We created a VR tool to test brain function. It could one day help diagnose dementia
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you or a loved one have noticed changes in your memory or thinking as you’ve grown older, this could reflect typical changes that occur with ageing. In some cases though, it might suggest something more, such as the onset of dementia.
The best thing to do if you have concerns is to make an appointment with your GP, who will probably run some tests. Assessment is important because if there is something more going on, early diagnosis can enable prompt access to the right interventions, supports and care.
But current methods of dementia screening have limitations, and testing can be daunting for patients.
Our research suggests virtual reality (VR) could be a useful cognitive screening tool, and mitigate some of the challenges associated with current testing methods, opening up the possibility it may one day play a role in dementia diagnosis.
Where current testing is falling short
If someone is worried about their memory and thinking, their GP might ask them to complete a series of quick tasks that check things like the ability to follow simple instructions, basic arithmetic, memory and orientation.
These sorts of screening tools are really good at confirming cognitive problems that may already be very apparent. But commonly used screening tests are not always so good at detecting early and more subtle difficulties with memory and thinking, meaning such changes could be missed until they get worse.
A clinical neuropsychological assessment is better equipped to detect early changes. This involves a comprehensive review of a patient’s personal and medical history, and detailed assessment of cognitive functions, including attention, language, memory, executive functioning, mood factors and more. However, this can be costly and the testing can take several hours.
Testing is also somewhat removed from everyday experience, not directly tapping into activities of daily living.
Enter virtual reality
VR technology uses computer-generated environments to create immersive experiences that feel like real life. While VR is often used for entertainment, it has increasingly found applications in health care, including in rehabilitation and falls prevention.
Using VR for cognitive screening is still a new area. VR-based cognitive tests generally create a scenario such as shopping at a supermarket or driving around a city to ascertain how a person would perform in these situations.
Notably, they engage various senses and cognitive processes such as sight, sound and spatial awareness in immersive ways. All this may reveal subtle impairments which can be missed by standard methods.
VR assessments are also often more engaging and enjoyable, potentially reducing anxiety for those who may feel uneasy in traditional testing environments, and improving compliance compared to standard assessments.

pikselstock/Shutterstock
Most studies of VR-based cognitive tests have explored their capacity to pick up impairments in spatial memory (the ability to remember where something is located and how to get there), and the results have been promising.
Given VR’s potential for assisting with diagnosis of cognitive impairment and dementia remains largely untapped, our team developed an online computerised game (referred to as semi-immersive VR) to see how well a person can remember, recall and complete everyday tasks. In our VR game, which lasts about 20 minutes, the user role plays a waiter in a cafe and receives a score on their performance.
To assess its potential, we enlisted more than 140 people to play the game and provide feedback. The results of this research are published across three recent papers.
Testing our VR tool
In our most recently published study, we wanted to verify the accuracy and sensitivity of our VR game to assess cognitive abilities.
We compared our test to an existing screening tool (called the TICS-M) in more than 130 adults. We found our VR task was able to capture meaningful aspects of cognitive function, including recalling food items and spatial memory.
We also found younger adults performed better in the game than older adults, which echoes the pattern commonly seen in regular memory tests.

pikselstock/Shutterstock
In a separate study, we followed ten adults aged over 65 while they completed the game, and interviewed them afterwards. We wanted to understand how this group – who the tool would target – perceived the task.
These seniors told us they found the game user-friendly and believed it was a promising tool for screening memory. They described the game as engaging and immersive, expressing enthusiasm to continue playing. They didn’t find the task created anxiety.
For a third study, we spoke to seven health-care professionals about the tool. Overall they gave positive feedback, and noted its dynamic approach to age-old diagnostic challenges.
However, they did flag some concerns and potential barriers to implementing this sort of tool. These included resource constraints in clinical practice (such as time and space to carry out the assessment) and whether it would be accessible for people with limited technological skills. There was also some scepticism about whether the tool would be an accurate method to assist with dementia diagnosis.
While our initial research suggests this tool could be a promising way to assess cognitive performance, this is not the same as diagnosing dementia. To improve the test’s ability to accurately detect those who likely have dementia, we’ll need to make it more specific for that purpose, and carry out further research to validate its effectiveness.
We’ll be conducting more testing of the game soon. Anyone interested in giving it a go to help with our research can register on our team’s website.![]()
Joyce Siette, Research Theme Fellow in Health and Wellbeing, Western Sydney University and Paul Strutt, Senior Lecturer in Psychology, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Physical Sunscreen or Chemical Sunscreen – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing physical sunscreens to chemical sunscreens, we picked the physical sunscreens.
Why?
It’s easy to vote against chemical sunscreens, because it has “chemical” in the name, which tends to be offputting PR-wise no matter how healthy something is.
But in this case, there’s actual science here too!
Physical sunscreens physically block the UV rays.
- On the simplest of levels, mud is a physical sunscreen, as you can see widely used by elephants, hippos, pigs, and other animals.
- On a more sophisticated level, modern physical sunscreens often use tiny zinc particles (or similar) to block the UV rays in a way that isn’t so obvious to the naked eye—so we can still see our skin, and it looks just like we applied an oil or other moisturizer.
Chemical sunscreens interact with the UV rays in a way that absorbs them.
- Specifically, they usually convert it into relatively harmless thermal energy (heat)
- However, this can cause problems if there’s too much heat!
- Additionally, chemical sunscreens can get “used up” in a way that physical sunscreens can’t* becoming effectively deactivated once the chemical reaction has run its course and there is no more reagent left unreacted.
- Worse, some of the reagents, when broken down by the UV rays, can potentially cause harm when absorbed by the skin.
*That said, physical sunscreens will still need “topping up” because we are a living organism and our body can’t resist redistributing and using stuff—plus, depending on the climate and our activities, we can lose some externally too.
Further reading
We wrote about sunscreens (of various kinds) here:
And you can also read specifically about today’s topic in more detail, here:
What’s The Difference Between Physical And Chemical Sunscreens?
Take care!
Share This Post
-

Low-Dose Aspirin & Anemia
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We recently wrote about…
How To Survive A Heart Attack When You’re Alone
…and one of the items was “if you have aspirin readily available, then after calling an ambulance is the time to take it—but don’t exert yourself trying to find some”.
But what of aspirin as a preventative?
Many people take low-dose aspirin daily as a way to reduce the risk of atherothrombosis specifically (and thus, indirectly, they hope to reduce the risk of heart attacks).
The science of how helpful this is both clear and complicated—that is to say, the stats are not ambiguous*, but there are complicating factors of which many people are unaware.
*it will reduce the overall risk of cardiovascular events, but will not affect CVD mortality; in other words, it may improve your recovery from minor cardiac events, but is not likely to save you from major ones.
And also, it has unwanted side effects that can constitute a more relevant threat for many people. We’ll share more on that at the end of today’s article, but first…
A newly identified threat from daily aspirin use
A large (n=313,508) study of older adults (median age 73) were sorted into those who used low-dose aspirin as a preventative, and those who did not.
The primary outcome was incidence of anemia sufficient to require treatment, and the secondary outcome was major bleeding. And, at least 1 in 5 of those who experienced anemia also experienced bleeding.
The bleeding issue was not “newly identified” and will not surprise many people; after all, the very reason that aspirin is taken as a CVD preventative is for its anti-clotting property of allowing blood to flow more freely.
The anemia, however, has been getting increasing scientific scrutiny lately, after long going unnoticed in the wild. Given that anemia also gives the symptom “dizziness”, this is also a significant threat for increasing the incidence of falls in the older population, too, which can of course lead to serious complications and ultimately death.
Here’s the paper itself:
Want to know more?
As promised, here’s what we wrote previously about some of aspirin’s other risks:
Aspirin, CVD Risk, & Potential Counter-Risks
Take care!
Share This Post
-

25 Healthy Habits That Will Change Your Life
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cori Lefkowith, of “Redefining Strength” and “Strong At Every Age” fame, has compiled a list of the simple habits that make a big difference, and here they are!
The Tips
Her recommendations include…
- The healthy activities you’re most prone to skipping? Do those first
- Create staple meals… Consciously! This means: instead of getting into a rut of cooking the same few things in rotation because it’s what you have the ingredients in for, consciously and deliberately make a list of at least 7 meals that, between them, constitute a healthy balanced diet, and choose to make them your staples. That doesn’t mean don’t eat anything else (indeed, variety is good!) but having a robust collection of healthy staples to fall back on will help you avoid falling into unhealthy eating traps.
- Schedule time for healthy activities that you love. Instead of thinking “it would be nice to…”, actually figure out a timeslot, plan in advance, making it recurring, and do it!
- Have (healthy!) no-spoil food options always available. No-spoil doesn’t have to mean “won’t spoil ever”, but does mean at least that it has a long shelf-life. Nuts are a good example, assuming you’re not allergic. Sundried fruits are good too; not nearly as good as fresh fruit, but a lot better than some random processed snack because it’s what in. If you eat fish, then see if you can get dried fish in; it’s high in protein and keeps for a very long time indeed.
- Stock up on spices! Not only do they all have great health-giving properties (at least, we can’t think of a refutation by counterexample, Arrakis be damned), but also, they literally spice up our culinary repertoire, and bring joy to cooking and eating healthy food.
If you like these, check out the rest:
Click Here If The Embedded Video Doesn’t Load Automatically
Further reading
For more about actually making habits stick quickly and reliably,enjoy:
How To Really Pick Up (And Keep!) Those Habits
Take care!
Share This Post

-
Why do some young people use Xanax recreationally? What are the risks?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anecdotal reports from some professionals have prompted concerns about young people using prescription benzodiazepines such as Xanax for recreational use.
Border force detections of these drugs have almost doubled in the past five years, further fuelling the worry.
So why do young people use them, and how do the harms differ to those used as prescribed by a doctor?

Dragana Gordic/Shutterstock What are benzodiazepines?
You might know this large group of drugs by their trade names. Valium (diazepam), Xanax (alprazolam), Normison (temazepam) and Rohypnol (flunitrazepam) are just a few examples. Sometimes they’re referred to as minor tranquillisers or, colloquially, as “benzos”.
They increase the neurotransmitter gamma aminobutyric acid (GABA). GABA reduces activity in the brain, producing feelings of relaxation and sedation.
Unwanted side effects include drowsiness, dizziness and problems with coordination.
Benzodiazepines used to be widely prescribed for long-term management of anxiety and insomnia. They are still prescribed for these conditions, but less commonly, and are also sometimes used as part of the treatment for cancer, epilepsy and alcohol withdrawal.
Long-term use can lead to tolerance: when the effect wears off over time. So you need to use more over time to get the same effect. This can lead to dependence: when your body becomes reliant on the drug. There is a very high risk of dependence with these drugs.
When you stop taking benzodiazepines, you may experience withdrawal symptoms. For those who are dependent, the withdrawal can be long and difficult, lasting for several months or more.
So now they are only recommended for a few weeks at most for specific short-term conditions.
How do people get them? And how does it make them feel?
Benzodiazepines for non-medical use are typically either diverted from legitimate prescriptions or purchased from illicit drug markets including online.
Some illegally obtained benzodiazepines look like prescription medicines but are counterfeit pills that may contain fentanyl, nitazenes (both synthetic opioids) or other potent substances which can significantly increase the risk of accidental overdose and death.
When used recreationally, benzodiazepines are usually taken at higher doses than those typically prescribed, so there are even greater risks.
The effect young people are looking for in using these drugs is a feeling of profound relaxation, reduced inhibition, euphoria and a feeling of detachment from one’s surroundings. Others use them to enhance social experiences or manage the “comedown” from stimulant drugs like MDMA.
There are risks associated with using at these levels, including memory loss, impaired judgement, and risky behaviour, like unsafe sex or driving.
Some people report doing things they would not normally do when affected by high doses of benzodiazepines. There are cases of people committing crimes they can’t remember.
When taken at higher doses or combined with other depressant drugs such as alcohol or opioids, they can also cause respiratory depression, which prevents your lungs from getting enough oxygen. In extreme cases, it can lead to unconsciousness and even death.
Using a high dose also increases risk of tolerance and dependence.
Is recreational use growing?
The data we have about non-prescribed benzodiazepine use among young people is patchy and difficult to interpret.
The National Drug Strategy Household Survey 2022–23 estimates around 0.5% of 14 to 17 year olds and and 3% of 18 to 24 year olds have used a benzodiazepine for non medical purposes at least once in the past year.
The Australian Secondary Schools Survey 2022–23 reports that 11% of secondary school students they surveyed had used benzodiazepines in the past year. However they note this figure may include a sizeable proportion of students who have been prescribed benzodiazepines but have inadvertently reported using them recreationally.
In both surveys, use has remained fairly stable for the past two decades. So only a small percentage of young people have used benzodiazepines without a prescription and it doesn’t seem to be increasing significantly.
Reports of more young people using benzodiazepines recreationally might just reflect greater comfort among young people in talking about drugs and drug problems, which is a positive thing.
Prescribing of benzodiazepines to adolescents or young adults has also declined since 2012.
What can you do to reduce the risks?
To reduce the risk of problems, including dependence, benzodiazepines should be used for the shortest duration possible at the lowest effective dose.
Benzodiazepines should not be taken with other medicines without speaking to a doctor or pharmacist.
You should not drink alcohol or take illicit drugs at the same time as using benzodiazepines.
Benzodiazepines shouldn’t be taken with other medicines, without the go-ahead from your doctor or pharmacist. Cloudy Design/Shutterstock Counterfeit benzodiazepines are increasingly being detected in the community. They are more dangerous than pharmaceutical benzodiazepines because there is no quality control and they may contain unexpected and dangerous substances.
Drug checking services can help people identify what is in substances they intend to take. It also gives them an opportunity to speak to a health professional before they use. People often discard their drugs after they find out what they contain and speak to someone about drug harms.
If people are using benzodiazepines without a prescription to self manage stress, anxiety or insomnia, this may indicate a more serious underlying condition. Psychological therapies such as cognitive behaviour therapy, including mindfulness-based approaches, are very effective in addressing these symptoms and are more effective long term solutions.
Lifestyle modifications – such as improving exercise, diet and sleep – can also be helpful.
There are also other medications with a much lower risk of dependence that can be used to treat anxiety and insomnia.
If you or someone you know needs help with benzodiazepine use, Reconnexions can help. It’s a counselling and support service for people who use benzodiazepines.
Alternatively, CounsellingOnline is a good place to get information and referral for treatment of benzodiazepine dependence. Or speak to your GP. The Sleep Health Foundation has some great resources if you are having trouble with sleep.
Nicole Lee, Adjunct Professor at the National Drug Research Institute (Melbourne based), Curtin University and Suzanne Nielsen, Professor and Deputy Director, Monash Addiction Research Centre, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between miscarriage and stillbirth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Former US First Lady Michelle Obama revealed in her memoir she had a miscarriage. UK singer-songwriter and actor Lily Allen has gone on the record about her stillbirth.
Both miscarriage and stillbirth are sadly familiar terms for pregnancy loss. They can be traumatic life events for the prospective parents and family, and their impacts can be long-lasting. But the terms can be confused.
Here are some similarities and differences between miscarriage and stillbirth, and why they matter.
christinarosepix/Shutterstock Let’s start with some definitions
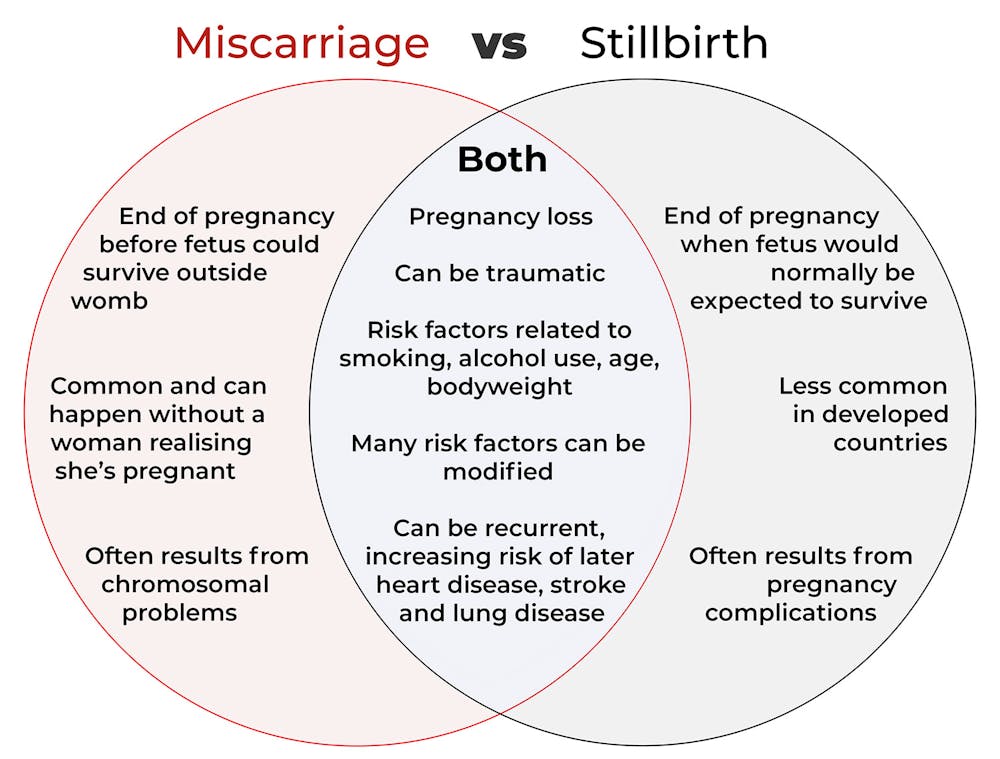
In broad terms, a miscarriage is when a pregnancy ends while the fetus is not yet viable (before it could survive outside the womb).
This is the loss of an “intra-uterine” pregnancy, when an embryo is implanted in the womb to then develop into a fetus. The term miscarriage excludes ectopic pregnancies, where the embryo is implanted outside the womb.
However, stillbirth refers to the end of a pregnancy when the fetus is normally viable. There may have been sufficient time into the pregnancy. Alternatively, the fetus may have grown large enough to be normally expected to survive, but it dies in the womb or during delivery.
The Australian Institute of Health and Welfare defines stillbirth as a fetal death of at least 20 completed weeks of gestation or with a birthweight of at least 400 grams.
Internationally, definitions of stillbirth vary depending on the jurisdiction.
How common are they?
It is difficult to know how common miscarriages are as they can happen when a woman doesn’t know she is pregnant. There may be no obvious symptoms or something that looks like a heavier-than-normal period. So miscarriages are likely to be more common than reported.
Studies from Europe and North America suggest a miscarriage occurs in about one in seven pregnancies (15%). More than one in eight women (13%) will have a miscarriage at some time in her life.
Around 1–2% of women have recurrent miscarriages. In Australia this is when someone has three or more miscarriages with no pregnancy in between.
Australia has one of the lowest rates of stillbirth in the world. The rate has been relatively steady over the past 20 years at 0.7% or around seven per 1,000 pregnancies.
Who’s at risk?
Someone who has already had a miscarriage or stillbirth has an increased risk of that outcome again in a subsequent pregnancy.
Compared with women who have had a live birth, those who have had a stillbirth have double the risk of another. For those who have had recurrent miscarriages, the risk of another miscarriage is four-fold higher.
Some factors have a u-shaped relationship, with the risk of miscarriage and stillbirth lowest in the middle.
For instance, maternal age is a risk factor for both miscarriage and stillbirth, especially if under 20 years old or older than 35. Increasing age of the male is only a risk factor for stillbirth, especially for fathers over 40.
An older dad can be a risk factor for stillbirth, but not miscarriage. Elizaveta Galitckaia/Shutterstock Similarly for maternal bodyweight, women with a body mass index or BMI in the normal range have the lowest risk of miscarriage and stillbirth compared with those in the obese or underweight categories.
Lifestyle factors such as smoking and heavy alcohol drinking while pregnant are also risk factors for both miscarriage and stillbirth.
So it’s important to not only avoid smoking and alcohol while pregnant, but before getting pregnant. This is because early in the pregnancy, women may not know they have conceived and could unwittingly expose the developing fetus.
Why do they happen?
Miscarriage often results from chromosomal problems in the developing fetus. However, genetic conditions or birth defects account for only 7-14% of stillbirths.
Instead, stillbirths often relate directly to pregnancy complications, such as a prolonged pregnancy or problems with the umbilical cord.
Maternal health at the time of pregnancy is another contributing factor in the risk of both miscarriage and stillbirths.
Chronic diseases, such as high blood pressure, diabetes, hypothyroidism (underactive thyroid), polycystic ovary syndrome, problems with the immune system (such as an autoimmune disorder), and some bacterial and viral infections are among factors that can increase the risk of miscarriage.
Similarly mothers with diabetes, high blood pressure, and untreated infections, such as malaria or syphilis, face an increased risk of stillbirth.
In many cases, however, the specific cause of pregnancy loss is not known.
How about the long-term health risks?
Miscarriage and stillbirth can be early indicators of health issues later in life.
For instance, women who have had recurrent miscarriages or recurrent stillbirths are at higher risk of cardiovascular disease (such as heart disease or stroke).
Our research has also looked at the increased risk of stroke. Compared with women who had never miscarried, we found women with a history of three or more miscarriages had a 35% higher risk of non-fatal stroke and 82% higher risk of fatal stroke.
Women who had a stillbirth had a 31% higher risk of a non-fatal stroke, and those who had had two or more stillbirths were at a 26% higher risk of a fatal stroke.
We saw similar patterns in chronic obstructive pulmonary disease or COPD, a progressive lung disease with respiratory symptoms such as breathlessness and coughing.
Our data showed women with a history of recurrent miscarriages or stillbirths were at a 36% or 67% higher risk of COPD, respectively, even after accounting for a history of asthma.
Long-term health risks of recurrent miscarriages or stillbirths include developing lung disease later in life. PRPicturesProduction/Shutterstock Why is all this important?
Being well-informed about the similarities and differences between these two traumatic life events may help explain what has happened to you or a loved one.
Where risk factors can be modified, such as smoking and obesity, this information can be empowering for individuals who wish to reduce their risk of miscarriage and stillbirth and make lifestyle changes before they become pregnant.
More information and support about miscarriage and stillbirth is available from SANDS and Pink Elephants.
Gita Mishra, Professor of Life Course Epidemiology, Faculty of Medicine, The University of Queensland; Chen Liang, PhD student, reproductive history and non-communicable diseases in women, The University of Queensland, and Jenny Doust, Clinical Professorial Research Fellow, School of Public Health, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Build Muscle (Healthily!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What Do You Have To Gain?
We have previously promised a three-part series about changing one’s weight:
- Losing weight (specifically, losing fat)
- Gaining weight (specifically, gaining muscle)
- Gaining weight (specifically, gaining fat)
And yes, that last one is also something that some people want/need to do (healthily!), and want/need help with that.
There will be, however, no need for a “losing muscle” article, because (even though sometimes a person might have some reason to want to do this), it’s really just a case of “those things we said for gaining muscle? Don’t do those and the muscle will atrophy naturally”.
Here’s the first part: How To Lose Weight (Healthily!)
While some people will want to lose fat, please do be aware that the association between weight loss and good health is not nearly so strong as the weight loss industry would have you believe:
And, while BMI is not a useful measure of health in general, it’s worth noting that over the age of 65, a BMI of 27 (which is in the high end of “overweight”, without being obese) is associated with the lowest all-cause mortality:
BMI and all-cause mortality in older adults: a meta-analysis
Body weight, muscle mass, and protein:
That BMI of 27, or whatever weight you might wish to be, ignores body composition. You’re probably aware that volume-for-volume, muscle weighs more than fat.
You’re also probably aware that if we’re not careful, we tend to lose muscle as we get older. This is known as age-related sarcopenia:
Protein, & Fighting Sarcopenia
Dr. Gabrielle Lyon, our featured expert in the above article, recommends getting at least 1.6g of protein per kg of body weight per day (Americans, divide your weight in pounds by 2.2 to get your weight in kg).
So for example, if you weigh 165lb, that’s 75kg, that’s 1.6×75=120g of protein per day.
There is an upper limit to how much protein per day is healthy, and that limit is probably around 2g of protein per kg of body weight per day:
Protein: How Much Do We Need, Really?
You may be wondering: should we go for animal or plant protein? In which case, the short version is:
- If you only care about muscle growth, any complete sources of protein are fine
- If you care about your general health too, then avoiding red meat is best, but other common protein sources are all fine
- Unprocessed is (unsurprisingly) better than processed in either case
Longer version: Plant vs Animal Protein: Head to Head
What exercises are best for muscle-building?
Of course, different muscles require different exercises, but for all of them, resistance training is what builds muscle the most, and it’s pretty much impossible to build a lot of muscle otherwise.
Check out: Resistance Is Useful! (Especially As We Get Older)
Prepare to fail!
No, really, prepare to fail. Because while resistance training in general is good for maintaining strong muscles and bones, you will only gain muscle if your current muscle is not enough to do the exercise:
- If you do a heavy resistance exercise without undue difficulty, your muscles will say to each other “Good job, team! That was hard, but luckily we were strong enough; no changes necessary”.
- If you do a heavy resistance exercise to the point where you can no longer do it (called: training to failure), then your muscles will say to each other “Oof, what a task! What we’ve got here is clearly not enough, so we’ll have to add more muscle for next time”.
Safety note: training to failure comes with safety risks. If using free weights or weight machines, please do so under well-trained supervision. If doing it with bodyweight (e.g. press-ups until you can press no more) or resistance bands, please check with your doctor first to ensure this is safe for you.
You can also increase the effectiveness of your resistance training by doing it in a way that “confuses” your muscles, making it harder for them to adapt in the moment, and thus forcing them to adapt more in the long term (e.g. get bigger and stronger):
HIIT, But Make It HIRT: High Intensity Resistance Training
Make time for recovery
While many kinds of exercise can be done daily, exercise to build muscle(s) means at the very least resting that muscle (or muscle group) the next day.
For this reason, a lot of bodybuilders have for example a week’s schedule that might look like:
- Monday: Upper body training
- Wednesday: Lower body training
- Friday: Core strength training
…and rest on other days. This gives most muscles a full week of recovery, and every muscle at least 48 hours of recovery.
Note: bodybuilders, like children (who are also doing a lot of body-building, in their own way) need more sleep in order to allow for this recovery and growth to occur. Serious bodybuilders often aim for 12 hours sleep per day. This might be impractical, undesirable, or even impossible for some people, but it’s a factor to be borne in mind and not forgotten.
See also:
Overdone It? How To Speed Up Recovery After Exercise (According To Actual Science)
Anything else that can (safely and healthily) be done to promote muscle growth?
There are a lot of supplements on the market; some are healthy and helpful, other not so much. Here are some we’ve written about:
- What To Eat, Take, And Do Before A Workout
- Creatine: Very Different For Young & Old People
- Ginseng: Exercising With Less Soreness!
- Taurine’s Benefits For Heart Health And More
- Topping Up Testosterone? What To Consider
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: