Elon Musk says ketamine can get you out of a ‘negative frame of mind’. What does the research say?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
X owner Elon Musk recently described using small amounts of ketamine “once every other week” to manage the “chemical tides” that cause his depression. He says it’s helpful to get out of a “negative frame of mind”.
This has caused a range of reactions in the media, including on X (formerly Twitter), from strong support for Musk’s choice of treatment, to allegations he has a drug problem.
But what exactly is ketamine? And what is its role in the treatment of depression?
It was first used as an anaesthetic
Ketamine is a dissociative anaesthetic used in surgery and to relieve pain.
At certain doses, people are awake but are disconnected from their bodies. This makes it useful for paramedics, for example, who can continue to talk to injured patients while the drug blocks pain but without affecting the person’s breathing or blood flow.
Ketamine is also used to sedate animals in veterinary practice.
Ketamine is a mixture of two molecules, usually referred to a S-Ketamine and R-Ketamine.
S-Ketamine, or esketamine, is stronger than R-Ketamine and was approved in 2019 in the United States under the drug name Spravato for serious and long-term depression that has not responded to at least two other types of treatments.
Ketamine is thought to change chemicals in the brain that affect mood.
While the exact way ketamine works on the brain is not known, scientists think it changes the amount of the neurotransmitter glutamate and therefore changes symptoms of depression.
How was it developed?
Ketamine was first synthesised by chemists at the Parke Davis pharmaceutical company in Michigan in the United States as an anaesthetic. It was tested on a group of prisoners at Jackson Prison in Michigan in 1964 and found to be fast acting with few side effects.
The US Food and Drug Administration approved ketamine as a general anaesthetic in 1970. It is now on the World Health Organization’s core list of essential medicines for health systems worldwide as an anaesthetic drug.
In 1994, following patient reports of improved depression symptoms after surgery where ketamine was used as the anaesthetic, researchers began studying the effects of low doses of ketamine on depression.

SB Arts Media/Shutterstock
The first clinical trial results were published in 2000. In the trial, seven people were given either intravenous ketamine or a salt solution over two days. Like the earlier case studies, ketamine was found to reduce symptoms of depression quickly, often within hours and the effects lasted up to seven days.
Over the past 20 years, researchers have studied the effects of ketamine on treatment resistant depression, bipolar disorder, post-traumatic sress disorder obsessive-compulsive disorder, eating disorders and for reducing substance use, with generally positive results.
One study in a community clinic providing ketamine intravenous therapy for depression and anxiety found the majority of patients reported improved depression symptoms eight weeks after starting regular treatment.
While this might sound like a lot of research, it’s not. A recent review of randomised controlled trials conducted up to April 2023 looking at the effects of ketamine for treating depression found only 49 studies involving a total of 3,299 patients worldwide. In comparison, in 2021 alone, there were 1,489 studies being conducted on cancer drugs.
Is ketamine prescribed in Australia?
Even though the research results on ketamine’s effectiveness are encouraging, scientists still don’t really know how it works. That’s why it’s not readily available from GPs in Australia as a standard depression treatment. Instead, ketamine is mostly used in specialised clinics and research centres.
However, the clinical use of ketamine is increasing. Spravato nasal spray was approved by the Australian Therapuetic Goods Administration (TGA) in 2021. It must be administered under the direct supervision of a health-care professional, usually a psychiatrist.
Spravato dosage and frequency varies for each person. People usually start with three to six doses over several weeks to see how it works, moving to fortnightly treatment as a maintenance dose. The nasal spray costs between A$600 and $900 per dose, which will significantly limit many people’s access to the drug.
Ketamine can be prescribed “off-label” by GPs in Australia who can prescribe schedule 8 drugs. This means it is up to the GP to assess the person and their medication needs. But experts in the drug recommend caution because of the lack of research into negative side-effects and longer-term effects.
What about its illicit use?
Concern about use and misuse of ketamine is heightened by highly publicised deaths connected to the drug.
Ketamine has been used as a recreational drug since the 1970s. People report it makes them feel euphoric, trance-like, floating and dreamy. However, the amounts used recreationally are typically higher than those used to treat depression.
Information about deaths due to ketamine is limited. Those that are reported are due to accidents or ketamine combined with other drugs. No deaths have been reported in treatment settings.
Reducing stigma
Depression is the third leading cause of disability worldwide and effective treatments are needed.
Seeking medical advice about treatment for depression is wiser than taking Musk’s advice on which drugs to use.
However, Musk’s public discussion of his mental health challenges and experiences of treatment has the potential to reduce stigma around depression and help-seeking for mental health conditions.
Clarification: this article previously referred to a systematic review looking at oral ketamine to treat depression. The article has been updated to instead cite a review that encompasses other routes of administration as well, such as intravenous and intranasal ketamine.![]()
Julaine Allan, Associate Professor, Mental Health and Addiction, Rural Health Research Institute, Charles Sturt University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Led by RFK Jr., Conservatives Embrace Raw Milk. Regulators Say It’s Dangerous.

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In summertime, cows wait under a canopy to be milked at Mark McAfee’s farm in Fresno, California. From his Cessna 210 Centurion propeller plane, the 63-year-old can view grazing lands of the dairy company he runs that produces products such as unpasteurized milk and cheese for almost 2,000 stores.
Federal regulators say it’s risky business. Samples of raw milk can contain bird flu virus and other pathogens linked to kidney disease, miscarriages, and death.
McAfee, founder and CEO of the Raw Farm, who also leads the Raw Milk Institute, says he plans to soon be in a position to change that message.
Robert F. Kennedy Jr., the anti-vaccine activist President Donald Trump has tapped to run the Department of Health and Human Services, recruited McAfee to apply for a job as the FDA’s raw milk standards and policy adviser, McAfee said. McAfee has already written draft proposals for possible federal certification of raw dairy farms, he said.
Virologists are alarmed. The Centers for Disease Control and Prevention recommends against unpasteurized dairy that hasn’t been heated to kill pathogens such as bird flu. Interstate raw milk sales for human consumption are banned by the FDA. A Trump administration that weakens the ban or extols raw milk, the scientists say, could lead to more foodborne illness. It could also, they say, raise the risk of the highly pathogenic H5N1 bird flu virus evolving to spread more efficiently, including between people, possibly fueling a pandemic.
“If the FDA says raw milk is now legal and the CDC comes through and says it advises drinking raw milk, that’s a recipe for mass infection,” said Angela Rasmussen, a virologist and co-editor-in-chief of the medical journal Vaccine and an adjunct professor at Stony Brook University in New York.
The raw milk controversy reflects the broader tensions President Donald Trump will confront when pursuing his second-administration agenda of rolling back regulations and injecting more consumer choice into health care.
Many policies Kennedy has said he wants to revisit — from the fluoridation of tap water to nutrition guidance to childhood vaccine requirements — are backed by scientific research and were established to protect public health. Some physician groups and Democrats are gearing up to fight initiatives they say would put people at risk.
Raw milk has gained a following among anti-regulatory conservatives who are part of a burgeoning health freedom movement.
“The health freedom movement was adopted by the tea party, and conspiracy websites gave it momentum,” said Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, who has studied the history of the anti-vaccine movement.
Once-fringe ideas are edging into the mainstream. Vaccine hesitancy is growing.
Arkansas, Utah, and Kentucky are weighing legislation that would relax or end requirements for fluoride in public water. And 30 states now allow for the sale of raw milk in some form within their borders.
While only an estimated 3% of the U.S. population consumes raw milk or cheese, efforts to try to restrict its sales have riled Republicans and provided grist for conservative podcasts.
Many conservatives denounced last year’s execution of a search warrant when Pennsylvania agriculture officials and state troopers arrived at an organic farm tucked off a two-lane road on Jan. 4, 2024. State inspectors were investigating cases of two children sickened by E. coli bacteria and sales of raw dairy from the operation owned by Amish farmer Amos Miller, according to a complaint filed by the state’s agricultural department.
Bundled in flannel shirts and winter jackets, the inspectors put orange stickers on products detaining them from sale, and they left toting product samples in large blue-and-white coolers, online videos show. The 2024 complaint against Miller alleged that he and his wife sold dairy products in violation of state law.
The farm was well known to regulators. They say in the complaint that a Florida consumer died after being sickened in 2014 with listeria bacteria found in raw dairy from Miller’s farm. The FDA said a raw milk sample from the farm indicates it was the “likely source” of the infection, based on the complaint.
Neither Miller’s farm nor his lawyer returned calls seeking comment.
The Millers’ attorney filed a preliminary objection that said “shutting down Defendants would cause inequitable harm, exceed the authority of the agency, constitute an excessive fine as well as disparate, discriminatory punishment, and contravene every essential Constitutional protection and powers reserved to the people of Pennsylvania.”
Regulators in Pennsylvania said in a press release they must protect the public, and especially children, from harm. “We cannot ignore the illnesses and further potential harm posed by distribution of these unregulated products,” the Pennsylvania agricultural department and attorney general said in a joint statement.
Unpasteurized dairy products are responsible for almost all the estimated 761 illnesses and 22 hospitalizations in the U.S. that occur annually because of dairy-related illness, according to a study published in the June 2017 issue of Emerging Infectious Diseases.
But conservatives say raiding an Amish farm is government overreach. They’re “harassing him and trying to make an example of him. Our government is really out of control,” Pennsylvania Republican Sen. Doug Mastriano said in a video he posted to Facebook.
Videos show protesters at a February 2024 hearing on Miller’s case included Amish men dressed in black with straw hats and locals waving homemade signs with slogans such as “FDA Go Away.” A court in March issued a preliminary injunction that barred Miller from marketing and selling raw dairy products within the commonwealth pending appeal, but the order did not preclude sales of raw milk to customers out of state. The case is ongoing.
With Kennedy, the raw milk debate is poised to go national. Kennedy wrote on X in October that the “FDA’s war on public health is about to end.” In the post, he pointed to the agency’s “aggressive suppression” of raw milk, as one example.
McAfee is ready. He wants to see a national raw milk ordinance, similar to one that exists for pasteurized milk, that would set minimal national standards. Farmers could attain certification through training, continuing education, and on-site pathogen testing, with one standard for farms that sell to consumers and another for retail sales.
The Trump administration didn’t return emails seeking comment.
McAfee has detailed the system he developed to ensure his raw dairy products are safe. He confirmed the process for KFF Health News: cows with yellow-tagged ears graze on grass pastures and are cleansed in washing pens before milking. The raw dairy is held back from consumer sale until it’s been tested and found clear of pathogens.
His raw dairy products, such as cheese and milk, are sold by a variety of stores, including health, organic, and natural grocery chains, according to the company website, as well as raw dairy pet products, which are not for human consumption.
He said he doesn’t believe the raw milk he sells could contain or transmit viable bird flu virus. He also said he doesn’t believe regulators’ warnings about raw milk and the virus.
“The pharmaceutical industry is trying to create a new pandemic from bird flu to get their stock back up,” said McAfee, who says he counts Kennedy as a customer. His view is not shared by leading virologists.
In December, the state of California secured a voluntary recall of all his company’s raw milk and cream products due to possible bird flu contamination.
Five indoor cats in the same household died or were euthanized in December after drinking raw milk from McAfee’s farm, and tests on four of the animals found they were infected with bird flu, according to the Los Angeles County Department of Health.
In an unrelated case, Joseph Journell, 56, said three of his four indoor cats drank McAfee’s raw milk. Two fell sick and died, he said. His third cat, a large tabby rescue named Big Boy, temporarily lost the use of his hind legs and had to use a specialized wheelchair device, he said. Urine samples from Big Boy were positive for bird flu, according to a copy of the results from Cornell University and the U.S. Department of Agriculture.
McAfee dismissed connections between the cats’ illnesses and his products, saying any potential bird flu virus would no longer be viable by the time his raw milk gets to stores. He also said he believes that any sick cats got bird flu from recalled pet food.
Journell said he has hired a lawyer to try to recover his veterinary costs but remains a staunch proponent of raw milk.
“Raw milk is good for you, just not if it has bird flu in it,” he said. “I do believe in its healing powers.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post
-
Mythbusting Cookware Materials
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

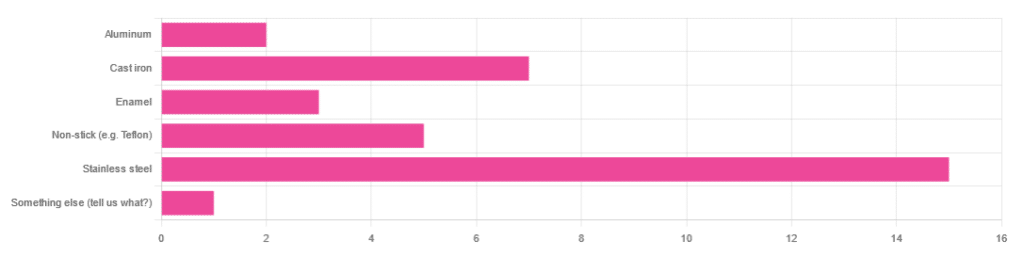
In Wednesday’s newsletter, we asked you what kind of cookware you mostly use, and got the above-depicted, below-described, set of responses:
- About 45% said stainless steel
- About 21% said cast iron
- About 15% said non-stick (e.g. Teflon)
- About 9% said enamel
- About 6% said aluminum
- And 1 person selected “something else”, but then commented to the contrary, writing “I use all of the above”
So, what does the science say about these options?
Stainless steel cookware is safe: True or False?
True! Assuming good quality and normal use, anyway. There really isn’t a lot to say about this, because it’s very unexciting. So long as it is what it is labelled as: there’s nothing coating it, nothing comes out of it unless you go to extremes*, and it’s easy to clean.
*If you cook for long durations at very high temperatures, it can leach nickel and chromium into food. What this means in practical terms: if you are using stainless steel to do deep-frying, then maybe stop that, and also consider going easy on deep-frying in general anyway, because obviously deep-frying is unhealthy for other reasons.
Per normal use, however: pretty much the only way (good quality) stainless steel cookware will harm you is if you touch it while it’s hot, or if it falls off a shelf onto your head.
That said, do watch out for cheap stainless steel cookware that can contain a lot of impurities, including heavy metals. Since you probably don’t have a mass spectrometer and/or chemistry lab at home to check for those impurities, your best guard here is simply to buy from a reputable brand with credible certifications.
Ceramic cookware is safe: True or False?
True… Most of the time! Ceramic pans usually have metal parts and a ceramic cooking surface coated with a very thin layer of silicon. Those metal parts will be as safe as the metals used, so if that’s stainless steel, you’re just as safe as the above. As for the silicon, it is famously inert and body-safe (which is why it’s used in body implants).
However: ceramic cookware that doesn’t have an obvious metal part and is marketed as being pure ceramic, will generally be sealed with some kind of glaze that can leach heavy metals contaminants into the food; here’s an example:
Lead toxicity from glazed ceramic cookware
Copper cookware is safe: True or False?
False! This is one we forgot to mention in the poll, as one doesn’t see a lot of it nowadays. The copper from copper pans can leach into food. Now, of course copper is an important mineral that we must get from our diet, but the amount of copper that that can leach into food from copper pans is far too much, and can induce copper toxicity.
In addition, copper cookware has been found to be, on average, highly contaminated with lead:
Non-stick cookware contaminates the food with microplastics: True or False?
True! If we were to discuss all the common non-stick contaminants here, this email would no longer fit (there’s a size limit before it gets clipped by most email services).
Suffice it to say: the non-stick coating, polytetrafluoroethylene, is itself a PFAS, that is to say, part of the category of chemicals considered environmental pollutants, and associated with a long list of health issues in humans (wherein the level of PFAS in our bloodstream is associated with higher incidence of many illnesses):
You may have noticed, of course, that the “non-stick” coating doesn’t stick very well to the pan, either, and will tend to come off over time, even if used carefully.
Also, any kind of wet cooking (e.g. saucepans, skillets, rice cooker inserts) will leach PFAS into the food. In contrast, a non-stick baking tray lined with baking paper (thus: a barrier between the tray and your food) is really not such an issue.
We wrote about PFAS before, so if you’d like a more readable pop-science article than the scientific paper above, then check out:
PFAS Exposure & Cancer: The Numbers Are High
Aluminum cookware contaminates the food with aluminum: True or False?
True! But not usually in sufficient quantities to induce aluminum toxicity, unless you are aluminum pans Georg who eats half a gram of aluminum per day, who is a statistical outlier and should not be counted.
That’s a silly example, but an actual number; the dose required for aluminum toxicity in blood is 100mg/L, and you have about 5 liters of blood.
Unless you are on kidney dialysis (because 95% of aluminum is excreted by the kidneys, and kidney dialysis solution can itself contain aluminum), you will excrete aluminum a lot faster than you can possibly absorb it from cookware. On the other hand, you can get too much of it from it being a permitted additive in foods and medications, for example if you are taking antacids they often have a lot of aluminum oxide in them—but that is outside the scope of today’s article.
However, aluminum may not be the real problem in aluminum pans:
❝In addition, aluminum (3.2 ± 0.25 to 4.64 ± 0.20 g/kg) and copper cookware (2.90 ± 0.12 g/kg) were highly contaminated with lead.
The time and pH-dependent study revealed that leaching of metals (Al, Pb, Ni, Cr, Cd, Cu, and Fe, etc.) into food was predominantly from anodized and non-anodized aluminum cookware.
More metal leaching was observed from new aluminum cookware compared to old. Acidic food was found to cause more metals to leach during cooking.❞
~ the same paper we cited when talking about copper
Cast iron cookware contaminates the food with iron: True or False?
True, but unlike with the other metals discussed, this is purely a positive, and indeed, it’s even recommended as a good way to fortify one’s diet with iron:
The only notable counterpoint we could find for this is if you have hemochromatosis, a disorder in which the body is too good at absorbing iron and holding onto it.
Thinking of getting some new cookware?
Here are some example products of high-quality safe materials on Amazon, but of course feel free to shop around:
Stainless Steel | Ceramic* | Cast Iron
*it says “non-stick” in the description, but don’t worry, it’s ceramic, not Teflon etc, and is safe
Bonus: rice cooker with stainless steel inner pot
Take care!
Share This Post
-

The Emperor’s New Klotho, Or Something More?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Unzipping The Genes Of Aging?
Klotho is an enzyme encoded in humans’ genes—specifically, in the KL gene.
It’s found throughout all living parts of the human body (and can even circulate about in its hormonal form, or come to rest in its membranaceous form), and its subgroups are especially found:
- α-klotho: in the brain
- β-klotho: in the liver
- γ-klotho: in the kidneys
Great! Why do we care?
Klotho, its varieties and variants, its presence or absence, are very important in aging.
Almost every biological manifestation of aging in humans has some klotho-related indicator; usually the decrease or mutation of some kind of klotho.
Which way around the cause and effect go has been the subject of much debate and research: do we get old because we don’t have enough klotho, or do we make less klotho because we’re getting old?
Of course, everything has to be tested per variant and per system, so that can take a while (punctuated by research scientists begging for more grants to do the next one). Given that it’s about aging, testing in humans would take an incredibly long while, so most studies so far have been rodent studies.
The general gist of the results of rodent studies is “reduced klotho hastens aging; increased klotho slows it”.
(this can be known by artificially increasing or decreasing the level of klotho expression, again something easier in mice as it is harder to arrange transgenic humans for the studies)
Here’s one example of many, of that vast set of rodent studies:
Suppression of Aging in Mice by the Hormone Klotho
Relevance for Alzheimer’s, and a science-based advice
A few years ago (2020), an Alzheimer’s study was undertaken; they noted that the famous apolipoprotein E4 (apoE4) allele is the strongest genetic risk factor for Alzheimer’s, and that klotho may be another. FGF21 (secreted by the liver, mostly during fasting) binds to its own receptor (FGFR1) and its co-receptor β-klotho. Since this is a known neuroprotective factor, they wondered whether klotho itself may interact with β-amyloid (Aβ), and found:
❝Aβ can enhance the ability of klotho to draw FGF21 to regions of incipient neurodegeneration in AD❞
In other words: β-amyloid, the substance whose accumulation is associated with neurodegeneration in Alzheimer’s disease, is a mediator in klotho bringing a known neuroprotective factor, FGF21, to the areas of neurodegeneration
In fewer words: klotho calls the firefighters to the scene of the fire
Read more: Alignment of Alzheimer’s disease amyloid β-peptide and klotho
The advice based on this? Consider practicing intermittent fasting, if that is viable for you, as it will give your liver more FGF21-secreting time, and the more FGF21, the more firefighters arrive when klotho sounds the alarm.
See also: Intermittent Fasting: What’s the truth?
…and while you’re at it:
Does intermittent fasting have benefits for our brain?
A more recent (2023) study with a slightly different (but connected) purpose, found results consistent with this:
Longevity factor klotho enhances cognition in aged nonhuman primates
…and, for that matter this (2023) study that found:
Associations between klotho and telomere biology in high stress caregivers
…which looks promising, but we’d like to see it repeated with a sounder method (they sorted caregiving into “high-stress” and “low-stress” depending on whether a child was diagnosed with ASD or not, which is by no means a reliable way of sorting this). They did ask for reported subjective stress levels, but to be more objective, we’d like to see clinical markers of stress (e.g. cortisol levels, blood pressure, heart rate changes, etc).
A very recent (April 2024) study found that it has implications for more aspects of aging—and this time, in humans (but using a population-based cohort study, rather than lab conditions):
Can I get it as a supplement?
Not with today’s technology and today’s paucity of clinical trials, you can’t. Maybe in the future!
However… The presence of senescent (old, badly copied, stumbling and staggering onwards when they should have been killed and eaten and recycled already) cells actively reduces klotho levels, which means that taking supplements that are senolytic (i.e., that kill those senescent cells) can increase serum klotho levels:
Orally-active, clinically-translatable senolytics restore α-Klotho in mice and humans
Ok, what can I take for that?
We wrote about a senolytic supplement that you might enjoy, recently:
Fisetin: The Anti-Aging Assassin
Want to know more?
If you have the time, Dr. Peter Attia interviews Dr. Dena Dubal (researcher in several of the above studies) here:
Click Here If The Embedded Video Doesn’t Load Automatically
Enjoy!
Share This Post

Related Posts
-

The Path To Revenue – by Theresa Marcroft
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
So many books about start-ups skip right over the elephant in the room: survivorship bias. Not so for Marcroft! This book contains the most comprehensive and unapologetic treatment of it we’ve seen.
Less “here’s what Steve Jobs did right and here’s what Chocolate-Teapots-For-Dogs-R-Us did wrong; don’t mess up that badly and you’ll be fine”… and more realism. Marcroft gives us a many-angled critical analytic approach. In it, she examines why many things can seem similar in both content and presentation… but can cause growth or failure (and how and why), based on more than anecdotes and luck.
The book is information-dense (taking a marketing-centric approach) and/but well-presented in a very readable format.
If we can find any criticism of the book, it’s less about what’s in it and more about what’s not in it. This can never be a “your start-up bible!” book because it’s not comprehensive. It doesn’t cover assembling your team, for example. Nor does it give a lot of attention to management, preferring to focus on strategy.
But no single book can be all things, and we highly recommend this one—the marketing advice alone is more than worth the cost of the book!
Take Your First Step Along The Path To Revenue By Checking It Out On Amazon!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What Happens To Your Body When You Do 100 Glute Bridges Every Day
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Not just for a sculpted butt:
Benefits
With consistent daily glute bridge practice, you may expect:
- Rounder, toned butt: targets the gluteus maximus, toning and lifting the butt for a rounder appearance.
- Improved posture: strengthens glutes to support the spine and pelvis, alleviating lower back and hip pain. Stretches tight hip flexors from prolonged sitting.
- Stronger lower back: glutes support the lower back and spine, reducing pain and making it easier to lift heavy objects. Activating the glutes transfers force from legs to core, preventing injuries.
- Stronger knees: stabilizes the knee joint and promotes alignment by engaging glutes, hamstrings, and quadriceps, reducing knee pain.
- Sculpted hamstrings: contracts hamstrings during lifts for strength, while stretching them on the way down increases flexibility.
- Increased hip flexibility: strengthens muscles around the hip joint, improving mobility and counteracting tight hips from sedentary habits.
- Reduced back pain: strengthens glutes to correct pelvic tilt and reduce strain on the lower back.
- Faster running speed: improves hip extension, strengthens hamstrings, and activates the gluteus medius for better running power and balance.
- Enhanced strength training performance: strengthens glutes, back, and knees, improving performance in exercises like squats and deadlifts.
As for how to get going, the video offers the following very sound advice: begin with 25–30 reps per session and gradually increase to sets of 100 daily. It should take about 5 minutes (that’s 3 seconds per repetition). Results can be seen in as little as 2 weeks, with significant changes after a month of consistent practice.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Strong Curves: A Woman’s Guide to Building a Better Butt and Body – by Bret Contreras & Kellie Davis
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Sciatica Exercises & Home Treatment – by Dr. George Best
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Best is a doctor of chiropractic, but his work here is compelling. He starts by giving an overview of the relevant anatomy, and then the assorted possible causes of sciatica, before moving on to the treatments.
As is generally the case for chiropractic, nothing here will be “cured”, but it will give methods for ongoing management to keep you pain-free—which in the case of sciatica, is usually the single biggest thing that most people suffering from it most dearly want.
We get to read a lot about self-massage and exercises, of the (very well-evidenced; about the most well-evidenced thing there is for back pain) McKenzie technique exercises, as well as assorted acupressure-based techniques that are less well-evidenced but have good anecdotal support.
He also writes about preventing sciatica—which if you already have it, that doesn’t mean it’s too late; it just means, in that case do these things (along with the aforementioned exercises) to gradually reverse the harm done and get back to where you were pre-sciatica.
Lastly, he does also speak on when signs might point to your problems being beyond the scope of this book, and seeking professional examination if you haven’t already.
The style throughout is straight to the point, informative, and instructional. There is zero fluff or padding, and no sensationalization. There are diagrams and illustrative photos where appropriate.
Bottom line: if you have, or fear the threat of, sciatica, then this is an excellent book to have and use its exercises.
Click here to check out Sciatica Exercises & Home Treatment, and live pain-free!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: