The Hormone Therapy That Reduces Breast Cancer Risk & More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Hormone Balancing Act
We’ve written before about menopausal HRT:
What You Should Have Been Told About Menopause Beforehand
…and even specifically about the considerations when it comes to breast cancer risk:
Menopausal Hormone Replacement Therapy
this really does bear reading, by the way—scroll down to the bit about breast cancer risk, because it’s not a simple increased/decreased risk; it can go either way, and which way it goes will depend on various factors including your medical history and what HRT, if any, you are taking.
Hormone Modulating Therapy
Hormone modulating therapy, henceforth HMT, is something a little different.
Instead of replacing hormones, as hormone replacement therapy does, guess what hormone modulating therapy does instead? That’s right…
MHT can modulate hormones by various means, but the one we’re going to talk about today does it by blocking estrogen receptors,
Isn’t that the opposite of what we want?
You would think so, but since for many people with an increased breast cancer risk, the presence of estrogen increases that risk, which leaves menopausal (peri- or post) people in an unfortunate situation, having to choose between increased breast cancer risk (with estrogen), or osteoporosis and increased dementia risk, amongst other problems (without).
However, the key here (in fact, that’s a very good analogy) is in how the blocker works. Hormones and their receptors are like keys and locks, meaning that the wrong-shaped hormone won’t accidentally trigger it. And when the right-shaped hormone comes along, it gets activated and the message (in this case, “do estrogenic stuff here!” gets conveyed). A blocker is sufficiently similar to fit into the receptor, without being so similar as to otherwise act as the hormone.
In this case, it has been found that HMT blocking estrogen receptors was sufficient to alleviate the breast cancer risk, while also being associated with a 7% lower risk of developing Alzheimer’s disease or related dementias, with that risk reduction being even greater for some demographics depending on race and age. Black women in the 65–74 age bracket enjoyed a 24% relative risk reduction, with white women of the same age getting an 11% relative risk reduction. Black women enjoyed the same benefits after that age, whereas white women starting it at that age did not get the same benefits. The conclusion drawn from this is that it’s good to start this at 65 if relevant and practicable, especially if white, because the protective effect is strongest when gained aged 65–69.
Here’s a pop-science article that goes into the details more deeply than we have room for here:
Hormone therapy for breast cancer linked with lower dementia risk
And here’s the paper itself; we highly recommend reading at least the abstract, because it goes into the numbers in much more detail than we reasonably can here. It’s a huge cohort study of 18,808 women aged 65 years or older, so this is highly relevant data:
Want to learn more?
If you’d like a much deeper understanding of breast cancer risk management, including in the context of hormone therapy, you might like this excellent book that we reviewed recently:
The Smart Woman’s Guide to Breast Cancer – by Dr. Jenn Simmons
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How they did it: STAT reporters expose how ailing seniors suffer when Medicare Advantage plans use algorithms to deny care

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In a call with a long-time source, what stood out most to STAT reporters Bob Herman and Casey Ross was just how viscerally frustrated and angry the source was about an algorithm used by insurance companies to decide how long patients should stay in a nursing home or rehab facility before being sent home.
The STAT stories had a far-reaching impact:
- The U.S. Senate Committee on Homeland Security and Government Affairs took a rare step of launching a formal investigation into the use of algorithms by the country’s three largest Medicare Advantage insurers.
- Thirty-two House members urged the Centers for Medicare and Medicaid Services to increase the oversight of algorithms that health insurers use to make coverage decisions.
- In a rare step, CMS launched its own investigation into UnitedHealth. It also stiffened its regulations on the use of proprietary algorithms and introduced plans to audit denials across Medicare Advantage plans in 2024.
- Based on STAT’s reporting, Medicare Advantage beneficiaries filed two class-action lawsuits against UnitedHealth and its NaviHealth subsidiary, the maker of the algorithm, and against Humana, another major health insurance company that was also using the algorithm.
- Amid scrutiny, UnitedHealth renamed NaviHealth.
The companies never allowed an on-the-record interview with their executives, but they acknowledged that STAT’s reporting was true, according to the news organization.
Ross and Herman spoke with The Journalist’s Resource about their project and shared the following eight tips.
1. Search public comments on proposed federal rules to find sources.
Herman and Ross knew that the Centers for Medicare and Medicaid Services had put out a request for public comments, asking stakeholders within the Medicare Advantage industry how the system could improve.
There are two main ways to get Medicare coverage: original Medicare, which is a fee-for-service health plan, and Medicare Advantage, which is a type of Medicare health plan offered by private insurance companies that contract with Medicare. Medicare Advantage plans have increasingly become popular in recent years.
Under the Social Security Act, the public has the opportunity to submit comments on Medicare’s proposed national coverage determinations. CMS uses public comments to inform its proposed and final decisions. It responds in detail to all public comments when issuing a final decision.
The reporters began combing through hundreds of public comments attached to a proposed Medicare Advantage rule that was undergoing federal review. NaviHealth, the UnitedHealth subsidiary and the maker of the algorithm, came up in many of the comments, which include the submitters’ information.
“These are screaming all-caps comments to federal regulators about YOU NEED TO SOMETHING ABOUT THIS BECAUSE IT’S DISGUSTING,” Ross says.
“The federal government is proposing rules and regulations all the time,” adds Herman, STAT’s business of health care reporter. “If someone’s going to take the time and effort to comment on them, they must have at least some knowledge of what’s going on. It’s just a great tool for any journalist to use to figure out more and who to contact.”
The reporters also found several attorneys who had complained in the comments. They began reaching out to them, eventually gaining access to confidential documents and intermediaries who put them in touch with patients to show the human impact of the algorithm.
2. Harness the power of the reader submission box.
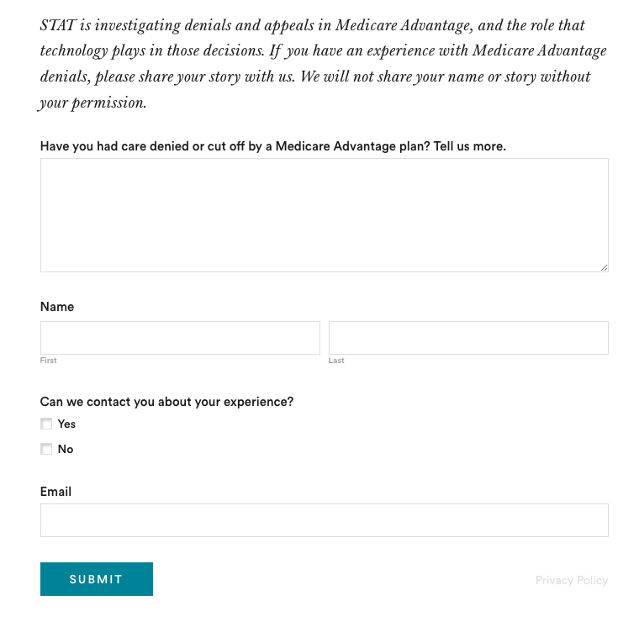
At the suggestion of an editor, the reporters added a reader submission box at the bottom of their first story, asking them to share their own experiences with Medicare Advantage denials.
The floodgates opened. Hundreds of submissions arrived.
By the end of their first story, Herman and Ross had confidential records and some patients, but they had no internal sources in the companies they were investigating, including Navihealth. The submission box led them to their first internal source.

(Screenshot of STAT’s submission box.) The journalists also combed through LinkedIn and reached out to former and current employees, but the response rate was much lower than what they received via the submission box.
The submission box “is just right there,” Herman says. “People who would want to reach out to us can do it right then and there after they read the story and it’s fresh in their minds.”
3. Mine podcasts relevant to your story.
The reporters weren’t sure if they could get interviews with some of the key figures in the story, including Tom Scully, the former head of the Centers for Medicare and Medicaid Services who drew up the initial plans for NaviHealth years before UnitedHealth acquired it.
But Herman and another colleague had written previously about Scully’s private equity firm and they had found a podcast where he talked about his work. So Herman went back to the podcast — where he discovered Scully had also discussed NaviHealth.
The reporters also used the podcast to get Scully on the phone for an interview.
“So we knew we had a good jumping off point there to be like, ‘OK, you’ve talked about NaviHealth on a podcast, let’s talk about this,’” Herman says. “I think that helped make him more willing to speak with us.”
4. When covering AI initiatives, proceed with caution.
“A source of mine once said to me, ‘AI is not magic,’” Ross says. “People need to just ask questions about it because AI has this aura about it that it’s objective, that it’s accurate, that it’s unquestionable, that it never fails. And that is not true.”
AI is not a neutral, objective machine, Ross says. “It’s based on data that’s fed into it and people need to ask questions about that data.”
He suggests several questions to ask about the data behind AI tools:
- Where does the data come from?
- Who does it represent?
- How is this tool being applied?
- Do the people to whom the tool is being applied match the data on which it was trained? “If racial groups or genders or age of economic situations are not adequately represented in the training set, then there can be an awful lot of bias in the output of the tool and how it’s applied,” Ross says.
- How is the tool applied within the institution? Are people being forced to forsake their judgment and their own ability to do their jobs to follow the algorithm?
5. Localize the story.
More than half of all Medicare beneficiaries have Medicare Advantage and there’s a high likelihood that there are multiple Medicare Advantage plans in every county across the nation.
“So it’s worth looking to see how Medicare Advantage plans are growing in your area,” Herman says.
Finding out about AI use will most likely rely on shoe-leather reporting of speaking with providers, nursing homes and rehab facilities, attorneys and patients in your community, he says. Another source is home health agencies, which may be caring for patients who were kicked out of nursing homes and rehab facilities too soon because of a decision by an algorithm.
The anecdote that opens their first story involves a small regional health insurer in Wisconsin, which was using NaviHealth and a contractor to manage post-acute care services, Ross says.
“It’s happening to people in small communities who have no idea that this insurer they’ve signed up with is using this tool made by this other company that operates nationally,” Ross says.
There are also plenty of other companies like NaviHealth that are being used by Medicare Advantage plans, Herman says. “So it’s understanding which Medicare Advantage plans are being sold in your area and then which post-acute management companies they’re using,” he adds.
Some regional insurers have online documents that show which contractors they use to evaluate post-acute care services.
6. Get familiar with Medicare’s appeals databases
Medicare beneficiaries can contest Medicare Advantage denials through a five-stage process, which can last months to years. The appeals can be filed via the Office of Medicare Hearings and Appeals.
“Between 2020 and 2022, the number of appeals filed to contest Medicare Advantage denials shot up 58%, with nearly 150,000 requests to review a denial filed in 2022, according to a federal database,” Ross and Herman write in their first story. “Federal records show most denials for skilled nursing care are eventually overturned, either by the plan itself or an independent body that adjudicates Medicare appeals.”
There are several sources to find appeals data. Be mindful that the cases themselves are not public to protect patient privacy, but you can find the number of appeals filed and the rationale for decisions.
CMS has two quality improvement organizations, or QIOs, Livanta and Kepro, which are required to file free, publicly-available annual reports, about the cases they handle, Ross says.
Another company, Maximus, a Quality Improvement Contractor, also files reports on prior authorization cases it adjudicates for Medicare. The free annual reports include data on raw numbers of cases and basic information about the percentage denials either overturned or upheld on appeal, Ross explains.
CMS also maintains its own database on appeals for Medicare Part C (Medicare Advantage plans) and Part D, which covers prescription drugs, although the data is not complete, Ross explains.
7. Give your editor regular updates.
“Sprinkle the breadcrumbs in front of your editors,” Ross says.
“If you wrap your editors in the process, you’re more likely to be able to get to the end of [the story] before they say, ‘That’s it! Give me your copy,’” Ross says.
8. Get that first story out.
“You don’t have to know everything before you write that first story,” Ross says. “Because with that first story, if it has credibility and it resonates with people, sources will come forward and sources will continue to come forward.”
Read the stories
Denied by AI: How Medicare Advantage plans use algorithms to cut off care for seniors in need
UnitedHealth pushed employees to follow an algorithm to cut off Medicare patients’ rehab care
UnitedHealth used secret rules to restrict rehab care for seriously ill Medicare Advantage patients
This article first appeared on The Journalist’s Resource and is republished here under a Creative Commons license.
Share This Post
-

Blue Cheese vs Brunost – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing blue cheese to brunost, we picked the brunost.
Why?
First, for the unfamiliar, as brunost isn’t necessarily as popular as blue cheese in N. America where most of our readers are:
Brunost, literally “brown cheese” is a traditional Norwegian affair made from aggressively boiling milk, cream, and whey in an iron cauldron. Whereas the blue in blue cheese comes from mold, the brown in brown cheese comes from caramelizing the milk sugars in the cauldron. When we say “cauldron”, yes, there is nowadays mass-produced brunost that is no longer made in something that could be mistaken for a witch’s brew, but the use of cast iron is actually important to the process, and has been the subject of regulatory controversy in Norway; first the cast iron was abandoned, then because that changed the cheese they fortified the product with added iron supplementation, then that was banned, then they reversed it because it affected iron levels in the general population. Nowadays, it is usually made with iron, one way or another.
Ok, so let’s see how they stack up against each other:
In terms of macronutrients, the two cheeses are comparable in fat, but brunost has more carbs—because whereas bacteria (and to a lesser extent, the mold) ate nearly all the carbs in the blue cheese, the caramelization of the milk sugars in brunost meant the result stayed higher in carbs. Both are considered “low GI” foods, but this category is still at least a moderate win for blue cheese.
When it comes to vitamins, brunost is higher in vitamins A, B1, B2, B3, B5, B6, and B12, while blue cheese is higher in vitamin B9. In other words, a clear and easy win for brunost.
In the category of minerals, brunost has more copper, iron, magnesium, manganese, phosphorus, and potassium. Meanwhile, blue cheese contains more zinc, although we can also mention that blue cheese has about 2x the sodium, which is generally not considered a benefit. The two cheeses are about equal in calcium and selenium. Adding these up makes for another clear and easy win for brunost.
In short, unless you are strongly avoiding [even low-GI foods’] carbs for some reason, brunost wins the day by virtue of its overwhelmingly better vitamin and mineral content.
Still, like most fermented dairy products, both cheeses can be enjoyed in moderation as part of a healthy diet (assuming you don’t have an allergy/intolerance).
Want to learn more?
You might like to read:
Take care!
Share This Post
-
Creatine, Genomic Screening, & More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In this week’s health news…
Creatine: no difference vs control at 5g/day
A study found, as the title suggests, no difference between creatine and placebo, at the usual dose of 5g/day, while doing a supervised resistance training program.
This was a 12-week trial, and in the first week, the creatine group put on an average of 0.5kg more lean (i.e. not fat) body mass than the control group, however, as this quickly equalized after the first week, it is assumed that the brief extra weight gain was water weight (creatine promotes water retention, especially in the initial phase).
However, it is still possible that it may promote weight gain at higher doses.
This study was done with adult participants under the age of 50; we’ve noted before that it is generally young people who use creatine for bodybuilding, so in principle, this should have been ideal for that, but it wasn’t.
Read in full: Sports supplement creatine makes no difference to muscle gains, trial finds
Related: Creatine’s Brain Benefits Increase With Age ← this, on the other hand, does work—but only for older adults.
Genomics & disease risk: what to know
In a recent study evaluation, 175,500 participants were screened, and 1 in 30 received medically important genetic results. More than 90% of those found to have a genetic risk were previously unaware of it.
This is important, because most current genetic risk assessment for patients is based on personal and family history, which often misses a lot of data due to barriers to care or lack of family history.
Genomic screening helps close these gaps:
Read in full: Genomic screening is important in identifying disease risk, study finds
Related: Do You Have A Personalized Health Plan? (Here’s How)
FDA-Approved Antivirals (Not Vaccines) Ineffective Against H5N1
The H5N1 avian influenza outbreak is now rife amongst dairy farms, with the virus found in cows’ milk and infecting farmworkers. Researchers studied potential treatments, revealing two FDA-approved antivirals (baloxavir and oseltamivir) were generally ineffective in treating severe H5N1 infections.
Oral infections per raw milk consumption, were the most severe and hardest to treat, and the virus spread quickly to the blood and brain (when the infection is respiratory, it is much slower to spread from the respiratory tract).
It wasn’t a complete loss, though:
- Eye infections were better controlled with baloxavir, achieving a 100% survival rate compared to 25% with oseltamivir.
- For nasal infections, baloxavir reduced viral levels better but still allowed the virus to reach the brain. Survival rates were 75% for baloxavir and 50% for oseltamivir.
The researchers in question are urging preventative measures as being of critical importance, given the difficulty of treatment:
Read in full: Current antivirals likely less effective against severe infection caused by bird flu virus in cows’ milk
Related: Bird Flu: Children At High Risk; Older Adults Not So Much
Take care!
Share This Post


-

Can I take antihistamines everyday? More than the recommended dose? What if I’m pregnant? Here’s what the research says
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Allergies happen when your immune system overreacts to a normally harmless substance like dust or pollen. Hay fever, hives and anaphylaxis are all types of allergic reactions.
Many of those affected reach quickly for antihistamines to treat mild to moderate allergies (though adrenaline, not antihistamines, should always be used to treat anaphylaxis).
If you’re using oral antihistamines very often, you might have wondered if it’s OK to keep relying on antihistamines to control symptoms of allergies. The good news is there’s no research evidence to suggest regular, long-term use of modern antihistamines is a problem.
But while they’re good at targeting the early symptoms of a mild to moderate allergic reaction (sneezing, for example), oral antihistamines aren’t as effective as steroid nose sprays for managing hay fever. This is because nasal steroid sprays target the underlying inflammation of hay fever, not just the symptoms.
Here are the top six antihistamines myths – busted.
Andrea Piacquadio/Pexels Myth 1. Oral antihistamines are the best way to control hay fever symptoms
Wrong. In fact, the recommended first line medical treatment for most patients with moderate to severe hay fever is intranasal steroids. This might include steroid nose sprays (ask your doctor or pharmacist if you’d like to know more).
Studies have shown intranasal steroids relieve hay fever symptoms better than antihistamine tablets or syrups.
To be effective, nasal steroids need to be used regularly, and importantly, with the correct technique.
In Australia, you can buy intranasal steroids without a doctor’s script at your pharmacy. They work well to relieve a blocked nose and itchy, watery eyes, as well as improve chronic nasal blockage (however, antihistamine tablets or syrups do not improve chronic nasal blockage).
Some newer nose sprays contain both steroids and antihistamines. These can provide more rapid and comprehensive relief from hay fever symptoms than just oral antihistamines or intranasal steroids alone. But patients need to keep using them regularly for between two and four weeks to yield the maximum effect.
For people with seasonal allergic rhinitis (hayfever), it may be best to start using intranasal steroids a few weeks before the pollen season in your regions hits. Taking an antihistamine tablet as well can help.
Antihistamine eye drops work better than oral antihistamines to relieve acutely itchy eyes (allergic conjunctivitis).
Myth 2. My body will ‘get used to’ antihistamines
Some believe this myth so strongly they may switch antihistamines. But there’s no scientific reason to swap antihistamines if the one you’re using is working for you. Studies show antihistamines continue to work even after six months of sustained use.
Myth 3. Long-term antihistamine use is dangerous
There are two main types of antihistamines – first-generation and second-generation.
First-generation antihistamines, such as chlorphenamine or promethazine, are short-acting. Side effects include drowsiness, dry mouth and blurred vision. You shouldn’t drive or operate machinery if you are taking them, or mix them with alcohol or other medications.
Most doctors no longer recommend first-generation antihistamines. The risks outweigh the benefits.
The newer second-generation antihistamines, such as cetirizine, fexofenadine, or loratadine, have been extensively studied in clinical trials. They are generally non-sedating and have very few side effects. Interactions with other medications appear to be uncommon and they don’t interact badly with alcohol. They are longer acting, so can be taken once a day.
Although rare, some side effects (such as photosensitivity or stomach upset) can happen. At higher doses, cetirizine can make some people feel drowsy. However, research conducted over a period of six months showed taking second-generation antihistamines is safe and effective. Talk to your doctor or pharmacist if you’re concerned.
Allergies can make it hard to focus. Pexels/Edward Jenner Myth 4. Antihistamines aren’t safe for children or pregnant people
As long as it’s the second-generation antihistamine, it’s fine. You can buy child versions of second-generation antihistamines as syrups for kids under 12.
Though still used, some studies have shown certain first-generation antihistamines can impair childrens’ ability to learn and retain information.
Studies on second-generation antihistamines for children have found them to be safer and better than the first-generation drugs. They may even improve academic performance (perhaps by allowing kids who would otherwise be distracted by their allergy symptoms to focus). There’s no good evidence they stop working in children, even after long-term use.
For all these reasons, doctors say it’s better for children to use second-generation than first-generation antihistimines.
What about using antihistimines while you’re pregnant? One meta analysis of combined study data including over 200,000 women found no increase in fetal abnormalities.
Many doctors recommend the second-generation antihistamines loratadine or cetirizine for pregnant people. They have not been associated with any adverse pregnancy outcomes. Both can be used during breastfeeding, too.
Myth 5. It is unsafe to use higher than the recommended dose of antihistamines
Higher than standard doses of antihistamines can be safely used over extended periods of time for adults, if required.
But speak to your doctor first. These higher doses are generally recommended for a skin condition called chronic urticaria (a kind of chronic hives).
Myth 6. You can use antihistamines instead of adrenaline for anaphylaxis
No. Adrenaline (delivered via an epipen, for example) is always the first choice. Antihistamines don’t work fast enough, nor address all the problems caused by anaphylaxis.
Antihistamines may be used later on to calm any hives and itching, once the very serious and acute phase of anaphylaxis has been resolved.
In general, oral antihistamines are not the best treatment to control hay fever – you’re better off with steroid nose sprays. That said, second-generation oral antihistamines can be used to treat mild to moderate allergy symptoms safely on a regular basis over the long term.
Janet Davies, Respiratory Allergy Stream Co-chair, National Allergy Centre of Excellence; Professor and Head, Allergy Research Group, Queensland University of Technology; Connie Katelaris, Professor of Immunology and Allergy, Western Sydney University, and Joy Lee, Respiratory Allergy Stream member, National Allergy Centre of Excellence; Associate Professor, School of Public Health and Preventive Medicine, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Wrong Arm Position = Wrong Measurement Of Blood Pressure
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is especially important to know if you measure your own blood pressure at home.
Even if you don’t, it’s still good to know this as healthcare providers also can (and often will) do it wrong, especially if they are under time pressure (e.g. they need to get you out of their office and the next person in):
From the heart
Many things can change our blood pressure, and even gravity changes (considerably!) our blood pressure locally.
For example, even with good circulation, so long as we are in the Earth’s gravity under normal conditions (e.g. not skydiving, not riding a rollercoaster, etc), our blood pressure will always be higher below our heart, and lower above it, because gravity is pulling our blood downwards; this is also why if your circulation is not good, you may feel light-headed upon sitting up or standing up, as the bloodstream takes a moment to win a battle against gravity. This is also why blood rushes to your head if you are hanging upside down—increasing the local blood pressure in your head, which unlike your feet, isn’t used to it, so you feel it, and the effect may be visible from the outside, too.
When it comes to having your arm above or below your heart, the difference is less pronounced as it’s only a small change, but that small change can make a big difference:
- If the cuff is above heart level → Lower blood pressure reading.
- If the cuff is below heart level → Higher blood pressure reading.
- Every 1-inch difference causes a 2 mmHg change in readings.
For the reading to be accurate, the blood pressure cuff therefore needs to be at the same height as your heart.
You may be thinking: “my heart is bigger than an inch; do I aim for the middle?”
And the answer is: ideally the cuff should be at the same height as the right atrium of the heart, which is under the midpoint of the sternum.
However, your arm needs to be supported at that height, because if you have to keep it there using your own power, that will mean a tensing of your muscles, and increase in both heart rate and blood pressure. In fact, studies cited in the video found:
- Unsupported arm, in healthy patients → Systolic +8 mmHg, Diastolic +7 mmHg.
- Unsupported arm, in high blood pressure patients → Systolic +23 mmHg, Diastolic +10 mmHg.
Some other considerations; firstly, correct sitting posture:
- Sit upright with back support
- Feet flat on the floor, legs uncrossed
- Arm should be outward from the body and, as per the above explanation, supported (armrest, table, etc.)
And finally, you should be relaxed and at rest.
For example, your writer here is due for a regular checkup in a couple of weeks, and usually when I go there, I will have walked a couple of miles to get there, then bounced cheerfully up 6 flights of stairs. However, for this appointment, I will need to make sure to arrive early, so that I have time for my (so far as I know, happy and healthy) heart to return to its resting pulse and blood pressure.
Also, if you are anything like this writer, the blood pressure cuff activating is not a relaxing experience (and so invites a higher pulse and blood pressure), so it’s better to take three readings and then discard the first one, and record the average of the second two (I do it this way at home).
Similarly, if a medical environment in general is stressful for you, then taking two minutes to do a little mindfulness meditation, or even just breathing exercises, can be good.
For more on all of these, plus also comments on issues such as correct cuff size and tightness, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Common Hospital Blood Pressure Mistake (Don’t Let This Happen To You Or A Loved One)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Measles cases are rising—here’s how to protect your family
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The U.S. is currently experiencing a spike in measles cases across several states. Measles a highly contagious and potentially life-threatening disease caused by a virus. The measles-mumps-rubella (MMR) vaccine prevents measles; unvaccinated people put themselves and everyone around them at risk, including babies who are too young to receive the vaccine.
Read on to learn more about measles: what it is, how to stay protected, and what to do if a measles outbreak happens near you.
What are the symptoms of measles?
Measles symptoms typically begin 10 to 14 days after exposure. The disease starts with a fever followed by a cough, runny nose, and red eyes and then produces a rash of tiny red spots on the face and body. Measles can affect anyone, but is most serious for children under 5, immunocompromised people, and pregnant people, who may give birth prematurely or whose babies may have low birth weight as a result of a measles infection.
Measles isn’t just a rash—the disease can cause serious health problems and even death. About one in five unvaccinated people in the U.S. who get measles will be hospitalized and could suffer from pneumonia, dehydration, or brain swelling.
If you get measles, it can also damage your immune system, making you more vulnerable to other diseases.
How do you catch measles?
Measles spreads through the air when an infected person coughs or sneezes. It’s so contagious that unvaccinated people have a 90 percent chance of becoming infected if exposed.
An infected person can spread measles to others before they have symptoms.
Why are measles outbreaks happening now?
The pandemic caused many children to miss out on routine vaccinations, including the MMR vaccine. Delayed vaccination schedules coincided with declining confidence in vaccine safety and growing resistance to vaccine requirements.
Skepticism about the safety and effectiveness of COVID-19 vaccines has resulted in some people questioning or opposing the MMR vaccine and other routine immunizations.
How do I protect myself and my family from measles?
Getting an MMR vaccine is the best way to prevent getting sick with measles or spreading it to others. The CDC recommends that children receive the MMR vaccine at 12 to 15 months and again at 4 to 6 years, before starting kindergarten.
One dose of the MMR vaccine provides 93 percent protection and two doses provide 97 percent protection against all strains of measles. Because some children are too young to be immunized, it’s important that those around them are vaccinated to protect them.
Is the MMR vaccine safe?
The MMR vaccine has been rigorously tested and monitored over 50 years and determined to be safe. Adverse reactions to the vaccine are extremely rare.
Receiving the MMR vaccine is much safer than contracting measles.
What do I do if there’s a measles outbreak in my community?
Anyone who is not fully vaccinated for measles should be immunized with a measles vaccine as soon as possible. Measles vaccines given within 72 hours after exposure may prevent or reduce the severity of disease.
Children as young as 6 months old can receive the MMR vaccine if they are at risk during an outbreak. If your child isn’t fully vaccinated with two doses of the MMR vaccine—or three doses, if your child received the first dose before their first birthday—talk to your pediatrician.
Unvaccinated people who have been exposed to the virus should stay home from work, school, day care, and other activities for 21 days to avoid spreading the disease.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: