Balanced Energy Cake Bars
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Unlike a lot of commercially available products, these bars won’t spike your blood sugars in the same way. There’s technically plenty of sugar in them, mostly from the chopped dates, but they’re also full of fiber, protein, and healthy fats. This means they can give you an energy boost (along with lots of gut-healthy, heart-healthy, and brain-healthy ingredients) without any crash later. They’re also delicious, and make for a great afternoon snack!
You will need
- 1 cup oats
- 15 Medjool dates, pitted and soaked in hot water for 15 minutes
- 3 carrots, grated
- 4oz almond butter
- 2 tbsp tahini
- 2 tbsp flaxseeds, milled
- 1 tbsp sesame seeds, toasted
- Optional: your choice of dried fruit and/or chopped nuts (mix it up; diversity is good!)
Method
(we suggest you read everything at least once before doing anything)
1) Steam the grated carrots for 3–4 minutes; pat dry and allow to cool
2) Drain and pat dry the dates, roughly chop them and add them to a bowl with the carrots. Because we chopped the dates rather than blended them (as many recipes do), they keep their fiber, which is important.
3) Add the oats, seeds, almond butter, and tahini. Also add in any additional dried fruit and/or chopped nuts you selected for the optional part. Mix well; the mixture should be quite firm. If it isn’t, add more oats.
4) Press the mixture into a 10″ square baking tin lined with baking paper. Refrigerate for a few hours, before cutting into bar shapes (or squares if you prefer). These can now be eaten immediately or stored for up to a week.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How light can shift your mood and mental health

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is the next article in our ‘Light and health’ series, where we look at how light affects our physical and mental health in sometimes surprising ways. Read other articles in the series.
It’s spring and you’ve probably noticed a change in when the Sun rises and sets. But have you also noticed a change in your mood?
We’ve known for a while that light plays a role in our wellbeing. Many of us tend to feel more positive when spring returns.
But for others, big changes in light, such as at the start of spring, can be tough. And for many, bright light at night can be a problem. Here’s what’s going on.

llaszlo/Shutterstock An ancient rhythm of light and mood
In an earlier article in our series, we learned that light shining on the back of the eye sends “timing signals” to the brain and the master clock of the circadian system. This clock coordinates our daily (circadian) rhythms.
“Clock genes” also regulate circadian rhythms. These genes control the timing of when many other genes turn on and off during the 24-hour, light-dark cycle.
But how is this all linked with our mood and mental health?
Circadian rhythms can be disrupted. This can happen if there are problems with how the body clock develops or functions, or if someone is routinely exposed to bright light at night.
When circadian disruption happens, it increases the risk of certain mental disorders. These include bipolar disorder and atypical depression (a type of depression when someone is extra sleepy and has problems with their energy and metabolism).
Light on the brain
Light may also affect circuits in the brain that control mood, as animal studies show.
There’s evidence this happens in humans. A brain-imaging study showed exposure to bright light in the daytime while inside the scanner changed the activity of a brain region involved in mood and alertness.
Another brain-imaging study found a link between daily exposure to sunlight and how the neurotransmitter (or chemical messenger) serotonin binds to receptors in the brain. We see alterations in serotonin binding in several mental disorders, including depression.
Our mood can lift in sunlight for a number of reasons, related to our genes, brain and hormones. New Africa/Shutterstock What happens when the seasons change?
Light can also affect mood and mental health as the seasons change. During autumn and winter, symptoms such as low mood and fatigue can develop. But often, once spring and summer come round, these symptoms go away. This is called “seasonality” or, when severe, “seasonal affective disorder”.
What is less well known is that for other people, the change to spring and summer (when there is more light) can also come with a change in mood and mental health. Some people experience increases in energy and the drive to be active. This is positive for some but can be seriously destabilising for others. This too is an example of seasonality.
Most people aren’t very seasonal. But for those who are, seasonality has a genetic component. Relatives of people with seasonal affective disorder are more likely to also experience seasonality.
Seasonality is also more common in conditions such as bipolar disorder. For many people with such conditions, the shift into shorter day-lengths during winter can trigger a depressive episode.
Counterintuitively, the longer day-lengths in spring and summer can also destabilise people with bipolar disorder into an “activated” state where energy and activity are in overdrive, and symptoms are harder to manage. So, seasonality can be serious.
Alexis Hutcheon, who experiences seasonality and helped write this article, told us:
[…] the season change is like preparing for battle – I never know what’s coming, and I rarely come out unscathed. I’ve experienced both hypomanic and depressive episodes triggered by the season change, but regardless of whether I’m on the ‘up’ or the ‘down’, the one constant is that I can’t sleep. To manage, I try to stick to a strict routine, tweak medication, maximise my exposure to light, and always stay tuned in to those subtle shifts in mood. It’s a time of heightened awareness and trying to stay one step ahead.
So what’s going on in the brain?
One explanation for what’s going on in the brain when mental health fluctuates with the change in seasons relates to the neurotransmitters serotonin and dopamine.
Serotonin helps regulate mood and is the target of many antidepressants. There is some evidence of seasonal changes in serotonin levels, potentially being lower in winter.
Dopamine is a neurotransmitter involved in reward, motivation and movement, and is also a target of some antidepressants. Levels of dopamine may also change with the seasons.
But the neuroscience of seasonality is a developing area and more research is needed to know what’s going on in the brain.
How about bright light at night?
We know exposure to bright light at night (for instance, if someone is up all night) can disturb someone’s circadian rhythms.
This type of circadian rhythm disturbance is associated with higher rates of symptoms including self-harm, depressive and anxiety symptoms, and lower wellbeing. It is also associated with higher rates of mental disorders, such as major depression, bipolar disorder, psychotic disorders and post-traumatic stress disorder (or PTSD).
Why is this? Bright light at night confuses and destabilises the body clock. It disrupts the rhythmic regulation of mood, cognition, appetite, metabolism and many other mental processes.
But people differ hugely in their sensitivity to light. While still a hypothesis, people who are most sensitive to light may be the most vulnerable to body clock disturbances caused by bright light at night, which then leads to a higher risk of mental health problems.
Bright light at night disrupts your body clock, putting you at greater risk of mental health issues. Ollyy/Shutterstock Where to from here?
Learning about light will help people better manage their mental health conditions.
By encouraging people to better align their lives to the light-dark cycle (to stabilise their body clock) we may also help prevent conditions such as depression and bipolar disorder emerging in the first place.
Healthy light behaviours – avoiding light at night and seeking light during the day – are good for everyone. But they might be especially helpful for people at risk of mental health problems. These include people with a family history of mental health problems or people who are night owls (late sleepers and late risers), who are more at risk of body clock disturbances.
Alexis Hutcheon has lived experience of a mental health condition and helped write this article.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14.
Jacob Crouse, Research Fellow in Youth Mental Health, Brain and Mind Centre, University of Sydney; Emiliana Tonini, Postdoctoral Research Fellow, Brain and Mind Centre, University of Sydney, and Ian Hickie, Co-Director, Health and Policy, Brain and Mind Centre, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

A short history of sunscreen, from basting like a chook to preventing skin cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australians have used commercial creams, lotions or gels to manage our skin’s sun exposure for nearly a century.
But why we do it, the preparations themselves, and whether they work, has changed over time.
In this short history of sunscreen in Australia, we look at how we’ve slathered, slopped and spritzed our skin for sometimes surprising reasons.
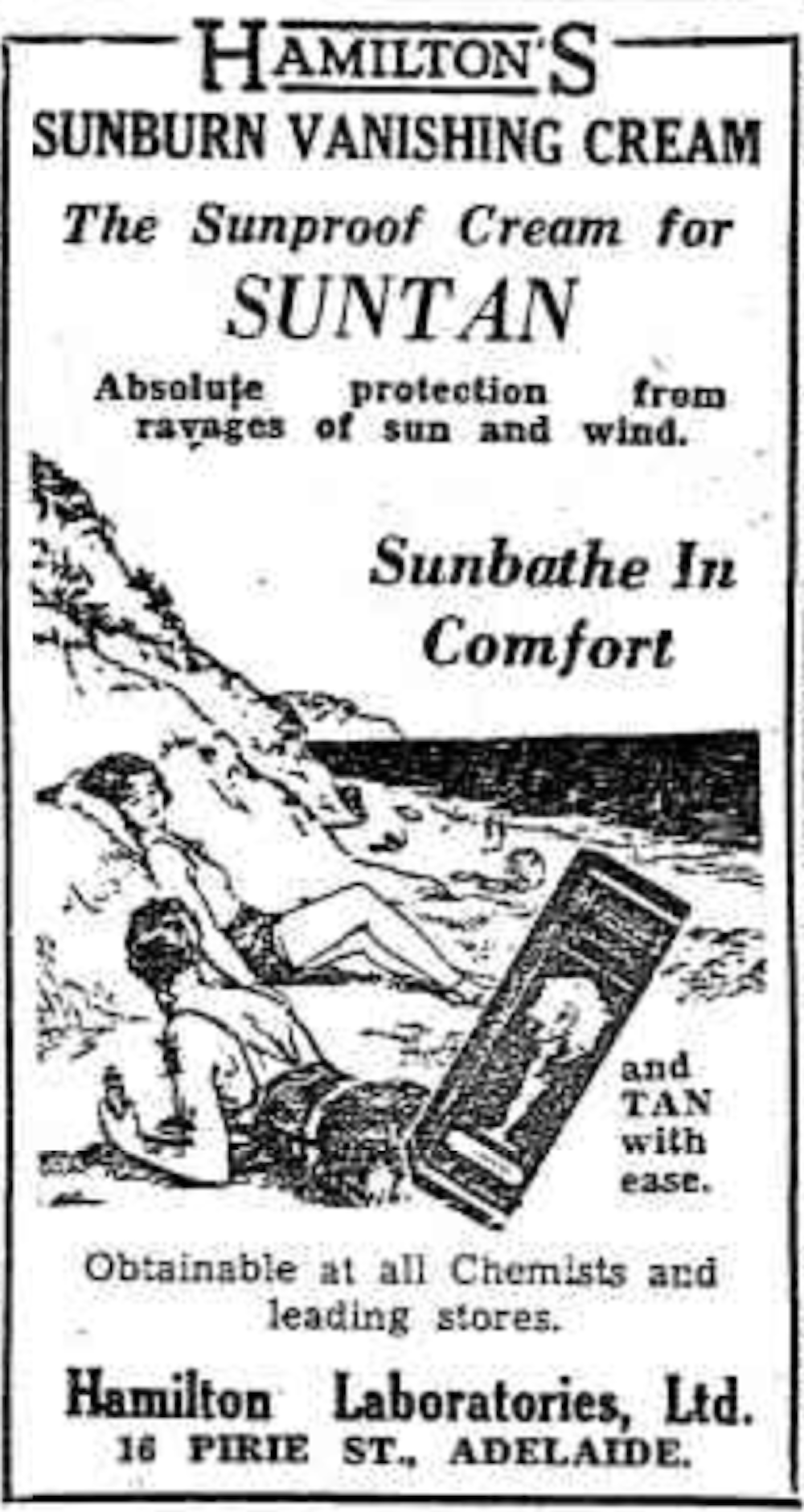
At first, suncreams helped you ‘tan with ease’

This early sunscreen claimed you could ‘tan with ease’.
Trove/NLASunscreens have been available in Australia since the 30s. Chemist Milton Blake made one of the first.
He used a kerosene heater to cook batches of “sunburn vanishing cream”, scented with French perfume.
His backyard business became H.A. Milton (Hamilton) Laboratories, which still makes sunscreens today.
Hamilton’s first cream claimed you could “
Sunbathe in Comfort and TAN with ease”. According to modern standards, it would have had an SPF (or sun protection factor) of 2.The mirage of ‘safe tanning’
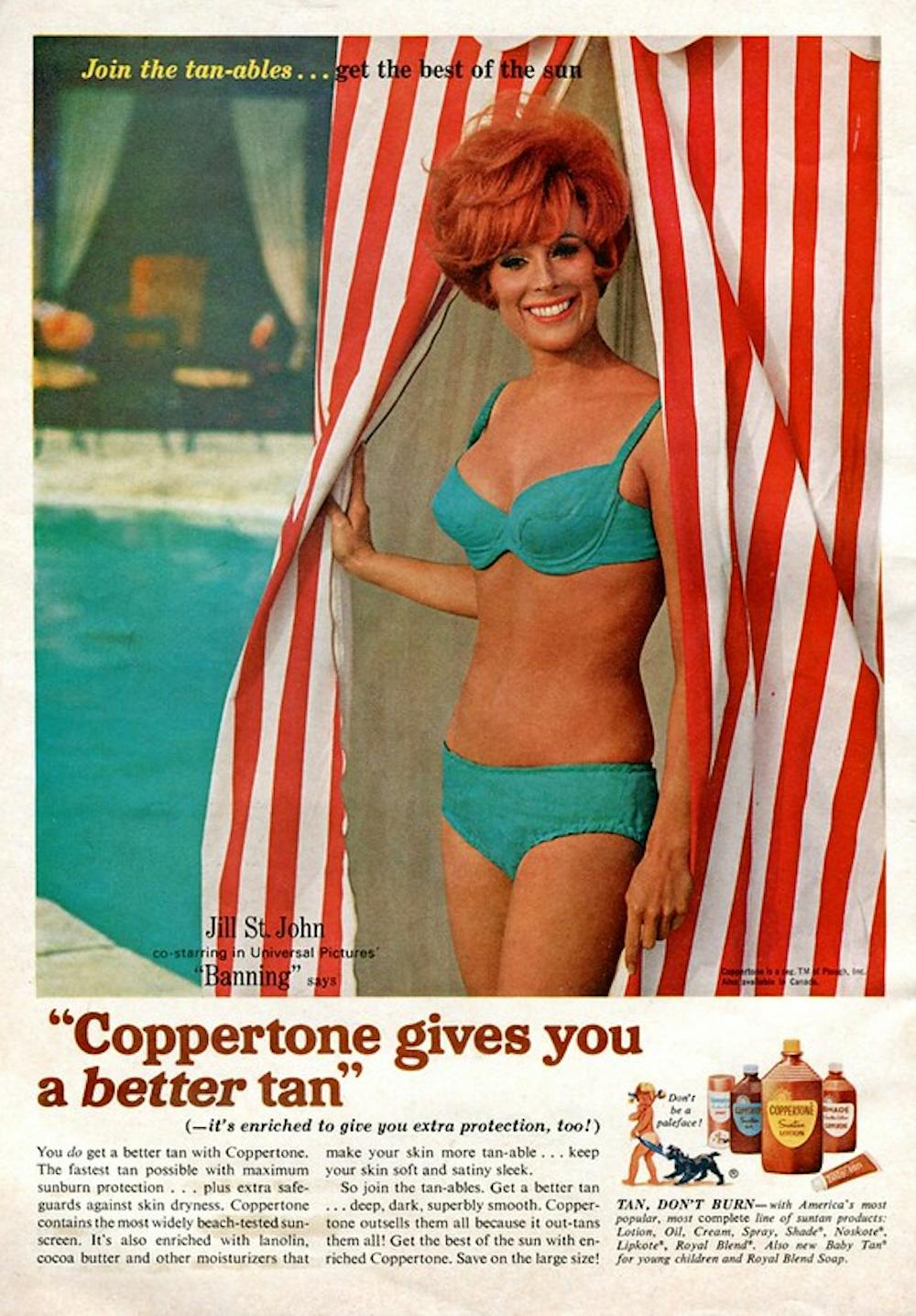
A tan was considered a “modern complexion” and for most of the 20th century, you might put something on your skin to help gain one. That’s when “safe tanning” (without burning) was thought possible.

This 1967 Coppertone advertisement urged you to ‘tan, not burn’.
SenseiAlan/Flickr, CC BY-SASunburn was known to be caused by the UVB component of ultraviolet (UV) light. UVA, however, was thought not to be involved in burning; it was just thought to darken the skin pigment melanin. So, medical authorities advised that by using a sunscreen that filtered out UVB, you could “safely tan” without burning.
But that was wrong.
From the 70s, medical research suggested UVA penetrated damagingly deep into the skin, causing ageing effects such as sunspots and wrinkles. And both UVA and UVB could cause skin cancer.
Sunscreens from the 80s sought to be “broad spectrum” – they filtered both UVB and UVA.
Researchers consequently recommended sunscreens for all skin tones, including for preventing sun damage in people with dark skin.
Delaying burning … or encouraging it?
Up to the 80s, sun preparations ranged from something that claimed to delay burning, to preparations that actively encouraged it to get that desirable tan – think, baby oil or coconut oil. Sun-worshippers even raided the kitchen cabinet, slicking olive oil on their skin.
One manufacturer’s “sun lotion” might effectively filter UVB; another’s merely basted you like a roast chicken.
Since labelling laws before the 80s didn’t require manufacturers to list the ingredients, it was often hard for consumers to tell which was which.
At last, SPF arrives to guide consumers
In the 70s, two Queensland researchers, Gordon Groves and Don Robertson, developed tests for sunscreens – sometimes experimenting on students or colleagues. They printed their ranking in the newspaper, which the public could use to choose a product.
An Australian sunscreen manufacturer then asked the federal health department to regulate the industry. The company wanted standard definitions to market their products, backed up by consistent lab testing methods.
In 1986, after years of consultation with manufacturers, researchers and consumers, Australian Standard AS2604 gave a specified a testing method, based on the Queensland researchers’ work. We also had a way of expressing how well sunscreens worked – the sun protection factor or SPF.
This is the ratio of how long it takes a fair-skinned person to burn using the product compared with how long it takes to burn without it. So a cream that protects the skin sufficiently so it takes 40 minutes to burn instead of 20 minutes has an SPF of 2.
Manufacturers liked SPF because businesses that invested in clever chemistry could distinguish themselves in marketing. Consumers liked SPF because it was easy to understand – the higher the number, the better the protection.
Australians, encouraged from 1981 by the Slip! Slop! Slap! nationwide skin cancer campaign, could now “slop” on a sunscreen knowing the degree of protection it offered.
How about skin cancer?
It wasn’t until 1999 that research proved that using sunscreen prevents skin cancer. Again, we have Queensland to thank, specifically the residents of Nambour. They took part in a trial for nearly five years, carried out by a research team led by Adele Green of the Queensland Institute of Medical Research. Using sunscreen daily over that time reduced rates of squamous cell carcinoma (a common form of skin cancer) by about 60%.
Follow-up studies in 2011 and 2013 showed regular sunscreen use almost halved the rate of melanoma and slowed skin ageing. But there was no impact on rates of basal cell carcinoma, another common skin cancer.
By then, researchers had shown sunscreen stopped sunburn, and stopping sunburn would prevent at least some types of skin cancer.
What’s in sunscreen today?
An effective sunscreen uses one or more active ingredients in a cream, lotion or gel. The active ingredient either works:
-
“chemically” by absorbing UV and converting it to heat. Examples include PABA (para-aminobenzoic acid) and benzyl salicylate, or
-
“physically” by blocking the UV, such as zinc oxide or titanium dioxide.
Physical blockers at first had limited cosmetic appeal because they were opaque pastes. (Think cricketers with zinc smeared on their noses.)
With microfine particle technology from the 90s, sunscreen manufacturers could then use a combination of chemical absorbers and physical blockers to achieve high degrees of sun protection in a cosmetically acceptable formulation.
Where now?
Australians have embraced sunscreen, but they still don’t apply enough or reapply often enough.
Although some people are concerned sunscreen will block the skin’s ability to make vitamin D this is unlikely. That’s because even SPF50 sunscreen doesn’t filter out all UVB.
There’s also concern about the active ingredients in sunscreen getting into the environment and whether their absorption by our bodies is a problem.
Sunscreens have evolved from something that at best offered mild protection to effective, easy-to-use products that stave off the harmful effects of UV. They’ve evolved from something only people with fair skin used to a product for anyone.
Remember, slopping on sunscreen is just one part of sun protection. Don’t forget to also slip (protective clothing), slap (hat), seek (shade) and slide (sunglasses).

Laura Dawes, Research Fellow in Medico-Legal History, Australian National University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
-
For Many Rural Women, Finding Maternity Care Outweighs Concerns About Abortion Access
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
BAKER CITY, Ore. — In what has become a routine event in rural America, a hospital maternity ward closed in 2023 in this small Oregon town about an hour from the Idaho border.
For Shyanne McCoy, 23, that meant the closest hospital with an obstetrician on staff when she was pregnant was a 45-mile drive away over a mountain pass.
When McCoy developed symptoms of preeclampsia last January, she felt she had the best chance of getting the care she needed at a larger hospital in Boise, Idaho, two hours away. She spent the final week of her pregnancy there, too far from home to risk leaving, before giving birth to her daughter.
Six months later, she said it seems clear to her that the health care needs of rural young women like her are largely ignored.
For McCoy and others, figuring out how to obtain adequate care to safely have a baby in Baker City has quickly eclipsed concerns about another medical service lacking in the area: abortion. But in Oregon and elsewhere in the country, progressive lawmakers’ attempts to expand abortion access sometimes clash with rural constituencies.
Oregon is considered one of the most protective states in the country when it comes to abortion. There are no legal limits on when someone can receive an abortion in the state, and the service is covered by its Medicaid system. Still, efforts to expand access in the rural, largely conservative areas that cover most of the state have encountered resistance and incredulity.
It’s a divide that has played out in elections in such states as Nevada, where voters passed a ballot measure in November that seeks to codify abortion protections in the state constitution. Residents in several rural counties opposed the measure.
In Oregon, during the months just before the Baker City closure was announced, Democratic state lawmakers were focused on a proposed pilot program that would launch two mobile reproductive health care clinics in rural areas. The bill specified that the van-based clinics would include abortion services.
State Rep. Christine Goodwin, a Republican from a southwestern Oregon district, called the proposal the “latest example” of urban legislators telling rural leaders what their communities need.
The mobile health clinic pilot was eventually removed from the bill that was under discussion. That means no new abortion options in Oregon’s Baker County — and no new state-funded maternity care either.
“I think if you expanded rural access in this community to abortions before you extended access to maternal health care, you would have an uprising on your hands,” said Paige Witham, 27, a member of the Baker County health care steering committee and the mother of two children, including an infant born in October.
A study published in JAMA in early December that examined nearly 5,000 acute care hospitals found that by 2022, 52% of rural hospitals lacked obstetrics care after more than a decade of unit closures. The health implications of those closures for young women, the population most likely to need pregnancy care, and their babies can be significant. Research has shown that added distance between a patient and obstetric care increases the likelihood the baby will be admitted to a neonatal intensive care unit, or NICU.
Witham said that while she does not support abortion, she believes the government should not “legislate it away completely.” She said that unless the government provides far more support for young families, like free child care and better mental health care, abortion should remain legal.
Conversations with a liberal school board member, a moderate owner of a timber company, members of Baker City’s Republican Party chapter, a local doula, several pregnant women, and the director of the Baker County Health Department — many of whom were not rigidly opposed to abortion — all turned up the same answer: No mobile clinics offering abortions here, please.
Kelle Osborn, a nurse supervisor for the Baker County Health Department, loved the idea of a mobile clinic that would provide education and birth control services to people in outlying areas. She was less thrilled about including abortion services in a clinic on wheels.
“It’s not something that should just be handed out from a mobile van,” she said of abortion services. She said people in her conservative rural county would probably avoid using the clinics for anything if they were understood to provide abortion services.
Both Osborn and Meghan Chancey, the health department’s director, said they would rank many health care priorities higher, including the need for a general surgeon, an ICU, and a dialysis clinic.
Nationally, reproductive health care services of all types tend to be limited for people in rural areas, even within states that protect abortion access. More than two-thirds of people in “maternity care deserts” — all of which are in rural counties — must drive more than a half-hour to get obstetric care, according to a 2024 March of Dimes report. For people in the Southern states where lawmakers installed abortion bans, abortion care can be up to 700 miles away, according to a data analysis by Axios.
Nathan Defrees grew up in Baker City and has practiced medicine here since 2017. He works for a family medicine clinic. If a patient asks about abortion, he provides information about where and how one can be obtained, but he doesn’t offer abortions himself.
“There’s not a lot of anonymity in small towns for physicians who provide that care,” he said. “Many of us aren’t willing to sacrifice the rest of our career for that.”
He also pointed to the small number of patients requesting the service locally. Just six people living in Baker County had an abortion in 2023, according to data from the Oregon Department of Public Health. Meanwhile, 125 residents had a baby that year.
A doctor with obstetric training living in another rural part of the state has chosen to quietly provide early-stage abortions when asked. The doctor, concerned for their family’s safety in the small, conservative town where they live, asked not to be identified.
The idea that better access to abortion is not needed in rural areas seems naive, the doctor said. People most in need of abortion often don’t have access to any medical service not already available in town, the doctor pointed out. The first patient the doctor provided an abortion for at the clinic was a meth user with no resources to travel or to manage an at-home medication abortion.
“It seemed entirely inappropriate for me to turn her away for care I had the training and the tools to do,” the doctor said.
Defrees said it has been easier for Baker County residents to get an abortion since the U.S. Supreme Court overturned Roe v. Wade.
A new Planned Parenthood clinic in Ontario, Oregon, 70 miles away in neighboring Malheur County, was built primarily to provide services to people from the Boise metro area, but it also created an option for many living in rural eastern Oregon.
Idaho is one of the 16 states with near-total bans on abortion. Like many states with bans, Idaho has struggled to maintain its already small fleet of fetal medicine doctors. The loss of regional expertise touches Baker City, too, Defrees said.
For example, he said, the treatment plan for women who have a desired pregnancy but need a termination for medical reasons is now far less clear. “It used to be those folks could go to Boise,” he said. “Now they can’t. That does put us in a bind.”
Portland is the next closest option for that type of care, and that means a 300-mile drive along a set of highways that can be treacherous in winter.
“It’s a lot scarier to be pregnant now in Baker City than it ever has been,” Defrees said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post



Related Posts
-
12 Things Your Urine Says About Your Health (Test At Home)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Urine has been used to assess health since Ancient Egypt (fun fact: because of Egyptian language having multiple sounds that get transliterated to “a” in English, the condition of passing blood in one’s urine was known as “Aaaaa” ← this word has three syllables; “Aa-a-aa”).
Modern techniques are more advanced than those of times past (for example, diabetes is no longer diagnosed by a urine taste-test), but basic urine inspection is still a very useful indicator of many things. Recognizing changes in urine can even help detect life-threatening conditions early:
Traffic lights?
How urine works: water that we consume is absorbed into the bloodstream and filtered by the kidneys. Urine is essentially blood with actual the blood cells filtered out and/or broken down. The yellow color comes from urochrome, produced during red blood cell breakdown. Here’s how things can happen a little differently:
- Fluorescent yellow: caused by excess vitamin B2 from supplements; harmless.
- Red urine: can indicate blood (bladder cancer, UTIs), hemoglobin, or myoglobin; seek medical attention.
- Dark brown/tea-colored urine: may result from muscle damage or blood cell destruction; requires evaluation.
- Orange urine: caused by dehydration, medications, or liver/bile duct issues (if paired with pale stools).
- Purple urine: UTI bacteria produce pigments that can cause this; treatable with antibiotics.
- Green urine: rare; caused by medications or dyes like methylene blue.
- Frothy/foamy urine: indicates high protein levels, often from kidney damage (e.g. per diabetes and/or hypertension).
- Crystal-clear urine: suggests overhydration, which can dangerously lower sodium levels.
- Dark yellow/amber urine: may mean dehydration; drink more water to maintain a light yellow color.
- Not peeing enough: may indicate severe dehydration or kidney failure; urgent medical attention needed.
- Peeing too much: often linked to diabetes or excessive water intake; can lead to dehydration or low sodium.
- Color-changing urine: port wine color signals porphyria; black urine indicates alkaptonuria (oxidation of homogentisic acid). Both are serious.
Bonus: if you eat a lot of beetroot and then your urine is pink/red/purple, that’s probably just the pigments passing through. If it persists though, then of course, see above.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Why You Don’t Need 8 Glasses Of Water Per Day
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

To-Do List Formula – by Damon Zahariades
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The first part of this book is given to reviewing popular to-do list methods that are already widely “out there”. This treatment is practical and exploratory, looking at the pros and cons of each.
The second part of the book is more Zahariades’ own method, taking what he sees as the best of each, plus some tricks and practices of his own. With these, he builds (and shares!) his optimized system.
You may be wondering what you, dear reader, can expect to get out of this book. Well, that depends on where you’re coming from:
Are you new to approaching your general to-dos with a system more organized than post-it notes on your fridge? If so, this will be a great initial introduction to many systems.
Or are you, perhaps, a veteran of GTD, ToDoist, assorted Pomodoro-based systems, and more? Do you do/delegate/defer/ditch tasks more deftly and dextrously than Serena Williams despatches tennis balls?
If so, what you’re more likely to gain here is a fresh perspective on old ideas, and maybe a trick or two you didn’t know before. At the very least, a boost to your motivation, getting you fired up for doing what you know best again.
All in all, a very respectable book for anyone’s to-read list!
Pick Up Your Copy of Zahariades’ To-Do List Formula on Amazon Today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The CBT Workbook for Mental Health – by Dr. Simon Rego & Sarah Fader
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have often reviewed psychology books here with a note saying “and no, it’s not just a book of the standard CBT techniques that you probably already know”.
So today, this one’s for anyone who was ever thinking “but I don’t know the standard CBT techniques and I would like to know them!”.
The authors outline specific solutions to many common quantifiable problems, with simple exercises that are well-explained and easy to implement.
Cognitive Behavioral Therapy (CBT) is not a panacea, but for the things it can be used for, it’s very effective and is a very good “first thing to reach for” to see if it works, because its success rate for a lot of problems is very high.
What kinds of things is this book most likely to help with? A lot of common forms of stress, anxiety, self-esteem issues, cravings, shame, and relationship issues. Other things too, but we can’t list everything and that list already covers a lot of very high-incidence stuff.
Bottom line: if CBT isn’t something already in your toolbox, this book will help you add all its best tips and tricks.
Click here to check out The CBT Workbook for Mental Health, and get tooled up!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: