Why Chronic Obstructive Pulmonary Disease (COPD) Is More Likely Than You Think
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Chronic Obstructive Pulmonary Disease (COPD): More Likely Than You Think
COPD is not so much one disease, as rather a collection of similar (and often overlapping) diseases. The main defining characteristic is that they are progressive lung diseases. Historically the most common have been chronic bronchitis and emphysema, though Long COVID and related Post-COVID conditions appear to have been making inroads.
Lung cancer is generally considered separately, despite being a progressive lung disease, but there is crossover too:
COPD prevalence is increased in lung cancer, independent of age, sex and smoking history
COPD can be quite serious:
“But I don’t smoke”
Great! In fact we imagine our readership probably has disproportionately few smokers compared to the general population, being as we all are interested in our health.
But, it’s estimated that 30,000,000 Americans have COPD, and approximately half don’t know it. Bear in mind, the population of the US is a little over 340,000,000, so that’s a little under 9% of the population.
Click here to see a state-by-state breakdown (how does your state measure up?)
How would I know if I have it?
It typically starts like any mild respiratory illness. Likely shortness of breath, especially after exercise, a mild cough, and a frequent need to clear your throat.
Then it will get worse, as the lungs become more damaged; each of those symptoms might become stronger, as well as chest tightness and a general lack of energy.
Later stages, you guessed it, the same but worse, and—tellingly—weight loss.
The reason for the weight loss is because you are getting less oxygen per breath, making carrying your body around harder work, meaning you burn more calories.
What causes it?
Lots of things, with smoking being up at the top, or being exposed to a lot of second-hand smoke. Working in an environment with a lot of air pollution (for example, working around chemical fumes) can cause it, as can inhaling dust. New Yorkers: yes, that dust too. It can also develop from other respiratory illnesses, and some people even have a genetic predisposition to it:
Alpha-1 antitrypsin deficiency: a commonly overlooked cause of lung disease
Is it treatable?
Treatment varies depending on what form of it you have, and most of the medical interventions are beyond the scope of this article. Suffice it to say, there are medications that can be taken (including bronchodilators taken via an inhaler device), corticosteroids, antibiotics and antivirals of various kinds if appropriate. This is definitely a “see your doctor” item though, because there are is far too much individual variation for us to usefully advise here.
However!
There are habits we can do to a) make COPD less likely and b) make COPD at least a little less bad if we get it.
Avoiding COPD:
- Don’t smoke. Just don’t.
- Avoid second-hand smoke if you can
- Avoid inhaling other chemicals/dust that may be harmful
- Breathe through your nose, not your mouth; it filters the air in a whole bunch of ways
- Seriously, we know it seems like nostril hairs surely can’t do much against tiny particles, but tiny particles are attracted to them and get stuck in mucous and dealt with by our immune system, so it really does make a big difference
Managing COPD:
- Continue the above things, of course
- Exercise regularly, even just light walking helps; we realize it will be difficult
- Maintain a healthy weight if you can
- This means both ways; COPD causes weight loss and that needs to be held in check. But similarly, you don’t want to be carrying excessive weight either; that will tire you even more.
- Look after the rest of your health; everything else will now hit you harder, so even small things need to be taken seriously
- If you can, get someone to help / do your household cleaning for you, ideally while you are not in the room.
Where can I get more help/advice?
As ever, speak to your doctor if you are concerned this may be affecting you. You can also find a lot of resources via the COPD Foundation’s website.
Take care of yourself!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Own Your Past Change Your Future – by Dr. John Delony

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This one is exactly what it says on the cover. It’s reminiscent in its premise of the more clinically-presented Tell Yourself A Better Lie (an excellent book, which we reviewed previously) but this time presented in a much more casual fashion.
Dr. Delony favors focusing on telling stories, and indeed this book contains many anecdotes. But also he bids the reader to examine our own stories—those we tell ourselves about ourselves, our past, people around us, and so forth.
To call those things “stories” may create a knee-jerk response of feeling like it is an accusation of dishonesty, but rather, it is acknowledging that experiences are subjective, and our framing of narratives can vary.
As for reframing things and taking control, his five-step-plan for doing such is:
- Acknowledge reality
- Get connected
- Change your thoughts
- Change your actions
- Seek redemption
…which each get a chapter devoted to them in the book.
You may notice that these are very similar to some of the steps in 12-step programs, and also some religious groups and/or self-improvement groups. In other words, this may not be the most original approach, but it is a tried-and-tested one.
Bottom line: if you feel like your life needs an overhaul, but don’t want to wade through a bunch of psychology to do it, then this book could be it for you.
Click here to check out Own Your Past To Change Your Future, and do just that!
Share This Post
-

When Doctors Make House Calls, Modern-Style!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

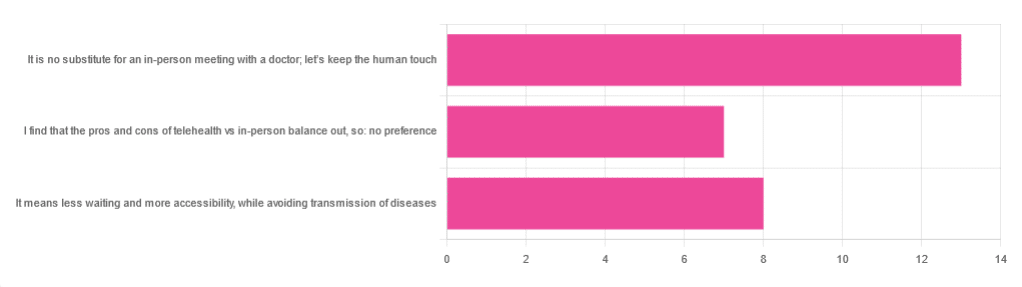
In Tuesday’s newsletter, we asked you foryour opinion of telehealth for primary care consultations*, and got the above-depicted, below-described, set of responses:
- About 46% said “It is no substitute for an in-person meeting with a doctor; let’s keep the human touch”
- About 29% said “It means less waiting and more accessibility, while avoiding transmission of diseases”
- And 25 % said “I find that the pros and cons of telehealth vs in-person balance out, so: no preference”
*We specified that by “primary care” we mean the initial consultation with a non-specialist doctor, before receiving treatment or being referred to a specialist. By “telehealth” we mean by videocall or phonecall.
So, what does the science say?
A quick note first
Because telehealth was barely a thing (statistically speaking) before the first stages of the COVID pandemic, compared to how it is now, most of the science for this is young, and a lot of the science simply hasn’t been done yet, and/or has not been published yet, because the process can take years.
Because of this, some studies we do have aren’t specifically about primary care, and are sometimes about specialists. We think this should not affect the results much, but it bears highlighting.
Nevertheless, we’ll do what we can with the science we have!
Telehealth is more accessible than in-person consultations: True or False?
True, for most people. For example…
❝Data was found from a variety of emergency and non-emergency departments of primary, secondary, and specialised healthcare.
Satisfaction was high among recipients of healthcare, scoring 9-10 on a scale of 0-10 or ranging from 73.3% to 100%.
Convenience was rated high in every specialty examined. Satisfaction of clinicians was high throughout the specialities despite connection failure and concerns about confidentiality of information.❞
whereas…
❝Nonetheless, studies reported perception of increased barriers to accessing care and inequalities for vulnerable patients especially in older people❞
~ Ibid.
Source: Satisfaction with telemedicine use during COVID-19 pandemic in the UK: a systematic review
Now, perception of those things does necessarily equate to an actual increased barrier, but it is reasonable that someone who thinks something is inaccessible will be less inclined to try to access it.
The quality of care provided via telehealth is as good as in-person: True or False?
True, ostensibly, with caveats. The caveats are:
- We’re going offreported patient satisfaction, not objective patient health outcomes (we found little* science as yet for the relative incidence of misdiagnosis, for example—which kind of thing will take time to be revealed).
- We’re also therefore speaking (as statistics do) for the significant majority of people. However, if we happen to be (statistically speaking) an insignificant minority, well, that just sucks for us personally.
*we did find some, but it wasn’t very helpful yet. For example:
An electronic trigger to detect telemedicine-related diagnostic errors
this one does look at the incidence of diagnostic errors, but provides no control group (i.e. otherwise-comparable in-person consultations) for comparison.
While most oft-considered demographic groups reported comparable patient satisfaction (per race, gender, and socioeconomic status, for example), there was one outlier variable, which was age (as we quoted from that first study above).
However!
Looking under the hood of these stats, it seems that age is not the real culprit, so much as technological illiteracy, which is heavily correlated with age:
❝Lower eHealth literacy is associated with more negative attitudes towards I/C technology in healthcare. This trend is consistent across diverse demographics and regions. ❞
Source: Meta-analysis: eHealth literacy and attitudes towards internet/computer technology
There are things that can be done at an in-person consultation that can’t be done by telehealth: True or False?
True, of course. It is incredibly rare that we will cite “common sense”, (as sometimes “common sense” is actually “common mistakes” and is simply and verifiably wrong), but in this case, as one 10almonds subscriber put it:
❝The doctor uses his five senses to assess. This cannot be attained over the phone❞
~ 10almonds subscriber
A quick note first: if your doctor is using their sense of taste to diagnose you, please get a different doctor, because they should definitely not be doing that!
Not in this century, anyway… Once upon a time, diabetes was diagnosed by urine-tasting (and yes, that was a fairly reliable method).
However, nowadays indeed a doctor will use sight, sound, touch, and sometimes even smell.
In a videocall we’re down to two of those senses (sight and sound), and in a phonecall, down to one (sound) and even that is hampered. Your doctor cannot, for example, use a stethoscope over the phone.
With this in mind, it really comes down to what you need from your doctor in that consultation.
- If you’re 99% sure that what you need is to be prescribed an antidepressant, that probably doesn’t need a full physical.
- If you’re 99% sure that what you need is a referral, chances are that’ll be fine by telehealth too.
- If your doctor is 99% sure that what you need is a verbal check-up (e.g. “How’s it been going for you, with the medication that I prescribed for you a month ago?”, then again, a call is probably fine.
If you have a worrying lump, or an unhappy bodily discharge, or an unexplained mysterious pain? These things, more likely an in-person check-up is in order.
Take care!
Share This Post
-

Unprocessed 10th Anniversary Edition – by Abbie Jay
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The main premise of this book is cooking…
- With nutritious whole foods
- Without salt, oil, sugar (“SOS”)
It additionally does it without animal products and without gluten, and (per “nutritious whole foods”), and, as the title suggests, avoiding anything that’s more than very minimally processed. Remember, for example, that if something is fermented, then that fermentation is a process, so the food has been processed—just, minimally.
This is a revised edition, and it’s been adjusted to, for example, strip some of the previous “no salt” low-sodium options (such as tamari with 233mg/tsp sodium, compared to salt’s 2,300mg/tsp sodium).
You may be wondering: what’s left? Tasty, well-seasoned, plant-based food, that leans towards the “comfort food” culinary niche.
Enough to sate the author, after her own battles with anorexia and obesity (in that order) and finally, after various hospital trips, getting her diet where it needed to be for the healthy lifestyle that she lives now, while still getting to eat such dishes as “Chef AJ’s Disappearing Lasagna” and peanut butter fudge truffles and 151 more.
Bottom line: if you want whole-food plant-based comfort-food cooking that’s healthy in general and especially heart-healthy, this book has plenty of that.
Click here to check out Unprocessed: 10th Anniversary Edition, and… Enjoy!
Share This Post


Related Posts
-

The Yoga of Breath – by Richard Rosen
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You probably know to breathe through your nose, and to breathe with your diaphragm. But did you know you’re usually only breathing through one nostril at a time, and alternate between nostrils every few hours? And did you know how to breathe through both nostrils equally instead, and the benefits that can bring?
The above is one example of many, of things that make this book stand out from the crowd when it comes to breathing exercises. Author Richard Rosen has a deep expertise in this topic, and explains everything clearly and comprehensively, without leaving room for ambiguity.
While most of the book focuses on the mechanics and physical techniques of breathing, he does also cover some more mindstate-related things too—without which, it wouldn’t be yoga.
If the book has a downside, it’s that its comprehensive nature could be off-putting to readers new to breathing work in general. However, since he does explain everything from the ground up, that’s no reason to be put off this book, iff you’re serious about learning.
Bottom line: if you’d like a deeper understanding of breathwork than “breathe slowly through your nose, using your diaphragm”, this book will teach you depths of breathing you probably didn’t know were possible.
Click here to check out The Yoga of Breath, and catch yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How often should you really weigh yourself?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Few topics are more debated in health than the value of the humble bathroom scale. Some experts advocate daily self-weigh-ins to promote accountability for weight management, particularly when we’re following a diet and exercise program to lose weight.
Others suggest ditching self-weigh-ins altogether, arguing they can trigger negative psychological responses and unhealthy behaviours when we don’t like, or understand, the number we see on the scale.
Many, like me, recommend using scales to weigh yourself weekly, even when we’re not trying to lose weight. Here’s why.

Diva Plavalaguna/Pexels 1. Weighing weekly helps you manage your weight
Research confirms regular self-weighing is an effective weight loss and management strategy, primarily because it helps increase awareness of our current weight and any changes.
A systematic review of 12 studies found participants who weighed themselves weekly or daily over several months lost 1–3 BMI (body mass index) units more and regained less weight than participants who didn’t weight themselves frequently. The weight-loss benefit was evident with weekly weighing; there was no added benefit with daily weighing.
Weighing regularly means we know when our weight changes. Andres Ayrton/Pexels Self-weigh-ins are an essential tool for weight management as we age. Adults tend to gain weight progressively through middle age. While the average weight gain is typically between 0.5–1kg per year, this modest accumulation of weight can lead to obesity over time. Weekly weighing and keeping track of the results helps avoid unnecessary weight gain.
Tracking our weight can also help identify medical issues early. Dramatic changes in weight can be an early sign of some conditions, including problems with our thyroid, digestion and diabetes.
2. Weekly weighing accounts for normal fluctuations
Our body weight can fluctuate within a single day and across the days of the week. Studies show body weight fluctuates by 0.35% within the week and it’s typically higher after the weekend.
Daily and day-to-day body weight fluctuations have several causes, many linked to our body’s water content. The more common causes include:
The type of food we’ve consumed
When we’ve eaten a dinner higher in carbohydrates, we’ll weigh more the next day. This change is a result of our bodies temporarily carrying more water. We retain 3–4 grams of water per gram of carbohydrate consumed to store the energy we take from carbs.
Our water content also increases when we consume foods higher in salt. Our bodies try to maintain a balance of sodium and water. When the concentration of salt in our bloodstream increases, a mechanism is triggered to restore balance by retaining water to dilute the excess salt.
The morning after a big pasta dinner, we’ll carry more water weight. Dana Tentis/Pexels Our food intake
Whether it’s 30 grams of nuts or 65 grams of lean meat, everything we eat and drink has weight, which increases our body weight temporarily while we digest and metabolise what we’ve consumed.
Our weight also tends to be lower first thing in the morning after our food intake has been restricted overnight and higher in the evening after our daily intake of food and drinks.
Exercise
If we weigh ourselves at the gym after a workout, there’s a good chance we’ll weigh less due to sweat-induced fluid loss. The amount of water lost varies depending on things like our workout intensity and duration, the temperature and humidity, along with our sweat rate and hydration level. On average, we lose 1 litre of sweat during an hour of moderate-intensity exercise.
Hormonal changes
Fluctuations in hormones within your menstrual cycle can also affect fluid balance. Women may experience fluid retention and temporarily gain 0.5–2kg of weight at this time. Specifically, the luteal phase, which represents the second half of a woman’s cycle, results in a shift of fluid from your blood plasma to your cells, and bloating.
Most of our weight fluctuations are water-related. Engin Akyurt/Unsplash Bowel movements
Going to the bathroom can lead to small but immediate weight loss as waste is eliminated from the body. While the amount lost will vary, we generally eliminate around 100 grams of weight through our daily bowel movements.
All of these fluctuations are normal, and they’re not indicative of significant changes in our body fat or muscle mass. However, seeing these fluctuations can lead to unnecessary stress and a fixation with our weight.
3. Weekly weighing avoids scale obsession and weight-loss sabotage
Weighing too frequently can create an obsession with the number on the scales and do more harm than good.
Often, our reaction when we see this number not moving in the direction we want or expect is to further restrict our food intake or embark on fad dieting. Along with not being enjoyable or sustainable, fad diets also ultimately increase our weight gain rather than reversing it.
This was confirmed in a long-term study comparing intentional weight loss among more than 4,000 twins. The researchers found the likelihood of becoming overweight by the age of 25 was significantly greater for a twin who dieted to lose 5kg or more. This suggests frequent dieting makes us more susceptible to weight gain and prone to future weight gain.
So what should you do?
Weighing ourselves weekly gives a more accurate measure of our weight trends over time.
Aim to weigh yourself on the same day, at the same time and in the same environment each week – for example, first thing every Friday morning when you’re getting ready to take a shower, after you’ve gone to the bathroom, but before you’ve drunk or eaten anything.
Weigh yourself at the same time on the same day of the week. Alexanderstock23/Shutterstock Use the best quality scales you can afford. Change the batteries regularly and check their accuracy by using a “known” weight – for example, a 10kg weight plate. Place the “known” weight on the scale and check the measurement aligns with the “known” weight.
Remember, the number on the scale is just one part of health and weight management. Focusing solely on it can overshadow other indicators, such as how your clothes fit. It’s also essential to pay equal attention to how we’re feeling, physically and emotionally.
Stop weighing yourself – at any time interval – if it’s triggering anxiety or stress, and get in touch with a health-care professional to discuss this.
At the Boden Group, Charles Perkins Centre, we are studying the science of obesity and running clinical trials for weight loss. You can register here to express your interest.
Nick Fuller, Charles Perkins Centre Research Program Leader, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Healthy Made Simple – by Ella Mills
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Often, cookbooks leave a gap between “add the beans to the rice, then microwave” and “delicately embarrass the green-shooted scallions with assiduous garlic before adding to the matelote of orrazata flamed in Sapient Pear Brandy”. This book fills that gap:
It has dishes good for entertaining, and dishes good for eating on a Tuesday night after a long day. Sometimes, they’re even the same dishes.
It has a focus on what’s pleasing, easy, healthy, and consistent with being cooked in a real home kitchen for real people.
The book offers 75 recipes that:
- Take under 30 minutes to make*
- Contain 10 ingredients or fewer
- Have no more than 5 steps
- Are healthy and packed with goodness
- Are delicious and flavorful
*With a selection for under 15 minutes, too!
A strength of the book is that it’s based on practical, real-world cooking, and as such, there are sections such as “Prep-ahead [meals]”, and “cook once, eat twice”, etc.
Just because one is cooking with simple fresh ingredients doesn’t mean that everything bought today must be used today!
Bottom line: if you’d like simple, healthy recipe ideas that lend themselves well to home-cooking and prepping ahead / enjoying leftovers the next day, this is an excellent book for you.
Click here to check out Healthy Made Simple, enjoy the benefits to your health, the easy way!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: