown them, and then had a germination rate of zero or something close to that (this reviewer has)?
Alice Mirren takes us on a tour of how to save seeds from plants you know are regionally viable (not the product of some vast globalized industry that doesn’t know you live in an ancient bog with a cold south-east wind blowing in from Siberia), and then how to care for and curate them, how to store them for future years, how to keep a self-perpetuating seed bank.
She goes beyond that, though. Regular 10almonds readers might remember about the supercentenarian “Blue Zones”, and how big factors in healthy longevity include community and purpose; Mirren advocates for organizing community seed banks, which will also mean that everyone (including you) has access to much more diverse seeds, and when it comes to the perils of natural selection, diversity means survival. Otherwise, if you have just one seed type, a single blight can wipe out everything pretty much overnight.
Bottom line: if you grow your own food or would like to, this is a “bible of…” level book that you absolutely should have to hand.
Click here to check out Seed Saving Secrets, and see the results in your kitchen and on your plate!
Share This Post
-

Deficiency In Two Vitamins & Two Minerals Linked To Cognitive Decline
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
…and other items from this week’s health news:
Food for thought
Researchers (Dr. Samitinjaya Dhakal et al.) analyzed dietary intake, eating patterns, and cognitive function in adults aged 65 and older, and found that higher intakes of fiber, healthy unsaturated fats, and micronutrients including vitamins A and E, as well as magnesium and potassium, were associated with better brain health and memory.
It is also worth mentioning that carotenoids, the pigments that give many fruits and vegetables their bright colors, were also linked to better overall cognitive function.
Nevertheless, nearly all participants had diets that fell short of age-appropriate nutrient adequacy, and some did even worse—higher consumption of refined grains such as white bread, certain cereals, pasta, and crackers was negatively associated with cognitive function and memory (i.e. they were associated with lower scores in those things).
Read in full: Fiber and certain micronutrients help with healthy brain aging, study finds
Related: A New Contender For “Best Diet For Heart & Brain” In Aging
Too old for it? No, but…
Researchers from the University of Tartu in Estonia analyzed data from 67,334 adults aged 18–89 in the Estonian Biobank, representing about 7% of the country’s adult population, to examine how sexual desire varies with demographic factors.
There were some interesting findings, including:
- men’s desire and age: men’s reported sexual desire peaked in their late 30s and early 40s rather than in their teens or 20s, which rather challenges long-held assumptions about male desire across the lifespan.
- women’s desire and age: sexual desire tended to decline with age for everyone, but the decrease was significantly steeper in women than in men; it also decreased more if in a family with children.
The researchers wrote that “demographic factors alone—even without accounting for psychological or relational influences—explained 28% of the variance in sexual desire,” meaning that nearly one-third of differences can be predicted from factors such as age, gender, education, and family situation.
In particular the men’s age range thing is quite interesting, as it means it’s not linked to peak testosterone (which would be teens and 20s).
Read in full: What a study of 67,000 people reveals about sexual desire and age
Related: Who Initiates Sex & Why It Matters
When teens need more social media, not less
Social media is often thought as a “Big Bad” when it comes to health in general, and older adults tend to especially hold this view when it comes to teens and younger. However, science suggests it’s not always true!
Researchers (Dr. Rachel Curtis et al.) analyzed data from nearly 100,991 children followed from grades 4 through 12, using self-reported social media use and annual wellbeing surveys covering happiness, life satisfaction, and emotional regulation.
There’s a definite “Goldilocks zone”, because:
- Those using social media for more than two hours every day were more likely to have low wellbeing compared with moderate users.
- Those not using social media at all were also much more likely to have poorer wellbeing, particularly in older adolescents.
This held true regardless of gender, but there was a disparity in how big the effect was, as boys who didn’t use social media were 300% more likely to have low wellbeing, while girls who didn’t use social media were “only” 79% more likely to have low wellbeing.
As the paper concluded:
❝Adolescents reporting moderate use generally demonstrated the most favorable well-being profiles, whereas both nonusers and those with the highest levels of use were at elevated risk for low well-being.❞
Read in full: Can teens use social media too little for their own good? Maybe, study says
Related: Make Social Media Work For Your Mental Health
Take care!
Share This Post
-

Why Going Gluten-Free Could Be A Bad Idea
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is A Gluten-Free Diet Right For You?

This is Rachel Begun, MS, RD. She’s a nutritionist who, since her own diagnosis with Celiac disease, has shifted her career into a position of educating the public (and correcting misconceptions) about gluten sensitivity, wheat allergy, and Celiac disease. In short, the whole “gluten-free” field.
First, a quick recap
We’ve written on this topic ourselves before; here’s what we had to say:
On “Everyone should go gluten-free”
Some people who have gone gluten-free are very evangelical about the lifestyle change, and will advise everyone that it will make them lose weight, have clearer skin, more energy, and sing well, too. Ok, maybe not the last one, but you get the idea—a dietary change gets seen as a cure-all.
And for some people, it can indeed make a huge difference!
Begun urges us to have a dose of level-headedness in our approach, though.
Specifically, she advises:
- Don’t ignore symptoms, and/but…
- Don’t self-diagnose
- Don’t just quit gluten
One problem with self-diagnosis is that we can easily be wrong:
But why is that a problem? Surely there’s not a health risk in skipping the gluten just to be on the safe side? As it turns out, there actually is:
If we self-diagnose incorrectly, Begun points out, we can miss the actual cause of the symptoms, and by cheerfully proclaiming “I’m allergic to gluten” or such, a case of endometriosis, or Hashimoto’s, or something else entirely, might go undiagnosed and thus untreated.
“Oh, I feel terrible today, there must have been some cross-contamination in my food” when in fact, it’s an undiagnosed lupus flare-up, that kind of thing.
Similarly, just quitting gluten “to be on the safe side” can mask a different problem, if wheat consumption (for example) contributed to, but did not cause, some ailment.
In other words: it could reduce your undesired symptoms, but in so doing, leave a more serious problem unknown.
Instead…
If you suspect you might have a gluten sensitivity, a wheat allergy, or even Celiac disease, get yourself tested, and take professional advice on proceeding from there.
How? Your physician should be able to order the tests for you.
You can also check out resources available here:
Celiac Disease Foundation | How do I get tested?
Or for at-home gluten intolerance tests, here are some options weighed against each other:
MNT | 5 gluten intolerance tests and considerations
Want to learn more?
Begun has a blog:
Rachel Begun | More than just recipes
(it is, in fact, just recipes—but they are very simple ones!)
You also might enjoy this interview, in which she talks about gluten sensitivity, celiac disease, and bio-individuality:
Want to watch it, but not right now? Bookmark it for later
Take care!
Share This Post


Related Posts
-
LSD vs Anxiety!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve written before about how psychedelics can have lasting (beneficial!) effects, here:
However, after a lot of research into psilocybin (the active compound in “magic mushrooms”) and some other psychedelics, the “yes even once” part of that was in reference to a study using the psychedelic compound 25CN-NBOH, a selective serotonin 2A receptor agonist (which honestly does not have a snappier name than that or else we’d use it), and how it improved cognitive flexibility (albeit: in mice) in a lasting fashion.
You can read that paper in full (and see graphs!) here:
*About “weeks”; the experiment ran for 20 days and that was that. It is not known how long the benefits would have persisted, only that in the first 20 days, they showed no signs of disappearing.
Suffice it to say, an LSD trip does not last for weeks. So, it seems the changes have been made to the brain and that’s that.
So, what about LSD and anxiety?
A “chill pill” with safe, lasting effects?
We previously shared this study:
However, that was (once again) mice. And, as the study title suggests, repeated LSD use, not just a single dose.
Today, we’ll be looking at a study into the effects of LSD vs anxiety in humans, from a single dose.
Researchers (Dr. Reid Robinson et al.) found that a single LSD dose eased anxiety symptoms for up to 3 months* in 198 patients with moderate to severe anxiety
*This is a case of the study running for three months, so the researchers can’t comment on what how long it lasts after the three months, because the research grant didn’t have enough for a crystal ball for them to use to write about the future and what will happen with the study participants after the study period. After all, at some point one needs to draw a line under it and publish the results.
About that timeline:
- at baseline, all patients had moderate to severe anxiety
- at four weeks, those who took higher doses significantly lowered anxiety scores compared to smaller doses or placebo
- at 12 weeks, 65% of patients who took 100 mg still showed improvements and 48% were in remission
One thing that set this study apart from many is that it unlike most psychedelic studies paired with therapy, this trial tested LSD alone under supervision to isolate the drug’s effect vs placebo, rather than the effect drug+therapy and being unsure whether it would have helped without the therapy.
About that placebo: it was noted as a limitation of the study that that many patients correctly guessed whether they took LSD or placebo (weakening blinding). The resultant high dropout rate (because it’s not very motivating to keep at something where you’re almost certain you received the placebo) reduced the final data set. Still, the researchers did what they could under the circumstances.
You can find the paper itself, here: Single Treatment With MM120 (Lysergide D-Tartrate) in Generalized Anxiety Disorder
On which note, with regard to “lysergide D-tartrate”; that is a form of LSD (it’s a salt of LSD, which is then metabolized as such, so one could argue that it’s essentially a pro-drug), and/but since it is far from the only form of LSD, it cannot be said for sure whether the effects will be the same with any/all LSD. It seems likely that the results will translate just the same to other forms of LSD, but we can’t say that confidently without the science actually being done for it.
Want to learn more?
With regard to psychedelics in general, see:
Taking A Trip Through The Evidence On Psychedelics
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Worried after sunscreen recalls? Here’s how to choose a safe one
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most of us know sunscreen is a key way to protect areas of our skin not easily covered by clothes from excessive ultraviolet (UV) radiation.
But it’s been a rough year for sunscreens.
In June, testing by Choice identified 16 products on Australian shelves that don’t provide the SPF protection they claimed.
In July, the Therapeutic Goods Administration (TGA) released a review recommending the amount of certain chemical ingredients allowed in sunscreens should be lowered.
Since then, several other sunscreens have been recalled or are under review, either due to manufacturing defects or concerns about poor SPF cover.
All this has left many of us feeling confused about which sunscreens are safe, effective and do what they say on the label.
Here’s what you need to know so you can stay safe this summer.

Kindel Media/Pexels The good news first
There’s very little evidence sunscreens cause cancer and plenty of evidence they prevent skin cancer.
This is vital in Australia, where two in three people will get skin cancer at some point in their lives.
One randomised controlled trial in Queensland, run over four and a half years between 1992 and 1996, asked 1,621 people to either use sunscreen every day or continue their usual use (usually one or two days a week or not at all).
It found using sunscreen every day reduced the numbers of squamous cell carcinomas by 40%, compared to the group that didn’t change their habits. Ten years after the study, the number of invasive melanomas was reduced by 73% in the daily sunscreen group.
Significantly, this study was conducted in the 90s using SPF 16 sunscreen. Modern sunscreens are expected to routinely provide SPF 30+ or 50+ protection.
Companies should provide the SPF levels they’re advertising. But this research shows even sub-par sunscreen (by modern standards) provides significant protection with daily use.
Making sure SPF claims stack up
In Australia, the TGA regulates how SPF is assessed in sunscreens, but doesn’t do the testing itself. Instead, companies perform or outsource the testing, which must be done on human skin, and provide the TGA with their results.
But when Choice independently tested 20 Australian sunscreens, it found 16 did not meet the SPF factor on the label.
An ABC investigation pinpointed two potential sources of the problems: a poor quality base ingredient manufactured by Wild Child Laboratories, and suspicious SPF testing data from Princeton Consumer Research, which many of the brands relied on.
The TGA has since recommended that people stop using 21 products that contain the Wild Child base, listed here.
What about the chemical ingredients?
The TGA regularly reviews scientific research to make sure Australian sunscreens keep up with advances in safety and effectiveness. To be sold in Australia, sunscreens must use active ingredients from a specific list, limited at maximum concentrations.
July’s safety review found evidence that two permitted ingredients – homosalate and oxybenzone – can cause hormone disruptions in some animals exposed to high doses for a long time. These doses were far higher than someone would be exposed to from sunscreen – even at the maximum usage – thanks to the TGA’s ingredient limits.
Still, chemical risks are managed strictly. The amount absorbed during consistent, high-dose sunscreen use, year-round, must be less than 1% of the dose known to cause problems in animals.
The new results suggest that absorption could go over this “margin of safety”. So the TGA has recommended the amount allowed be reduced.
Homosalate and oxybenzone are not being banned, and you don’t need to throw out sunscreens containing these ingredients.
But if the idea of using them makes you nervous, you can check ingredient lists and buy sunscreens without them.
What should I look for in a sunscreen?
When buying a sunscreen there are four non-negotiables. It must have:
- 30+ or 50+ SPF
- broad spectrum UV protection (filters both UVB and UVA rays)
- water-resistant (for staying power in Australia’s sweaty climate)
- TGA approval mark on the packaging (“AUST L” followed by a number).
Sunscreen only works if you use it, so choose a sunscreen you like enough to actually wear.
There are milks, gels and creams, unscented, matte, tinted and many other varieties. Since faces are often the most sensitive, many people use a specialty sunscreen for the face and a cheaper, general one for the rest of the body.
Spray-on sunscreen is not recommended, however, because it’s too hard to apply enough.
You need to apply more than you think
Sunscreen works best when you apply it 20 minutes before you go into the sun, and reapply every two hours and after swimming, sport or towel drying.
How you apply it affects how well it works. You need about one teaspoon each for:
- your face and neck
- back
- chest and abdomen
- each arm and leg.
It’s also common to miss your ears, hands, feet and back of the neck – don’t forget these either.
Sunscreen usually lasts two to three years stored below 30°C, so keep an eye on the use-by date and follow any instructions about shaking before use.
If the sunscreen seems to have separated into thinner and thicker layers even after shaking, the ingredients providing SPF may not be mixed evenly throughout and might not work properly.
But remember – sunscreen isn’t a suit of armour
If you’re planning to be out in the sun for more than a few minutes at a time, slip on sun-protective clothing and slap on a hat. Use sunscreen to protect the areas you can’t easily cover.
Slide on sunnies and seek shade where possible to complete your sun-protection practice for a burn-free summer.
Katie Lee, Postdoctoral Researcher, Dermatology Research Centre, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The facts about ultra-processed foods
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
- Ultra-processed foods contain at least one industrially produced ingredient, such as artificial sweeteners, preservatives, or other additives.
- Research suggests diets high in certain ultra-processed foods may be linked to health risks, but most studies are observational and cannot prove cause and effect. Researchers have not established that these foods directly cause health problems.
- Recent state restrictions on ultra-processed foods aim to improve health. But some experts warn they could limit major sources of nutrition for low-income families, disabled individuals, and older adults.
Last summer, U.S. health officials announced plans to address concerns about ultra-processed foods. Although the announcement linked the foods to an “epidemic” of chronic disease, the science on their health effects is still evolving. There is no single scientific consensus on exactly how to define an ultra-processed food.
Here’s what we know so far.
What are ultra-processed foods?
Ultra-processed foods are extremely common, accounting for up to 70 percent of the American diet.
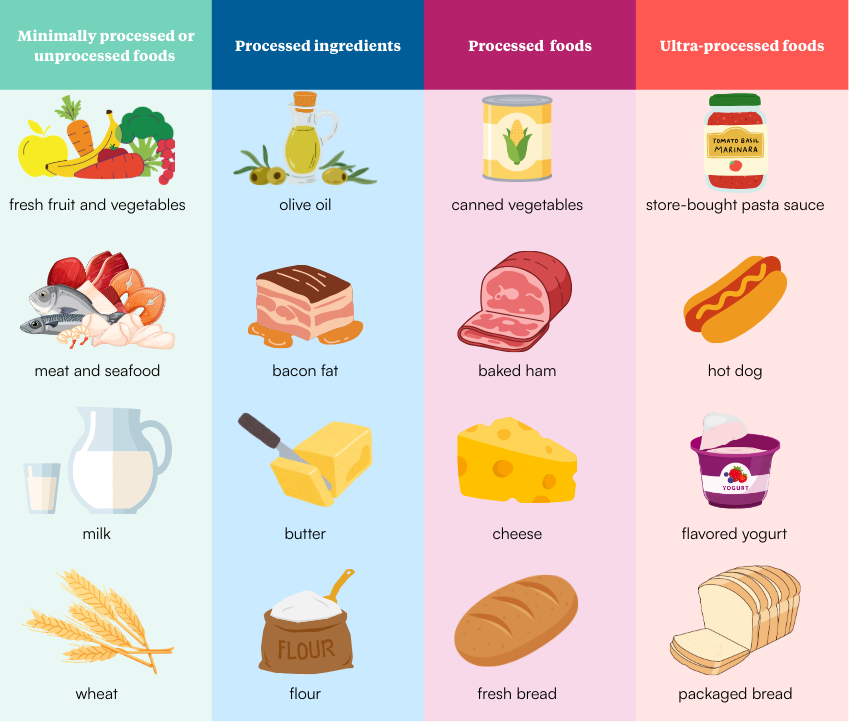
The term “processing” refers to anything that changes ingredients from their natural state. Meat, produce, and grains that have been washed, chopped, ground, juiced, cooked, fermented, pasteurized, or refrigerated are all considered processed.
The distinction between processed and ultra-processed foods isn’t always clear or consistent.
Unprocessed or minimally processed foods
Unprocessed or minimally processed foods are in their natural state or slightly altered from it. Minimal processing typically makes foods safer and more convenient to eat and has little effect on their nutritional value. An apple picked from a tree is unprocessed; fresh apple slices are minimally processed. Raw milk is unprocessed (and unsafe to consume), while pasteurized milk is minimally processed.
Processed ingredients
Processed culinary ingredients are used in food preparation. They are made from unprocessed foods through pressing, churning, grinding, refining, or milling.
These include cooking fats, salt and pepper, ground herbs, natural and refined sweeteners, and milled grains like flour, rice, and oats.
Processed foods
When processed ingredients are used to prepare unprocessed foods, the result is processed foods. Fresh-baked bread, canned fruit, pickles, cheese, and many homemade meals fall into this category.
Ultra-processed foods
Ultra-processed foods are made using one or more industrially produced ingredients. These may include:
- Artificial sweeteners, colors, and flavors
- Hydrogenated fats
- Emulsifiers and thickening agents
- Preservatives that extend shelf life
- Other additives, including fortified nutrients like iron and vitamin B
What does science tell us about ultra-processed foods?
Ultra-processed foods have come under increased scrutiny in recent years, with some researchers and policymakers calling for regulation. However, policies are complicated by the lack of a universally accepted definition of “ultra-processed food.”
“Health authorities across the globe have rejected using the ‘ultra-processed food’ concept as a basis for public health policy, citing its lack of scientific consensus,” wrote the International Food & Beverage Alliance in a November 2025 statement.
Eating ultra-processed foods is associated with health risks.
Many studies have identified links between diets high in ultra-processed foods and health risks. A large 2024 BMJ analysis of previous research included data from nearly 10 million people.
The analysis found that higher consumption of ultra-processed foods was potentially associated with 32 negative health outcomes. The strongest associations were for obesity, type 2 diabetes, cardiovascular disease, and “common mental disorders.”
Research consistently shows that people who consume more ultra-processed foods are at higher risk of weight gain, type 2 diabetes, and cardiovascular conditions. This is particularly true for ultra-processed foods high in sugar, sodium, and saturated fats but low in nutrients.
“Consuming [ultra-processed foods] has two main problems,” said Angela Zivkovic, a nutrition researcher at the University of California, Davis.
“We can more easily overconsume calories and thus gain weight, but also that we may be missing the nutrients that we would be getting if we were instead consuming nutrient-dense whole foods.”
Many health organizations advise reducing intake of ultra-processed foods, particularly those high in salt, sugar, and saturated fats, and replacing them with more nutrient-dense options.
Research on the direct health impacts of ultra-processed food is extremely limited.
Despite consistent associations, there is limited evidence that ultra-processed foods directly cause disease.
In the BMJ analysis, none of the included research studies were rated “high quality,” and much of the evidence was categorized as “weak” or merely “suggestive.” For example, evidence linking ultra-processed foods to overall cancer risk was rated “very low” quality. Evidence for a link with Crohn’s disease (chronic inflammation of the digestive tract) was considered “weak.”
Most research relies on people self-reporting what they remember eating, which can introduce errors.
“We have no way of telling whether the association between the reported intake of [ultra-processed foods] and the disease outcome is due to the intake of [ultra-processed foods] or whether it is a reflection of an overall diet and lifestyle,” added Zivkovic.
“Very few studies that can actually evaluate the direct impacts of [ultra-processed foods] have been performed.”
“Ultra-processed” does not equal “unhealthy.”
The term “ultra-processed food” may bring to mind soda, candy, and chips. But many ultra-processed foods are common parts of healthy diets.
Milk alternatives, packaged bread, breakfast cereal, store-bought pasta sauce, and flavored yogurt are all ultra-processed foods.
Foods fortified with vitamins and minerals are also classified as ultra-processed, often with significant health benefits.
In 1998, the U.S. required enriched grains to be fortified with folic acid, a nutrient essential for early nervous system development. Fortification has been credited with dramatically reducing certain serious birth defects.
What is the health impact of restricting ultra-processed foods?
In August, federal health officials commended six states that banned the purchase of certain highly processed foods with federal Supplemental Nutrition Assistance Program benefits.
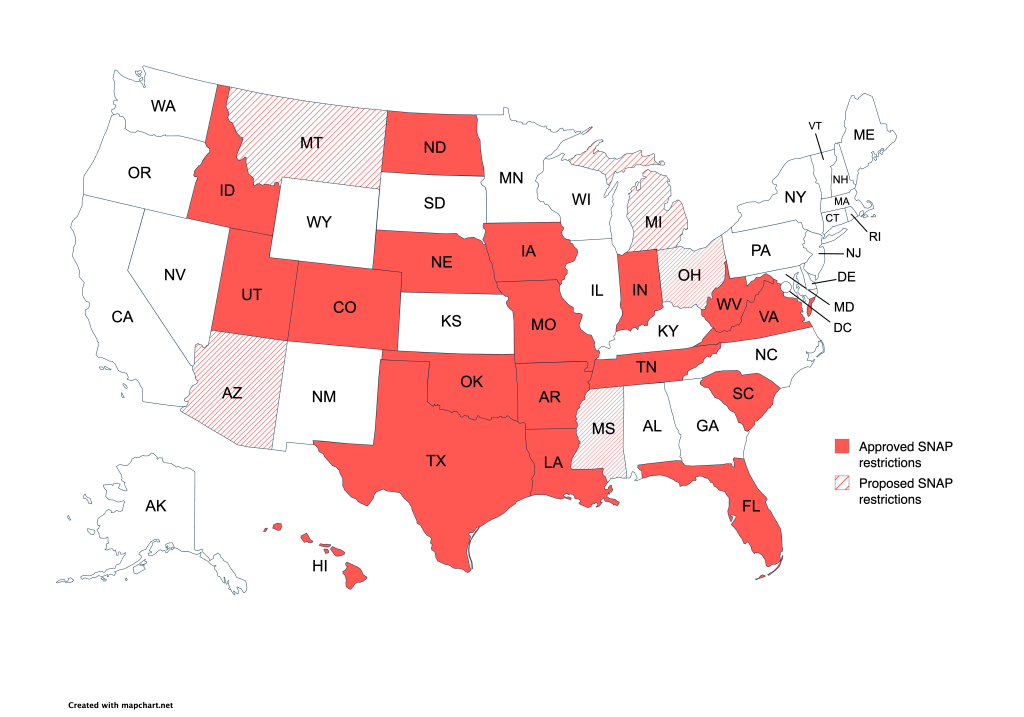
As of January, at least 18 states have SNAP restrictions, and five others have proposed similar policies. The restrictions include many snack foods, frozen meals, sweetened drinks, packaged desserts, gums, and dried fruits.
Source: United States Department of Agriculture, January 28, 2026. While these policies are intended to promote health, some nutrition experts warn they may limit access to affordable and readily available foods for people with low incomes or disabilities.
Ultra-processed foods are often inexpensive, widely available, and shelf-stable. For many households, they provide a significant share of daily calories and nutrients. For others, they are what families can afford and have the time, equipment, or ability to prepare.
About one in 10 Americans live in food deserts, without easy access to a full-service grocery store. In some of these areas, shelf-stable and packaged foods are among the most consistently available options.
Some experts argue that restricting access to ultra-processed foods does not address the underlying barriers to healthy eating, such as cost, transportation, and neighborhood food access.
“For many households, processed foods provide convenience, affordability and stability,” wrote Beverley O’Hara, a nutrition researcher at Leeds Beckett University, in a 2025 The Conversation article.
“Shaming people for eating the foods they can afford or grew up with ignores the realities of everyday life.”
It’s also unclear whether restrictions meaningfully change overall diets.
“Randomized controlled trials that have tested the effects of different limitations or incentives on SNAP purchases demonstrate that…there are no meaningful differences on individuals’ overall dietary intake,” said Kate W. Bauer, a nutrition scientist at the University of Michigan, in a 2025 interview.
Bauer cited a 2016 clinical trial that found SNAP restrictions were effective only when paired with incentives that made fresh foods more affordable.
“Before considering restrictions, we need to address structural barriers like food deserts, transportation limitations, and the higher cost of nutritious foods,” Bauer continued.
“The focus should be on improving food environments rather than restricting choices within inadequate environments.”
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: