How to Prevent Dementia – by Dr. Richard Restak
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve written about this topic here, we know. But there’s a lot more we can do to be on guard against, and pre-emptively strengthen ourselves against, dementia.
The author, a neurologist, takes us on a detailed exploration of dementia in general, with a strong focus on Alzheimer’s in particular, as that accounts for more than half of all dementia cases.
But what if you can’t avoid it? It could be that with the wrong genes and some other factor(s) outside of your control, it will get you if something else doesn’t get you first.
Rather than scaremongering, Dr. Restak tackles this head-on too, and discusses how symptoms can be managed, to make the illness less anxiety-inducing, and look to maintain quality of life as much as possible.
The style of the book is… it reads a lot like an essay compilation. Good essays, then organized and arranged in a sensible order for reading, but distinct self-contained pieces. There are ten or eleven chapters (depending on how we count them), each divided into few or many sections. All this makes for:
- A very “read a bit now and a bit later and a bit the next day” book, if you like
- A feeling of a very quick pace, if you prefer to sit down and read it in one go
Either way, it’s a very informative read.
Bottom line: if you’d like to better understand the many-headed beast that is dementia, this book gives a far more comprehensive overview than we could here, and also explains the prophylactic interventions available.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s Keeping the US From Allowing Better Sunscreens?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When dermatologist Adewole “Ade” Adamson sees people spritzing sunscreen as if it’s cologne at the pool where he lives in Austin, Texas, he wants to intervene. “My wife says I shouldn’t,” he said, “even though most people rarely use enough sunscreen.”
At issue is not just whether people are using enough sunscreen, but what ingredients are in it.
The Food and Drug Administration’s ability to approve the chemical filters in sunscreens that are sold in countries such as Japan, South Korea, and France is hamstrung by a 1938 U.S. law that has required sunscreens to be tested on animals and classified as drugs, rather than as cosmetics as they are in much of the world. So Americans are not likely to get those better sunscreens — which block the ultraviolet rays that can cause skin cancer and lead to wrinkles — in time for this summer, or even the next.
Sunscreen makers say that requirement is unfair because companies including BASF Corp. and L’Oréal, which make the newer sunscreen chemicals, submitted safety data on sunscreen chemicals to the European Union authorities some 20 years ago.
Steven Goldberg, a retired vice president of BASF, said companies are wary of the FDA process because of the cost and their fear that additional animal testing could ignite a consumer backlash in the European Union, which bans animal testing of cosmetics, including sunscreen. The companies are asking Congress to change the testing requirements before they take steps to enter the U.S. marketplace.
In a rare example of bipartisanship last summer, Sen. Mike Lee (R-Utah) thanked Rep. Alexandria Ocasio-Cortez (D-N.Y.) for urging the FDA to speed up approvals of new, more effective sunscreen ingredients. Now a bipartisan bill is pending in the House that would require the FDA to allow non-animal testing.
“It goes back to sunscreens being classified as over-the-counter drugs,” said Carl D’Ruiz, a senior manager at DSM-Firmenich, a Switzerland-based maker of sunscreen chemicals. “It’s really about giving the U.S. consumer something that the rest of the world has. People aren’t dying from using sunscreen. They’re dying from melanoma.”
Every hour, at least two people die of skin cancer in the United States. Skin cancer is the most common cancer in America, and 6.1 million adults are treated each year for basal cell and squamous cell carcinomas, according to the Centers for Disease Control and Prevention. The nation’s second-most-common cancer, breast cancer, is diagnosed about 300,000 times annually, though it is far more deadly.
Dermatologists Offer Tips on Keeping Skin Safe and Healthy
– Stay in the shade during peak sunlight hours, 10 a.m. to 4 p.m. daylight time.– Wear hats and sunglasses.– Use UV-blocking sun umbrellas and clothing.– Reapply sunscreen every two hours.You can order overseas versions of sunscreens from online pharmacies such as Cocooncenter in France. Keep in mind that the same brands may have different ingredients if sold in U.S. stores. But importing your sunscreen may not be affordable or practical. “The best sunscreen is the one that you will use over and over again,” said Jane Yoo, a New York City dermatologist.
Though skin cancer treatment success rates are excellent, 1 in 5 Americans will develop skin cancer by age 70. The disease costs the health care system $8.9 billion a year, according to CDC researchers. One study found that the annual cost of treating skin cancer in the United States more than doubled from 2002 to 2011, while the average annual cost for all other cancers increased by just 25%. And unlike many other cancers, most forms of skin cancer can largely be prevented — by using sunscreens and taking other precautions.
But a heavy dose of misinformation has permeated the sunscreen debate, and some people question the safety of sunscreens sold in the United States, which they deride as “chemical” sunscreens. These sunscreen opponents prefer “physical” or “mineral” sunscreens, such as zinc oxide, even though all sunscreen ingredients are chemicals.
“It’s an artificial categorization,” said E. Dennis Bashaw, a retired FDA official who ran the agency’s clinical pharmacology division that studies sunscreens.
Still, such concerns were partly fed by the FDA itself after it published a study that said some sunscreen ingredients had been found in trace amounts in human bloodstreams. When the FDA said in 2019, and then again two years later, that older sunscreen ingredients needed to be studied more to see if they were safe, sunscreen opponents saw an opening, said Nadim Shaath, president of Alpha Research & Development, which imports chemicals used in cosmetics.
“That’s why we have extreme groups and people who aren’t well informed thinking that something penetrating the skin is the end of the world,” Shaath said. “Anything you put on your skin or eat is absorbed.”
Adamson, the Austin dermatologist, said some sunscreen ingredients have been used for 30 years without any population-level evidence that they have harmed anyone. “The issue for me isn’t the safety of the sunscreens we have,” he said. “It’s that some of the chemical sunscreens aren’t as broad spectrum as they could be, meaning they do not block UVA as well. This could be alleviated by the FDA allowing new ingredients.”
Ultraviolet radiation falls between X-rays and visible light on the electromagnetic spectrum. Most of the UV rays that people come in contact with are UVA rays that can penetrate the middle layer of the skin and that cause up to 90% of skin aging, along with a smaller amount of UVB rays that are responsible for sunburns.
The sun protection factor, or SPF, rating on American sunscreen bottles denotes only a sunscreen’s ability to block UVB rays. Although American sunscreens labeled “broad spectrum” should, in theory, block UVA light, some studies have shown they fail to meet the European Union’s higher UVA-blocking standards.
“It looks like a number of these newer chemicals have a better safety profile in addition to better UVA protection,” said David Andrews, deputy director of Environmental Working Group, a nonprofit that researches the ingredients in consumer products. “We have asked the FDA to consider allowing market access.”
The FDA defends its review process and its call for tests of the sunscreens sold in American stores as a way to ensure the safety of products that many people use daily, rather than just a few times a year at the beach.
“Many Americans today rely on sunscreens as a key part of their skin cancer prevention strategy, which makes satisfactory evidence of both safety and effectiveness of these products critical for public health,” Cherie Duvall-Jones, an FDA spokesperson, wrote in an email.
D’Ruiz’s company, DSM-Firmenich, is the only one currently seeking to have a new over-the-counter sunscreen ingredient approved in the United States. The company has spent the past 20 years trying to gain approval for bemotrizinol, a process D’Ruiz said has cost $18 million and has advanced fitfully, despite attempts by Congress in 2014 and 2020 to speed along applications for new UV filters.
Bemotrizinol is the bedrock ingredient in nearly all European and Asian sunscreens, including those by the South Korean brand Beauty of Joseon and Bioré, a Japanese brand.
D’Ruiz said bemotrizinol could secure FDA approval by the end of 2025. If it does, he said, bemotrizinol would be the most vetted and safest sunscreen ingredient on the market, outperforming even the safety profiles of zinc oxide and titanium dioxide.
As Congress and the FDA debate, many Americans have taken to importing their own sunscreens from Asia or Europe, despite the risk of fake products.
“The sunscreen issue has gotten people to see that you can be unsafe if you’re too slow,” said Alex Tabarrok, a professor of economics at George Mason University. “The FDA is just incredibly slow. They’ve been looking at this now literally for 40 years. Congress has ordered them to do it, and they still haven’t done it.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

13 Things Mentally Strong Couples Don’t Do – by Dr. Amy Morin
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The saying “happy wife; happy life” indeed goes regardless of gender. One can have every other happiness, but if there’s relational trouble, it brings everything else down.
This book is not intended, however, only for people whose relationships are one couple’s therapy session away from divorce. Rather, it’s intended as a preventative. Because, in this as in every other aspect of health, prevention is better than cure!
It is the sign of a strong couple to be proactive about the health of the relationship, and work together to build and reinforce things along the way.
The style of this book is very accessible pop-science, but the author speaks from a strong professional background in social work, psychology, and psychotherapy, and it shows.
Bottom line: if you’d like to strengthen your relationship skills, this book gives 13 great ways to do that.
Share This Post
-

Almonds vs Macadamias – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing almonds to macadamias, we picked the almonds.
Why?
It’s not just our pro-almonds bias:
In terms of macros, almonds have 3x the protein and as well as more fiber and carbs, the ratio of which latter two give almonds the lower glycemic index, while macadamias have more total fat, and 4x the saturated fat percentage. All in all, we say this is a win for almonds in this category.
In the category of vitamins, almonds have more of vitamins B2, B3, B9, E, and choline, while macadamias have more of vitamins B1, B5, B6, and C. A modest 5:4 win for almonds, unless we consider that almonds have more than 47x as much vitamin E (almonds are an exceptionally good source of vitamin E), in which case, a stronger win for almonds.
When it comes to minerals, almonds have more calcium, copper, iron, magnesium, phosphorus, potassium, selenium, and zinc, while macadamias have more manganese. A very clear win for almonds.
Adding up the sections makes for a convincing overall win for almonds, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Why You Should Diversify Your Nuts!
Enjoy!
Share This Post
Related Posts
-
Unlock Your Flexibility With These 4 New Stretches
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
People often stick to the same few stretches, which may limit flexibility progress, especially as the most common stretches often miss deeper, harder-to-reach areas.
So, here are some new (well, probably new to most people, at least) stretches that can get things moving in different directions:
Diversity Continues To Be Good!
The stretches are:
90/90 Hip stretch with a twist:
- Sit with your knees forming 90° angles; add an arm bar and twist your chest upward.
- Hold for 5 deep breaths and repeat.
- This one targets top glute muscles and quadratus lumborum in the lower back.
Shoulder mobility stretch using a wall:
- Kneel in front of a wall with your forearms placed shoulder-width apart, hands turned outward.
- Lift your hips, push your chest toward your legs, and use the wall and your body weight for deeper leverage.
- This one targets multiple shoulder and rotator cuff muscles through external rotation.
Quad stretch using body weight:
- Sit with your feet hip-width apart, lift your hips, step one foot back, and tuck in your tailbone.
- Focus on pointing your knee down and forward for a deep quad stretch.
- This one targets all four quad muscles, hip flexors, plantar fascia, and opens chest/shoulders.
Chicken wing stretch for upper back:
- Sit with bent knees, place the back of one hand on your waist (chicken wing position).
- Tuck the “wing” into the inner thigh, press your knee inward while resisting with the arm.
- This one broadens the shoulder blade and stretches rear shoulder/upper back muscles; it’s particularly effective for reaching difficult upper back areas not typically stretched.
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Yoga Teacher: “If I wanted to get flexible in 2025, here’s what I’d do”
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Sleep Tracking, For Five Million Nights
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
5 Sleep Phenotypes, By Actual Science
You probably know people can be broadly divided into “early birds” and “night owls”:
Early Bird Or Night Owl? Genes vs Environment
…and then the term “hummingbird” gets used for a person who flits between the two.
That’s three animals so far. If you read a book we reviewed recently, specifically this one:
The Power of When – by Dr. Michael Breus
…then you may have used the guide within to self-diagnose your circadian rhythm type (chronotype) according to Dr. Breus’s system, which divides people into bears, lions, wolves, and dolphins.
That’s another four animals. If you have a FitBit, it can “diagnose” you with being those and/or a menagerie of others, such as giraffe, hedgehog, parrot, and tortoise:
How Fitbit Developed the Sleep Profile Experience (Part 2 – Sleep Animals)
Five million nights
A team of researchers recently took a step away from this veritable zoo of 11 different animals and counting, and used a sophisticated modelling system to create a spatial-temporal map of people’s sleep habits, and this map created five main “islands” that people’s sleep habits could settle on, or sometimes move from island to island.
Those “five million nights” by the way? It was actually 5,095,798 nights! You might notice that would take from the 2020s to the 15970s to complete, so this was rather a matter of monitoring 33,152 individuals between January and October of the same year. Between them, they got those 5,095,798 nights of sleep (or in some cases, nights of little or no sleep, but still, they were there for the nights).
The five main phenotypes that the researchers found were:
- What we think of as “normal” sleep. In this phenotype, people get about eight hours of uninterrupted sleep for at least six days in a row.
- As above for half the nights, but they only sleep for short periods of time in bouts of less than three hours the other half.
- As per normal sleep, but with one interrupted night per week, consisting of a 5 hour sleep period and then broken sleep for a few more hours.
- As per normal sleep generally, but with occasional nights in which long bouts of sleep are separated by a mid-sleep waking.
- Sleeping for very short periods of time every night. This phenotype was the rarest the researchers found, and represents extremely disrupted sleep.
As you might suspect, phenotype 1 is healthier than phenotype 5. But that’s not hugely informational, as the correlation between getting good sleep and having good health is well-established. So, what did the study teach us?
❝We found that little changes in sleep quality helped us identify health risks. Those little changes wouldn’t show up on an average night, or on a questionnaire, so it really shows how wearables help us detect risks that would otherwise be missed.❞
More specifically,
❝We found that the little differences in how sleep disruptions occur can tell us a lot. Even if these instances are rare, their frequency is also telling. So it’s not just whether you sleep well or not – it’s the patterns of sleep over time where the key info hides❞
…and, which gets to the absolute point,
❝If you imagine there’s a landscape of sleep types, then it’s less about where you tend to live on that landscape, and more about how often you leave that area❞
In other words: if your sleep pattern is not ideal, that’s one thing and it’d probably be good to address it, by improving your sleep. However, if your sleep pattern changes phenotype without an obvious known reason why, this may be considered an alarm bell warning of something else that needs addressing, which may be an underlying illness or condition—meaning it can be worthwhile being a little extra vigilant when it comes to regular health screenings, in case something new has appeared.
Want to read more?
You can read the paper in full here:
Five million nights: temporal dynamics in human sleep phenotypes
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Qigong: A Breath Of Fresh Air?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Qigong: Breathing Is Good (Magic Remains Unverified)

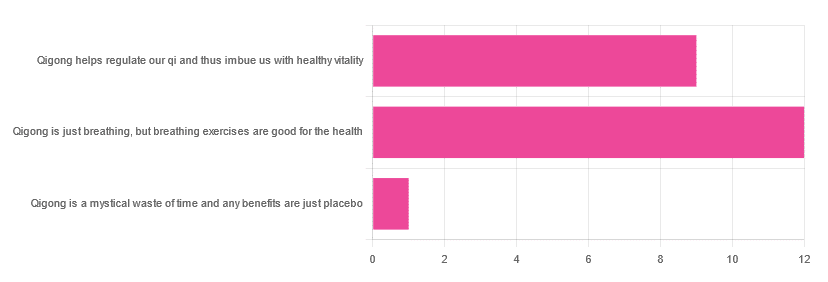
In Tuesday’s newsletter, we asked you for your opinions of qigong, and got the above-depicted, below-described, set of responses:
- About 55% said “Qigong is just breathing, but breathing exercises are good for the health”
- About 41% said “Qigong helps regulate our qi and thus imbue us with healthy vitality”
- One (1) person said “Qigong is a mystical waste of time and any benefits are just placebo”
The sample size was a little low for this one, but the results were quite clearly favorable, one way or another.
So what does the science say?
Qigong is just breathing: True or False?
True or False, depending on how we want to define it—because qigong ranges in its presentation from indeed “just breathing exercises”, to “breathing exercises with visualization” to “special breathing exercises with visualization that have to be exactly this way, with these hand and sometimes body movements also, which also must be just right”, to far more complex definitions that involve qi by various mystical definitions, and/or an appeal to a scientific analog of qi; often some kind of bioelectrical field or such.
There is, it must be said, no good quality evidence for the existence of qi.
Writer’s note, lest 41% of you want my head now: I’ve been practicing qigong and related arts for about 30 years and find such to be of great merit. This personal experience and understanding does not, however, change the state of affairs when it comes to the availability (or rather, the lack) of high quality clinical evidence to point to.
Which is not to say there is no clinical evidence, for example:
Acute Physiological and Psychological Effects of Qigong Exercise in Older Practitioners
…found that qigong indeed increased meridian electrical conductance!
Except… Electrical conductance is measured with galvanic skin responses, which increase with sweat. But don’t worry, to control for that, they asked participants to dry themselves with a towel. Unfortunately, this overlooks the fact that a) more sweat can come where that came from, because the body will continue until it is satisfied of adequate homeostasis, and b) drying oneself with a towel will remove the moisture better than it’ll remove the salts from the skin—bearing in mind that it’s mostly the salts, rather than the moisture itself, that improve the conductivity (pure distilled water does conduct electricity, but not very well).
In other words, this was shoddy methodology. How did it pass peer review? Well, here’s an insight into that journal’s peer review process…
❝The peer-review system of EBCAM is farcical: potential authors who send their submissions to EBCAM are invited to suggest their preferred reviewers who subsequently are almost invariably appointed to do the job. It goes without saying that such a system is prone to all sorts of serious failures; in fact, this is not peer-review at all, in my opinion, it is an unethical sham.❞
~ Dr. Edzard Ernst, a founding editor of EBCAM (he since left, and decries what has happened to it since)
One of the other key problems is: how does one test qigong against placebo?
Scientists have looked into this question, and their answers have thus far been unsatisfying, and generally to the tune of the true-but-unhelpful statement that “future research needs to be better”:
Problems of scientific methodology related to placebo control in Qigong studies: A systematic review
Most studies into qigong are interventional studies, that is to say, they measure people’s metrics (for example, blood pressure, heart rate, maybe immune function biomarkers, sleep quality metrics of various kinds, subjective reports of stress levels, physical biomarkers of stress levels, things like that), then do a course of qigong (perhaps 6 weeks, for example), then measure them again, and see if the course of qigong improved things.
This almost always results in an improvement when looking at the before-and-after, but it says nothing for whether the benefits were purely placebo.
We did find one study that claimed to be placebo-controlled:
…but upon reading the paper itself carefully, it turned out that while the experimental group did qigong, the control group did a reading exercise. Which is… Saying how well qigong performs vs reading (qigong did outperform reading, for the record), but nothing for how well it performs vs placebo, because reading isn’t a remotely credible placebo.
See also: Placebo Effect: Making Things Work Since… Well, A Very Long Time Ago ← this one explains a lot about how placebo effect does work
Qigong is a mystical waste of time: True or False?
False! This one we can answer easily. Interventional studies invariably find it does help, and the fact remains that even if placebo is its primary mechanism of action, it is of benefit and therefore not a waste of time.
Which is not to say that placebo is its only, or even necessarily primary, mechanism of action.
Even from a purely empirical evidence-based medicine point of view, qigong is at the very least breathing exercises plus (usually) some low-impact body movement. Those are already two things that can be looked at, mechanistic processes pointed to, and declarations confidently made of “this is an activity that’s beneficial for health”.
See for example:
- Effects of Qigong practice in office workers with chronic non-specific low back pain: A randomized control trial
- Qigong for the Prevention, Treatment, and Rehabilitation of COVID-19 Infection in Older Adults
- Impact of Medical Qigong on quality of life, fatigue, mood and inflammation in cancer patients: a randomized controlled trial
…and those are all from respectable journals with meaningful peer review processes.
None of them are placebo-controlled, because there is no real option of “and group B will only be tricked into believing they are doing deep breathing exercises with low-impact movements”; that’s impossible.
But! They each show how doing qigong reliably outperforms not doing qigong for various measurable metrics of health.
And, we chose examples with physical symptoms and where possible empirically measurable outcomes (such as COVID-19 infection levels, or inflammatory responses); there are reams of studies showings qigong improves purely subjective wellbeing—but the latter could probably be claimed for any enjoyable activity, whereas changes in inflammatory biomarkers, not such much.
In short: for most people, it indeed reliably helps with many things. And importantly, it has no particular risks associated with it, and it’s almost universally framed as a complementary therapy rather than an alternative therapy.
This is critical, because it means that whereas someone may hold off on taking evidence-based medicines while trying out (for example) homeopathy, few people are likely to hold off on other treatments while trying out qigong—since it’s being viewed as a helper rather than a Hail-Mary.
Want to read more about qigong?
Here’s the NIH’s National Center for Complementary and Integrative Health has to say. It cites a lot of poor quality science, but it does mention when the science it’s citing is of poor quality, and over all gives quite a rounded view:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: