

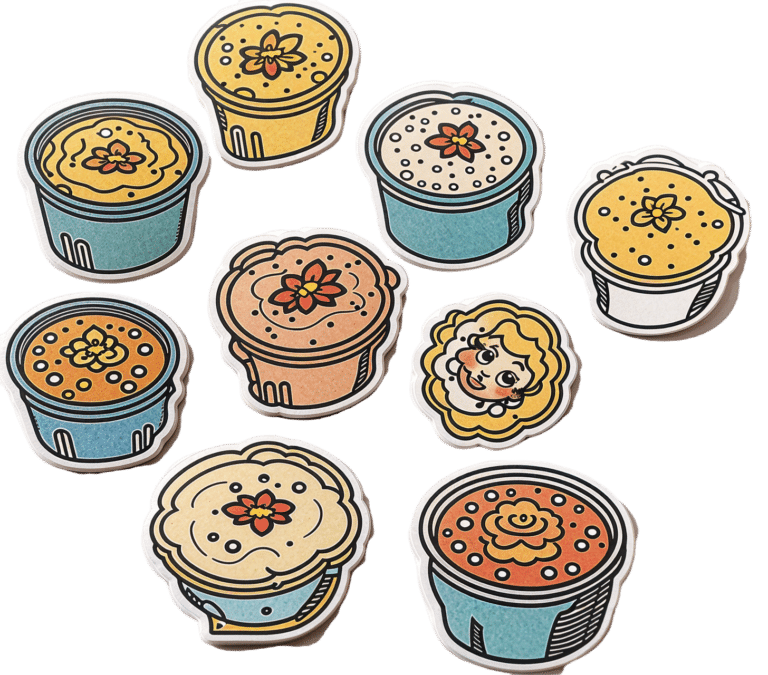
Healthy Chocolate Fudge Energy Bites
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
While these are quite high-calorie, they’re also high in protein, and the fiber and healthy fats flatten the blood sugar curve:
You will need
- 1 cup peanut butter
- 4 oz dark chocolate, melted (try to get dark chocolate with >80% cocoa, if you can; 85% is very respectable and 90% is perfect)
- ⅓ cup maple syrup (you can safely reduce this, or even omit it, if you prefer less sweetness)
- ¼ cup hazelnuts
- ¼ cup almond milk (or your preferred milk, but we recommend almond for taste and health)
- 1 tsp vanilla extract
- Topping: ¼ cup hazelnuts, roughly chopped
Method
(we suggest you read everything at least once before doing anything)
1) Combine all the ingredients (except the topping) in a food processor, and blend until smooth.
2) Line a container (5″x7″ is a good size) with baking paper and spread the mixture evenly into it, pressing down gently.
3) Sprinkle the topping onto it, press that even more gently into it.
4) Refrigerate overnight (or chill it for 2hrs in the freezer).
5) Cut into cubes to serve; they can be served frozen or thawed, per your preference:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Eating For Energy (In Ways That Actually Work)
- “Let Them Eat Cake”, She Said…
- Why You Should Diversify Your Nuts!
- Plant-Based Milks—What’s Best?
- Chocolate & Health: Fact or Fiction?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Kombucha vs Kimchi – Which is Healthier

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kombucha to kimchi, we picked the kombucha.
Why?
While both are very respectable gut-healthy fermented products,
• the kombucha contains fermented tea, a little apple cider vinegar, and a little fiber
• the kimchi contains (after the vegetables) 810 mg sodium in that little tin, and despite the vegetables, no fiber.You may reasonably be surprised that they managed to take something that is made of mostly vegetables and ended up with no fiber without juicing it, but they did. Fermented vegetables are great for the healthy bacteria benefits (and are tasty too!), but the osmotic pressure due to the salt destroys the cell walls and thus the fiber.
Thus, we chose the kombucha that does the same job without delivering all that salt.
However! If you are comparing kombucha and kimchi out in the wilds of your local supermarket, do still check individual labels. It’s not uncommon, for example, for stores to sell pre-made kombucha that’s loaded with sugar.
About sugar and kombucha…
Sugar is required to make kombucha, to feed the yeast and helpful bacteria. However, there should be none of that sugar left (or only the tiniest trace amount) in the final product, because the yeast (and friends) consumed and metabolized it.
What some store brands do, however, is add in sugar afterwards, as they believe it improves the taste. This writer cannot imagine how, but that is their rationale in any case. Needless to say, it is not a healthy addition, and specifically, it’s bad for your gut, which (healthwise) is the whole point of drinking kombucha in the first place.
Want some? Here is an example product on Amazon, but feel free to shop around as there are many flavors available!
Read more about gut health: Gut Health 101
Share This Post
-

Why Going Gluten-Free Could Be A Bad Idea
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is A Gluten-Free Diet Right For You?

This is Rachel Begun, MS, RD. She’s a nutritionist who, since her own diagnosis with Celiac disease, has shifted her career into a position of educating the public (and correcting misconceptions) about gluten sensitivity, wheat allergy, and Celiac disease. In short, the whole “gluten-free” field.
First, a quick recap
We’ve written on this topic ourselves before; here’s what we had to say:
On “Everyone should go gluten-free”
Some people who have gone gluten-free are very evangelical about the lifestyle change, and will advise everyone that it will make them lose weight, have clearer skin, more energy, and sing well, too. Ok, maybe not the last one, but you get the idea—a dietary change gets seen as a cure-all.
And for some people, it can indeed make a huge difference!
Begun urges us to have a dose of level-headedness in our approach, though.
Specifically, she advises:
- Don’t ignore symptoms, and/but…
- Don’t self-diagnose
- Don’t just quit gluten
One problem with self-diagnosis is that we can easily be wrong:
But why is that a problem? Surely there’s not a health risk in skipping the gluten just to be on the safe side? As it turns out, there actually is:
If we self-diagnose incorrectly, Begun points out, we can miss the actual cause of the symptoms, and by cheerfully proclaiming “I’m allergic to gluten” or such, a case of endometriosis, or Hashimoto’s, or something else entirely, might go undiagnosed and thus untreated.
“Oh, I feel terrible today, there must have been some cross-contamination in my food” when in fact, it’s an undiagnosed lupus flare-up, that kind of thing.
Similarly, just quitting gluten “to be on the safe side” can mask a different problem, if wheat consumption (for example) contributed to, but did not cause, some ailment.
In other words: it could reduce your undesired symptoms, but in so doing, leave a more serious problem unknown.
Instead…
If you suspect you might have a gluten sensitivity, a wheat allergy, or even Celiac disease, get yourself tested, and take professional advice on proceeding from there.
How? Your physician should be able to order the tests for you.
You can also check out resources available here:
Celiac Disease Foundation | How do I get tested?
Or for at-home gluten intolerance tests, here are some options weighed against each other:
MNT | 5 gluten intolerance tests and considerations
Want to learn more?
Begun has a blog:
Rachel Begun | More than just recipes
(it is, in fact, just recipes—but they are very simple ones!)
You also might enjoy this interview, in which she talks about gluten sensitivity, celiac disease, and bio-individuality:
Want to watch it, but not right now? Bookmark it for later
Take care!
Share This Post
-

Stop Self-Sabotage – by Dr. Judy Ho
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of books of this genre identify one particular kind of self-sabotage, for example, they might pick one out of:
- Bad habits
- Limiting self-beliefs
- Poor goal-setting
- Procrastination
…etc, slap a quick fix on whatever they chose to focus on, and call it a day. Not so with Dr. Ho!
Here we have a much more comprehensive approach to tackling the problem of unintentional self-sabotage. With a multi-vector method, of which all angles can be improved simultaneously, it becomes much less like “whack-a-mole”… And much more like everything actually getting into order and staying that way.
The main approach here is CBT, but far beyond what most pop-psychology CBT books go for, with more techniques and resources.
On which note…
There are many great exercises that Dr. Ho recommends we do while reading… So you might want to get a nice notebook alongside this book if you don’t already have one! And what is more inspiring of optimism than a new notebook?
Bottom line: this is a great, well-organized guide to pruning the “why am I still doing this to myself?” aspects out of your life for a much more intentional, purposeful, effective way of living.
Click here to check it out on Amazon today, and stop sabotaging yourself!
Share This Post

Related Posts
-

GLP-1 Drugs’ Surprising Brain Benefits
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First introduced as a diabetes medication, GLP-1 drugs quickly took hold for off-label use as weight loss aids, even when the science was still very young.
Here’s one of our first articles on that, back in the day: Semaglutide’s Surprisingly Big Research Gap
As for that popularity? Check out: 1 in 5 US Women Aged 50–64 Has Used GLP-1 RAs: What We’ve Learned
Spoiler, one of the things we’ve learned is: Most People Who Start GLP-1 RAs Quit Them Within A Year (Here’s Why)
Nevertheless, the benefits are plentiful, so it’s worth knowing about. And the latest example of a hitherto-unknown putative benefit is:
Neuroprotectant
Researchers (Dr. Ching-Yang Cheng et al.) examined data from 452,766 adults in the US with an average age of 61, none of whom had epilepsy or seizures at the start of the study, and looked whether GLP-1 medications are associated with a lower risk of developing epilepsy.
In few words: people using GLP-1 drugs were 16% less likely to develop epilepsy over at least five years compared with those using DPP-4 inhibitors (another diabetes drug), after adjusting for factors such as age, high blood pressure, and cardiovascular disease.
Specifically, the GLP-1 drugs included dulaglutide, liraglutide, and semaglutide, with semaglutide showing the strongest association with reduced epilepsy risk. You might be wondering why tirzepatide, a dual GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptor agonist, did not make the list. The answer is that it was not part of the analysis because it became available after the study period began.
It’s worth noting that for its primary purposes, tirzepatide is more effective than its predecessors, including Ozempic:
❝The first GLP-1 mimicking drug was exenatide (Bayetta). It’s still available for treating type 2 diabetes, but there are currently no generics. Exenatide does provide some weight loss, but this is quite modest, typically around 3-5% of body weight.
For liraglutide, those using the drug to treat obesity will use the stronger one (Saxenda), which typically gives about 10% weight loss.
Semaglutide, with the stronger formulation called Wegovy, typically results in 15% weight loss.
The newest GLP-1 mimicking drug on the market, tirzepatide (Mounjaro for type 2 diabetes and Zepbound for weight loss), results in weight loss of around 25% of body weight.❞
Read in full: Ozempic’s cousin drug liraglutide is about to get cheaper. But how does it stack up?
You can also read more about tirzepatide in our main feature about it, here: Mounjaro/Zepbound’s Stable Weight Loss Curve
Back to the more recent study, this (about the reduced epilepsy risk) is an important finding, because it suggests GLP-1 drugs may have neurological effects beyond blood sugar control.
You can find the paper itself, here: Association Between GLP-1 Receptor Agonist Use and Epilepsy Risk in Type 2 Diabetes
And for more on GLP-1 drugs and the brain (albeit in the other direction), see: How Your Emotions Affect GLP-1 Drug Results!
A possible connection?
This is extra interesting too, because the ketogenic diet, which also affects glycemic control albeit by a completely different mechanism, was first conceived for the treatment of children with refractory epilepsy. By starving the body (including the brain) of glucose, the liver must convert fat into fatty acids and ketones, which latter the brain (and indeed the rest of the body) can now use for energy instead of glucose, thus avoiding one of the the main triggers of refractory epilepsy in children.
Source: The Ketogenic Diet: One Decade Later | Pediatrics
Even the pediatric epilepsy studies, however, conclude the keto diet does have unwanted side effects, such as kidney stones, constipation, high cholesterol, and acidosis, so the ketogenic diet is far from a substitute to medical treatments that don’t have such risks.
You can read more about that here: Ketogenic Diet: Burning Fat Or Burning Out?
Want to learn more?
You might like this book that we reviewed a little while back:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Cherries vs Cranberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cherries to cranberries, we picked the cherries.
Why?
In terms of macros, cherries have a little more protein (but it’s not much) while cranberries have a little more fiber, and they’re about equal on carbs. Despite this, cherries have the lower glycemic index—about half that of cranberries. So on balance, a subjective win for cherries, or we could call it a tie.
In the category of vitamins, cherries have a lot more of vitamins A, B1, B2, B3, B7, and B9, while cranberries have more of vitamins B5, B6, C, E, and K. Thus, a modest win for cherries here.
When it comes to minerals, things are more divided: cherries have more calcium, copper, iron, magnesium, phosphorus, potassium, and zinc, while cranberries have more manganese. An easy win for cherries.
In other considerations, both have special beneficial properties of their own (see the “learn more” links below for details of these), but cherries’ properties are solely beneficial, while cranberries have some drawbacks too (despite being famously good vs UTIs, they also increase the risk of kidney stones, so there are pros and cons on the urinary health front). So, we’re calling this round a win for cherries, too.
Adding up the sections makes for a clear overall win for cherries, but by all means enjoy both, unless you have kidney problems, in which case, maybe stick to just the cherries!
Want to learn more?
You might like to read:
- Cherries’ Very Healthy Wealth Of Benefits!
- Health Benefits Of Cranberries (But: You’d Better Watch Out)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
1 in 8 households don’t have the money to buy enough food
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Around one in eight (1.3 million) Australian households experienced food insecurity in 2023. This means they didn’t always have enough money to buy the amount or quality of food they needed for an active and healthy life.
The data, released on Friday by the Australian Bureau of Statistics (ABS), show food insecurity is now a mainstream public health and equity challenge.
When funds are tight, food budgets suffer
The main driver of food insecurity in Australia is financial pressure.
Housing costs and energy bills expenses consume much of household income, leaving food as the most flexible part of the budget.
When money runs short, families cut back on groceries, buy cheaper but less nutritious food, skip meals, or rely on food charities.
These strategies come at the expense of nutrition, health and wellbeing.
Inflation has added further pressure. The cost of food has risen substantially over the past two years, with groceries for a family of four costing around $1,000 per fortnight.
Who is most affected?
Not all households are affected equally. Single parents face the highest rates of food insecurity, with one in three (34%) struggling to afford enough food.
Families with children are more vulnerable (16%) than those without (8%).
Group households, often made up of students or young workers, are also heavily affected at 28%.
Rates are even higher for Aboriginal and Torres Strait Islander households, where 41% report food insecurity.
Income remains a defining factor. Nearly one in four (23.2% of) households in the lowest income bracket experience food insecurity, compared with just 3.6% in the highest.
These headline numbers are only part of the story. Past research shows higher risks of food insecurity for some other groups:
- rural and remote communities face higher food prices and limited outlets. Some areas are becoming “food deserts” where affordable, nutritious food simply isn’t available
- university students and young adults juggle unstable work and housing costs while studying
- temporary residents are often excluded from available supports
- culturally and linguistically diverse households can struggle to access affordable, culturally appropriate food.
While the ABS survey can not provide local breakdowns, it will also be important to know which states and territories have higher rates of food insecurity, to better inform state-level responses.
What are the impacts?
Food insecurity is both a symptom and a cause of poor health.
It leads to poorer quality diets, as households cut back on fruit, vegetables and protein-rich foods that spoil quickly. Instead, they may rely on processed items that are cheaper, more filling and keep for longer.
The ongoing stress of worrying about not having enough food takes a toll on mental health and increases social isolation.
Together these pressures increase the risk of chronic diseases including diabetes, heart disease and some cancers.
For children, not having enough food affects concentration, learning and long-term development.
Breaking this cycle means recognising that improving health depends on improving food security. Left unaddressed, food insecurity deepens existing inequalities across generations.
What can we do about it?
We already know the solutions to food insecurity and they are evidence-based.
Strengthening income support by increasing the amount of JobSeeker and other government payments is crucial. This would ensure households have enough money to cover food alongside other essentials.
Investment in universal school meals, such as free lunch programs, can guarantee children at least one nutritious meal a day.
Policies that make healthy food more affordable and available in disadvantaged areas are also important, whether through subsidies, price regulation, or support for local retailers.
Community-based approaches, such as food co-operatives where members share bulk-buying power and social supermarkets that sell donated or surplus food at low cost can help people buy cheaper food. However, they cannot be a substitute for systemic reform.
Finally, ongoing monitoring of food insecurity must be embedded in national health and social policy frameworks so we can track progress over time. The last ABS data on food insecurity was collected ten years ago, and we cannot wait another decade to understand how Australians are faring.
The National Food Security Strategy is being developed by the Department of Agriculture, Fisheries and Forestry with guidance from a new National Food Council. It provides an opportunity to align these actions, set measurable targets and ensure food security is addressed at a national scale.
Food insecurity is widespread and shaped by disadvantage, with serious health consequences. The question is no longer whether food insecurity exists, but whether Australia will act on the solutions.
Katherine Kent, Senior Lecturer in Nutrition and Dietetics, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:


