Black Beans vs Soy Beans – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing black beans to soy beans, we picked the soy.
Why?
Quite some heavyweights competing here today, as both have been the winners of other comparisons!
Comparing these two’s macros first, black beans have 3x the carbs and slightly more fiber, while soy has more than 2x the protein. We’ll call this a win for soy.
As a tangential note, it’s worth remembering also that soy is a complete protein (contains a full set of the amino acids we need), whereas black beans… Well, technically they are too, but in practicality, they only have much smaller amounts of some amino acids.
In terms of vitamins, black beans have more of vitamins B1, B3, B5, B9, and E, while soy beans have more of vitamins A, B2, B6, C, K, and choline. A marginal win for soy here.
In the category of minerals, however, it isn’t close: black beans are not higher in any minerals, while soy beans are higher in calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. An overwhelming win for soy.
It should be noted, however, that black beans are still very good for minerals! They just look bad when standing next to soy, that’s all.
So, enjoy either or both, but for nutritional density, soy wins the day.
Want to learn more?
You might like to read:
Plant vs Animal Protein: Head to Head
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Hate Sit-Ups? Try This 10-Minute Standing Abs Routine!

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Abdominal muscles are important to many people for aesthetics; they also fulfil the important role of keeping your innards in, as well as being a critical part of core stability (and you cannot have a truly healthy back without healthy abs on the other side). However, not everyone loves sit-ups and their many variations, so here’s an all-standing workout instead:
On your feet!
The exercise are as follows:
- High knees: engage core to work abs; do slow for low impact. Great for speeding up the metabolism. Jog during rest to keep moving.
- Extend & twist: raise arms high, drive them down while raising one leg into a twist. No rest, switch sides immediately.
- Extend & vertical crunch: extend leg back, drive knee forward into a crunch. Swap sides with no breaks.
- Oblique jacks: jump or slow version; targeting the obliques.
- Front toe-touch: engage core for effectiveness.
- Crossover toe-touch: no break; move into this directly from the front toe-touch.
- Wood chop: lift arms up, twist, chop down. Great for obliques. No rest between sides.
- Heisman: step side to side, bringing your other knee up towards the opposite side. Focus on core engagement rather than speed.
- Side leg raise & side bent: raise leg to side with slight bend; works obliques. No rest between sides.
That’s it!
For a visual demonstration, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Is A Visible Six-Pack Obtainable Regardless Of Genetic Predisposition?
Take care!
Share This Post
-

Kale vs Watercress – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kale to watercress, we picked the kale.
Why?
It was very close! If ever we’ve been tempted to call something a tie, this has been the closest so far.
Their macros are close; watercress has a tiny amount more protein and slightly lower carbs, but these numbers are tiny, so it’s not really a factor. Nevertheless, on macros alone we’d call this a slight nominal win for watercress.
In terms of vitamins, they’re even. Watercress has higher vitamin E and choline (sometimes considered a vitamin), as well as being higher in some B vitamins. Kale has higher vitamins A and K, as well as being higher in some other B vitamins.
In the category of minerals, watercress has higher calcium, magnesium, phosphorus, and potassium, while kale has higher copper, iron, manganese, and zinc. The margins are slightly wider for kale’s more plentiful minerals though, so we’ll call this section a marginal win for kale.
When it comes to polyphenols, kale takes and maintains the lead here, with around 2x the quercetin and 27x the kaempferol. Watercress does have some lignans that kale doesn’t, but ultimately, kale’s strong flavonoid content keeps it in the lead.
So of course: enjoy both if both are available! But if we must pick one, it’s kale.
Want to learn more?
You might like to read:
- Fight Inflammation & Protect Your Brain, With Quercetin
- Spinach vs Kale – Which is Healthier?
- Thai-Style Kale Chips (recipe)
Take care!
Share This Post
-

How Are You, Really?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How Are You, Really? The Free NHS Health Test
We took this surprisingly incisive 10-minute test from the UK’s famous National Health Service—the test is part of the “Better Health” programme, a free-to-all (yes, even those from/in other countries) initiative aimed at keeping people healthy enough to have less need of medical attention.
As one person who took the test wrote:
❝I didn’t expect that a government initiative would have me talking about how I need to keep myself going to be there for the people I love, let alone that a rapid-pace multiple-choice test would elicit these responses and give personalized replies in turn, but here we are❞
It goes beyond covering the usual bases, in that it also looks at what’s most important to you, and why, and what might keep you from doing the things you want/need to do for your health, AND how those obstacles can be overcome.
Pretty impressive for a 10-minute test!
Is Your Health Above Average Already? Take the Free 10-minute NHS test now!
How old are you, in your heart?
Poetic answers notwithstanding (this writer sometimes feels so old, and yet also much younger than she is), there’s a biological answer here, too.
Again free for the use of all*, here’s a heart age calculator.
*It is suitable for you if you are aged 30–95, and do not have a known complicating cardiovascular disease.
It will ask you your (UK) postcode; just leave that field blank if you’re not in the UK; it’ll be fine.
How Old Are You, In Your Heart? Take the Free 10-minute NHS test now!
(Neither test requires logging into anything, and they do not ask for your email address. The tests are right there on the page, and they give the answers right there on the page, immediately)
Share This Post


Related Posts
-
What’s the difference between a heart attack and cardiac arrest? One’s about plumbing, the other wiring
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In July 2023, rising US basketball star Bronny James collapsed on the court during practice and was sent to hospital. The 18-year-old athlete, son of famous LA Lakers’ veteran LeBron James, had experienced a cardiac arrest.
Many media outlets incorrectly referred to the event as a “heart attack” or used the terms interchangeably.
A cardiac arrest and a heart attack are distinct yet overlapping concepts associated with the heart.
With some background in how the heart works, we can see how they differ and how they’re related.

Explode/Shutterstock Understanding the heart
The heart is a muscle that contracts to work as a pump. When it contracts it pushes blood – containing oxygen and nutrients – to all the tissues of our body.
For the heart muscle to work effectively as a pump, it needs to be fed its own blood supply, delivered by the coronary arteries. If these arteries are blocked, the heart muscle doesn’t get the blood it needs.
This can cause the heart muscle to become injured or die, and results in the heart not pumping properly.
Heart attack or cardiac arrest?
Simply put, a heart attack, technically known as a myocardial infarction, describes injury to, or death of, the heart muscle.
A cardiac arrest, sometimes called a sudden cardiac arrest, is when the heart stops beating, or put another way, stops working as an effective pump.
In other words, both relate to the heart not working as it should, but for different reasons. As we’ll see later, one can lead to the other.
Why do they happen? Who’s at risk?
Heart attacks typically result from blockages in the coronary arteries. Sometimes this is called coronary artery disease, but in Australia, we tend to refer to it as ischaemic heart disease.
The underlying cause in about 75% of people is a process called atherosclerosis. This is where fatty and fibrous tissue build up in the walls of the coronary arteries, forming a plaque. The plaque can block the blood vessel or, in some instances, lead to the formation of a blood clot.
Atherosclerosis is a long-term, stealthy process, with a number of risk factors that can sneak up on anyone. High blood pressure, high cholesterol, diet, diabetes, stress, and your genes have all been implicated in this plaque-building process.
Other causes of heart attacks include spasms of the coronary arteries (causing them to constrict), chest trauma, or anything else that reduces blood flow to the heart muscle.
Regardless of the cause, blocking or reducing the flow of blood through these pipes can result in the heart muscle not receiving enough oxygen and nutrients. So cells in the heart muscle can be injured or die.
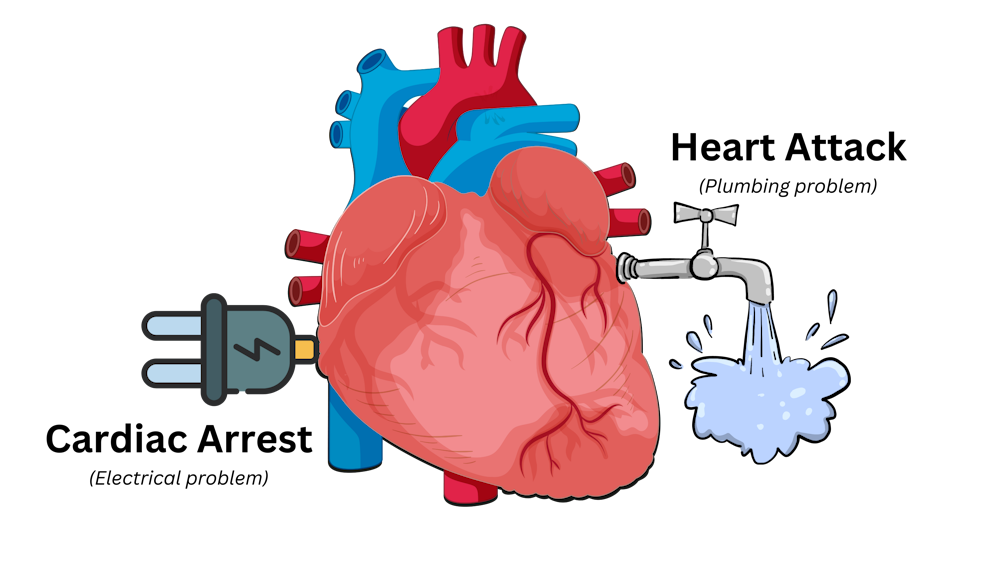
Here’s a simple way to remember the difference. Author provided But a cardiac arrest is the result of heartbeat irregularities, making it harder for the heart to pump blood effectively around the body. These heartbeat irregularities are generally due to electrical malfunctions in the heart. There are four distinct types:
- ventricular tachycardia: a rapid and abnormal heart rhythm in which the heartbeat is more than 100 beats per minute (normal adult, resting heart rate is generally 60-90 beats per minute). This fast heart rate prevents the heart from filling with blood and thus pumping adequately
- ventricular fibrillation: instead of regular beats, the heart quivers or “fibrillates”, resembling a bag of worms, resulting in an irregular heartbeat greater than 300 beats per minute
- pulseless electrical activity: arises when the heart muscle fails to generate sufficient pumping force after electrical stimulation, resulting in no pulse
- asystole: the classic flat-line heart rhythm you see in movies, indicating no electrical activity in the heart.
Remember this flat-line rhythm from the movies? It’s asystole, when there’s no electrical activity in the heart. Kateryna Kon/Shutterstock Cardiac arrest can arise from numerous underlying conditions, both heart-related and not, such as drowning, trauma, asphyxia, electrical shock and drug overdose. James’ cardiac arrest was attributed to a congenital heart defect, a heart condition he was born with.
But among the many causes of a cardiac arrest, ischaemic heart disease, such as a heart attack, stands out as the most common cause, accounting for 70% of all cases.
So how can a heart attack cause a cardiac arrest? You’ll remember that during a heart attack, heart muscle can be damaged or parts of it may die. This damaged or dead tissue can disrupt the heart’s ability to conduct electrical signals, increasing the risk of developing arrhythmias, possibly causing a cardiac arrest.
So while a heart attack is a common cause of cardiac arrest, a cardiac arrest generally does not cause a heart attack.
What do they look like?
Because a cardiac arrest results in the sudden loss of effective heart pumping, the most common signs and symptoms are a sudden loss of consciousness, absence of pulse or heartbeat, stopping of breathing, and pale or blue-tinged skin.
But the common signs and symptoms of a heart attack include chest pain or discomfort, which can show up in other regions of the body such as the arms, back, neck, jaw, or stomach. Also frequent are shortness of breath, nausea, light-headedness, looking pale, and sweating.
What’s the take-home message?
While both heart attack and cardiac arrest are disorders related to the heart, they differ in their mechanisms and outcomes.
A heart attack is like a blockage in the plumbing supplying water to a house. But a cardiac arrest is like an electrical malfunction in the house’s wiring.
Despite their different nature both conditions can have severe consequences and require immediate medical attention.
Michael Todorovic, Associate Professor of Medicine, Bond University and Matthew Barton, Senior lecturer, School of Nursing and Midwifery, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Podiatrists Debunk 11 Feet Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Podiatrists Dr. Sarah Haller and Dr. Brad Schaeffer put us on a better path:
Don’t get wrong-footed
We’ll not keep the 11 myths a mystery; they are…
- “You have warts because your feet are dirty.”
False! Warts are caused by a virus, not dirt. Viruses can be picked up from surfaces like yoga mats, pools, gyms, and showers. - “Bunions are caused by wearing heels.”
False! Bunions are genetic deformities where the bone behind the big toe shifts. Heels might worsen them but don’t cause them. - “Cutting the sides of my toenail will prevent an ingrown toenail.”
False! Toenails should be cut straight across. Cutting the sides can make ingrown toenails worse. - “Pedicures gave me toenail fungus.”
Partially true! You can get fungus from many places, but safe, sterile pedicures are generally fine. - “Only athletes get athlete’s foot.”
False! Athlete’s foot is a fungal infection caused by warm, moist environments. Anyone can get it, not just athletes. - “My feet are fine because I trained them to walk in stilettos.”
False! You can get used to stilettos, but they aren’t healthy long-term. They shorten the Achilles tendon and put pressure on the foot. - “You can’t do anything for a broken toe.”
False! Broken toes can be treated and should be checked by a doctor. They may need to be set for proper healing. - “It’s normal for your feet to hurt from standing all day.”
False! Foot pain isn’t normal and can be prevented with proper footwear, support, and compression socks. - “All inserts are the same.”
False! Everyone’s feet are different. Some may benefit from over-the-counter insoles, but others need custom orthotics. - “Sprained ankles are no big deal.”
False! Sprains can damage ligaments and lead to instability or arthritis if untreated. Proper stabilization is essential. - “If I can walk after an injury, I don’t need to see a doctor.”
False! You can still have serious injuries like fractures even if you can walk. Always get checked after an injury.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Steps For Keeping Your Feet A Healthy Foundation
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- “You have warts because your feet are dirty.”
-

Exercise with Type 1 Diabetes – by Ginger Vieira
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you or a loved one has Type 1 Diabetes, you’ll know that exercise can be especially frustrating…
- If you don’t do it, you risk weight gain and eventual insulin resistance.
- If you do it, you risk dangerous hypos, or perhaps hypers if you took off your pump or skipped a bolus.
Unfortunately, the popular medical advice is “well, just do your best”.
Ginger Vieira is Type 1 Diabetic, and writes with 20+ experience of managing her diabetes while being a keen exerciser. As T1D folks out there will also know, comorbidities are very common; in her case, fibromyalgia was the biggest additional blow to her ability to exercise, along with an underactive thyroid. So when it comes to dealing with the practical nuts and bolts of things, she (while herself observing she’s not a doctor, let alone your doctor) has a lot more practical knowledge than an endocrinologist (without diabetes) behind a desk.
Speaking of nuts and bolts, this book isn’t a pep talk.
It has a bit of that in, but most of it is really practical information, e.g: using fasted exercise (4 hours from last meal+bolus) to prevent hypos, counterintuitive as that may seem—the key is that timing a workout for when you have the least amount of fast-acting insulin in your body means your body can’t easily use your blood sugars for energy, and draws from your fat reserves instead… Win/Win!
That’s just one quick tip because this is a 1-minute review, but Vieira gives:
- whole chapters, with example datasets (real numbers)
- tech-specific advice, e.g. pump, injection, etc
- insulin-specific advice, e.g. fast vs slow, and adjustments to each in the context of exercise
- timing advice re meal/bolus/exercise for different insulins and techs
- blood-sugar management advice for different exercise types (aerobic/anaerobic, sprint/endurance, etc)
…and lots more that we don’t have room to mention here
Basically… If you or a loved one has T1D, we really recommend this book!
Order a copy of “Exercise with Type 1 Diabetes” from Amazon today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: