Some women’s breasts can’t make enough milk, and the effects can be devastating
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many new mothers worry about their milk supply. For some, support from a breastfeeding counsellor or lactation consultant helps.
Others cannot make enough milk no matter how hard they try. These are women whose breasts are not physically capable of producing enough milk.
Our recently published research gives us clues about breast features that might make it difficult for some women to produce enough milk. Another of our studies shows the devastating consequences for women who dream of breastfeeding but find they cannot.
Some breasts just don’t develop
Unlike other organs, breasts are not fully developed at birth. There are key developmental stages as an embryo, then again during puberty and pregnancy.
At birth, the breast consists of a simple network of ducts. Usually during puberty, the glandular (milk-making) tissue part of the breast begins to develop and the ductal network expands. Then typically, further growth of the ductal network and glandular tissue during pregnancy prepares the breast for lactation.
But our online survey of women who report low milk supply gives us clues to anomalies in how some women’s breasts develop.
We’re not talking about women with small breasts, but women whose glandular tissue (shown in this diagram as “lobules”) is underdeveloped and have a condition called breast hypoplasia.
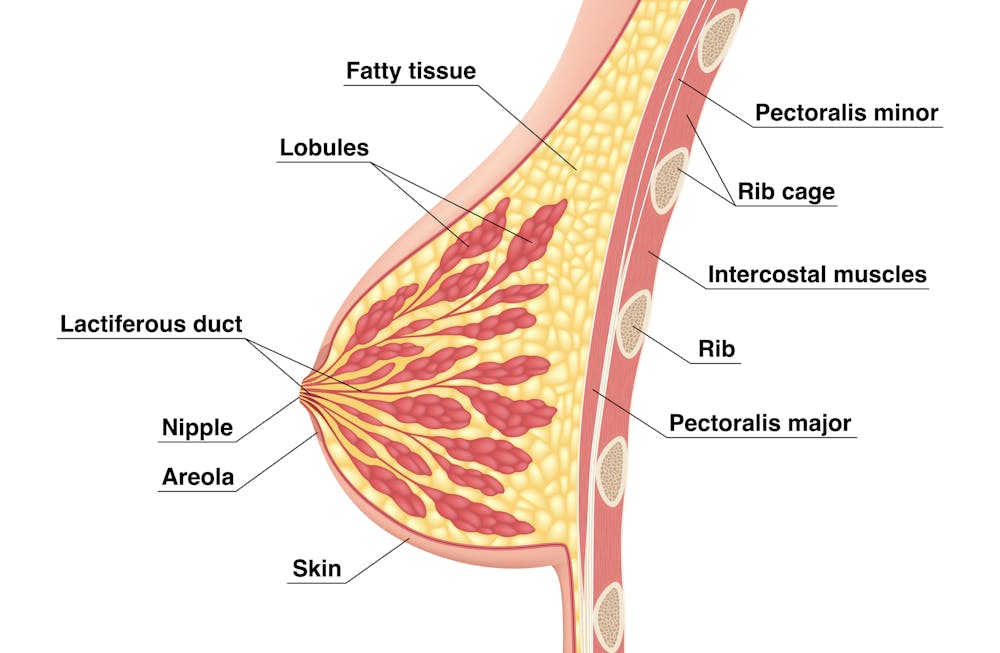
Tsuyna/Shutterstock
We don’t know how common this is. But it has been linked with lower rates of exclusive breastfeeding.
We also don’t know what causes it, with much of the research conducted in animals and not humans.
However, certain health conditions have been associated with it, including polycystic ovary syndrome and other endocrine (hormonal) conditions. A high body-mass index around the time of puberty may be another indicator.
Could I have breast hypoplasia?
Our survey and other research give clues about who may have breast hypoplasia.
But it’s important to note these characteristics are indicators and do not mean women exhibiting them will definitely be unable to exclusively breastfeed.
Indicators include:
- a wider than usual gap between the breasts
- tubular-shaped (rather than round) breasts
- asymmetric breasts (where the breasts are different sizes or shapes)
- lack of breast growth in pregnancy
- a delay in or absence of breast fullness in the days after giving birth
In our survey, 72% of women with low milk supply had breasts that did not change appearance during pregnancy, and about 70% reported at least one irregular-shaped breast.
The effects
Mothers with low milk supply – whether or not they have breast hyoplasia or some other condition that limits their ability to produce enough milk – report a range of emotions.
Research, including our own, shows this ranges from frustration, confusion and surprise to intense or profound feelings of failure, guilt, grief and despair.
Some mothers describe “breastfeeding grief” – a prolonged sense of loss or failure, due to being unable to connect with and nourish their baby through breastfeeding in the way they had hoped.
These feelings of failure, guilt, grief and despair can trigger symptoms of anxiety and depression for some women.

Bricolage/Shutterstock
One woman told us:
[I became] so angry and upset with my body for not being able to produce enough milk.
Many women’s emotions intensified when they discovered that despite all their hard work, they were still unable to breastfeed their babies as planned. A few women described reaching their “breaking point”, and their experience felt “like death”, “the worst day of [my] life” or “hell”.
One participant told us:
I finally learned that ‘all women make enough milk’ was a lie. No amount of education or determination would make my breasts work. I felt deceived and let down by all my medical providers. How dare they have no answers for me when I desperately just wanted to feed my child naturally.
Others told us how they learned to accept their situation. Some women said they were relieved their infant was “finally satisfied” when they began supplementing with formula. One resolved to:
prioritise time with [my] baby over pumping for such little amounts.
Where to go for help
If you are struggling with low milk supply, it can help to see a lactation consultant for support and to determine the possible cause.
This will involve helping you try different strategies, such as optimising positioning and attachment during breastfeeding, or breastfeeding/expressing more frequently. You may need to consider taking a medication, such as domperidone, to see if your supply increases.
If these strategies do not help, there may be an underlying reason why you can’t make enough milk, such as insufficient glandular tissue (a confirmed inability to make a full supply due to breast hypoplasia).
Even if you have breast hypoplasia, you can still breastfeed by giving your baby extra milk (donor milk or formula) via a bottle or using a supplementer (which involves delivering milk at the breast via a tube linked to a bottle).
More resources
The following websites offer further information and support:
- Australian Breastfeeding Association
- Lactation Consultants of Australia and New Zealand
- Royal Women’s Hospital, Melbourne
- Supply Line Breastfeeders Support Group of Australia Facebook support group
- IGT And Low Milk Supply Support Group Facebook support group
- Breastfeeding Medicine Network Australia/New Zealand
- Supporting breastfeeding grief (a collection of resources).
Shannon Bennetts, a research fellow at La Trobe University, contributed to this article.![]()
Renee Kam, PhD candidate and research officer, La Trobe University and Lisa Amir, Professor in Breastfeeding Research, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Clean – by Dr. James Hamblin

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our skin is our largest organ, and it’s easy to forget that, and how much it does for us. All things considered, it’s good to take good care of it! But what if we sometimes take too much “care” of it?
Dr. James Hamblin, a medical doctor-turned-writer, has explored this a lot both personally and in research. Through such, he has come to the conclusion there’s definitely a “sweet spot” of personal hygiene:
- Too little, and the Bubonic plague sweeps through Europe, or other plagues sweep through other places when European invaders came.
- Too much, and we strip our skin of one of its greatest qualities: the ability to protect us.
Dr. Hamblin asks (and answers) such questions as:
- What is good hygiene, and what is neurotically doing ourselves multiple levels of harm because advertising companies shamed us into doing so?
- Is it good or bad to use a series of products, each to undo the problem caused by the previous?
- What the difference between a 5-step skincare routine, and a series of gratuitous iatrogenic damage?
- Which products clean us most helpfully, and which clean us most harmfully?
- How often should we bathe/shower, really?
If the book has a weak point, it’s that it’s written mostly with his body in mind. That makes a difference when it comes to hairwashing, for example. He’s a white guy with short hair. If you’re black and/or have long hair, for example, your haircare needs will be quite different. Similarly, many women engage in shaving/depilation in places that most men don’t, and the consequences of that choice (and implications for any extra washing needs/harms) aren’t covered.
Bottom line: notwithstanding the aforementioned blind-spots, this book will help readers reduce the amount of harm we are doing to our bodies with our washing routines, without sacrificing actual hygiene.
Click here to check out Clean and help your skin to help you!
Share This Post
-

To tackle gendered violence, we also need to look at drugs, trauma and mental health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
After several highly publicised alleged murders of women in Australia, the Albanese government this week pledged more than A$925 million over five years to address men’s violence towards women. This includes up to $5,000 to support those escaping violent relationships.
However, to reduce and prevent gender-based and intimate partner violence we also need to address the root causes and contributors. These include alcohol and other drugs, trauma and mental health issues.
Why is this crucial?
The World Health Organization estimates 30% of women globally have experienced intimate partner violence, gender-based violence or both. In Australia, 27% of women have experienced intimate partner violence by a co-habiting partner; almost 40% of Australian children are exposed to domestic violence.
By gender-based violence we mean violence or intentionally harmful behaviour directed at someone due to their gender. But intimate partner violence specifically refers to violence and abuse occurring between current (or former) romantic partners. Domestic violence can extend beyond intimate partners, to include other family members.
These statistics highlight the urgent need to address not just the aftermath of such violence, but also its roots, including the experiences and behaviours of perpetrators.
What’s the link with mental health, trauma and drugs?
The relationships between mental illness, drug use, traumatic experiences and violence are complex.
When we look specifically at the link between mental illness and violence, most people with mental illness will not become violent. But there is evidence people with serious mental illness can be more likely to become violent.
The use of alcohol and other drugs also increases the risk of domestic violence, including intimate partner violence.
About one in three intimate partner violence incidents involve alcohol. These are more likely to result in physical injury and hospitalisation. The risk of perpetrating violence is even higher for people with mental ill health who are also using alcohol or other drugs.
It’s also important to consider traumatic experiences. Most people who experience trauma do not commit violent acts, but there are high rates of trauma among people who become violent.
For example, experiences of childhood trauma (such as witnessing physical abuse) can increase the risk of perpetrating domestic violence as an adult.

Childhood trauma can leave its mark on adults years later. Roman Yanushevsky/Shutterstock Early traumatic experiences can affect the brain and body’s stress response, leading to heightened fear and perception of threat, and difficulty regulating emotions. This can result in aggressive responses when faced with conflict or stress.
This response to stress increases the risk of alcohol and drug problems, developing PTSD (post-traumatic stress disorder), and increases the risk of perpetrating intimate partner violence.
How can we address these overlapping issues?
We can reduce intimate partner violence by addressing these overlapping issues and tackling the root causes and contributors.
The early intervention and treatment of mental illness, trauma (including PTSD), and alcohol and other drug use, could help reduce violence. So extra investment for these are needed. We also need more investment to prevent mental health issues, and preventing alcohol and drug use disorders from developing in the first place.
Early intervention and treatment of mental illness, trauma and drug use is important. Okrasiuk/Shutterstock Preventing trauma from occuring and supporting those exposed is crucial to end what can often become a vicious cycle of intergenerational trauma and violence. Safe and supportive environments and relationships can protect children against mental health problems or further violence as they grow up and engage in their own intimate relationships.
We also need to acknowledge the widespread impact of trauma and its effects on mental health, drug use and violence. This needs to be integrated into policies and practices to reduce re-traumatising individuals.
How about programs for perpetrators?
Most existing standard intervention programs for perpetrators do not consider the links between trauma, mental health and perpetrating intimate partner violence. Such programs tend to have little or mixed effects on the behaviour of perpetrators.
But we could improve these programs with a coordinated approach including treating mental illness, drug use and trauma at the same time.
Such “multicomponent” programs show promise in meaningfully reducing violent behaviour. However, we need more rigorous and large-scale evaluations of how well they work.
What needs to happen next?
Supporting victim-survivors and improving interventions for perpetrators are both needed. However, intervening once violence has occurred is arguably too late.
We need to direct our efforts towards broader, holistic approaches to prevent and reduce intimate partner violence, including addressing the underlying contributors to violence we’ve outlined.
We also need to look more widely at preventing intimate partner violence and gendered violence.
We need developmentally appropriate education and skills-based programs for adolescents to prevent the emergence of unhealthy relationship patterns before they become established.
We also need to address the social determinants of health that contribute to violence. This includes improving access to affordable housing, employment opportunities and accessible health-care support and treatment options.
All these will be critical if we are to break the cycle of intimate partner violence and improve outcomes for victim-survivors.
The National Sexual Assault, Family and Domestic Violence Counselling Line – 1800 RESPECT (1800 737 732) – is available 24 hours a day, seven days a week for any Australian who has experienced, or is at risk of, family and domestic violence and/or sexual assault.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14. In an emergency, call 000.
Siobhan O’Dean, Postdoctoral Research Associate, The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney; Lucinda Grummitt, Postdoctoral Research Fellow, The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney, and Steph Kershaw, Research Fellow, The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Here’s Looking At Ya!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This Main Feature Should Take You Two Minutes (and 18 Seconds) To Read*
*Or at least, that’s what we’re told by this software that checks things for readability!
There’s a problem nobody wants to talk about when it comes to speed-reading
If you’re not very conscientious in your method, information does get lost. Especially, anything over 500 words per minute is almost certainly skimming and not true speed-reading.
One of the reasons information gets lost is because of a weird and wonderful feature of our eyes and brain: saccades.
Basically, our eyes can either collect visual information or they can move; they can’t do both at once. And as you may know, our eyes are almost always moving. So why aren’t we blind most of the time?
We actually are.
Did you know: your eyes take two upside-down 2D images and your brain presents you one 3D image the right way around instead? You probably did know that. So: it’s a bit like that.
Your brain takes a series of snapshots from whenever your eyes weren’t moving, and mentally fills in the blanks for you, just like a studio animation. We have a “frame rate” of about 60 frames per second, by the way—that’s why many computer monitors use that frequency. Lower frequencies can result in a noticeable flicker, and higher frequencies are wasted on us mere mortals!
Our eyes do some super-speedy movements called saccades (up to 500º per second! Happily no, our eyes don’t rotate 500º, but that’s the “per second” rate) and our brain fills in the gaps with its best guesses. The more you push it, the more it’ll guess wrong.
We’re not making this up, by the way! See for yourself:
Eye Movements In Reading And Information Processing: 20 Years Of Research
Fortunately, it is possible to use your eyes in a way that reduces the brain’s need to guess. That also means it has more processing power left over to guess correctly when it does need to.
Yes, There’s An App For That
Actually there are a few! But we’re going to recommend Spreeder as a top-tier option, with very rapid improvement right from day one.
It works by presenting the text with a single unmoving focal point. This is the opposite of traditional speed-reading methods that involve a rapidly moving pacer (such as your finger on the page, or a dot on the screen).
This unmoving focal point (while the words move instead) greatly reduces the number of saccades needed, and so a lot less information is lost to optical illusions and guesswork.
Try Spreeder (any platform) Here Now!
If you find that easy to use and would like something with a few more features, you might like another app that works on the same principle: Spritz.
It can take a bit more getting-used-to, but allows for greater integrations with all your favourite content in the long-run:
Check Out Spritz: Android App / iOS App / Free Chrome Extension
Lastly, if you don’t want any of those fancy apps and would just like to read more quickly and easily with less eye-strain, Beeline has you covered.
For free, unless you want to unlock some premium features!
How Beeline works is by adding a color gradient to text on websites and in documents. This makes it a lot easier for the eye to track without going off-piste, skipping a line, or re-reading the same bit again, etc.
Share This Post


Related Posts
-

The Cancer Journey – by Dr. Chadi Nabhan
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
After a brief introduction of what cancer actually is and what causes it, the layout of the rest of the book is in chronological order of patient experience, that is to say, what to expect during the journey from screening and diagnosis, to one’s first oncology visit (the author being an oncologist himself), how cancer staging works, getting second opinions, and a chapter-by-chapter review of many different treatment options, ranging from surgery and chemotherapy, to radiation and hormonal therapies, and even more modern targeted therapies, immunotherapy, cellular therapies, and yes, complementary and alternative therapies, amongst others we haven’t listed for the sake of brevity.
He doesn’t leave it there though; he also talks managing side effects, monitoring for recurrence, and even caring for the caregiver(s), along with eventual survivorship and that emotional journey, or if it comes down to it, palliative and hospice care.
Finishing on a hopeful note, he also brings attention to novel approaches that are being trialled presently, and the prospects for the near future of cancer care.
The style is very human and readable, notwithstanding that the author has hundreds of peer-reviewed publications to his name, the content here is presented in a much more approachable, less clinical way, while still conveying all the information that needs to be conveyed.
Bottom line: if you or a loved one is facing cancer, this book will be an invaluable resource.
Click here to check out The Cancer Journey, and understand each part of it!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Migraine Mythbusting
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine: When Headaches Are The Tip Of The Neurological Iceberg

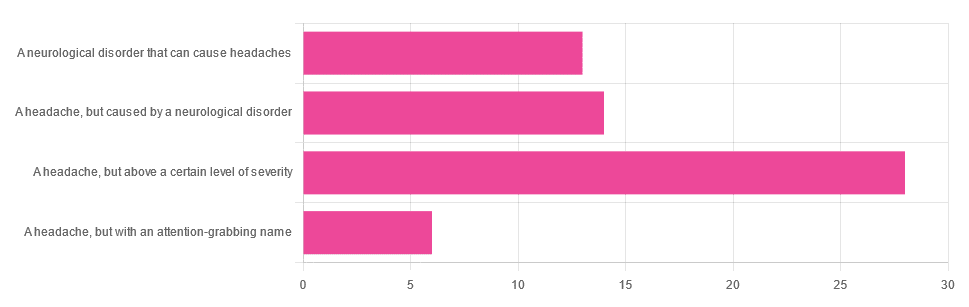
Yesterday, we asked you “What is a migraine?” and got the above-depicted, below-described spread of responses:
- Just under 46% said “a headache, but above a certain level of severity”
- Just under 23% said “a headache, but caused by a neurological disorder”
- Just over 21% said “a neurological disorder that can cause headaches”
- Just under 10% said “a headache, but with an attention-grabbing name”
So… What does the science say?
A migraine is a headache, but above a certain level of severity: True or False?
While that’s usually a very noticeable part of it… That’s only one part of it, and not a required diagnostic criterion. So, in terms of defining what a migraine is, False.
Indeed, migraine may occur without any headache, let alone a severe one, for example: Abdominal Migraine—though this is much less well-researched than the more common with-headache varieties.
Here are the defining characteristics of a migraine, with the handy mnemonic 5-4-3-2-1:
- 5 or more attacks
- 4 hours to 3 days in duration
- 2 or more of the following:
- Unilateral (affects only one side of the head)
- Pulsating
- Moderate or severe pain intensity
- Worsened by or causing avoidance of routine physical activity
- 1 or more of the following:
- Nausea and/or vomiting
- Sensitivity to both light and sound
Source: Cephalalgia | ICHD-II Classification: Parts 1–3: Primary, Secondary and Other
As one of our subscribers wrote:
❝I have chronic migraine, and it is NOT fun. It takes away from my enjoyment of family activities, time with friends, and even enjoying alone time. Anyone who says a migraine is just a bad headache has not had to deal with vertigo, nausea, loss of balance, photophobia, light sensitivity, or a host of other symptoms.❞
Migraine is a neurological disorder: True or False?
True! While the underlying causes aren’t known, what is known is that there are genetic and neurological factors at play.
❝Migraine is a recurrent, disabling neurological disorder. The World Health Organization ranks migraine as the most prevalent, disabling, long-term neurological condition when taking into account years lost due to disability.
Considerable progress has been made in elucidating the pathophysiological mechanisms of migraine, associated genetic factors that may influence susceptibility to the disease❞
Source: JHP | Mechanisms of migraine as a chronic evolutive condition
Migraine is just a headache with a more attention-grabbing name: True or False?
Clearly, False.
As we’ve already covered why above, we’ll just close today with a nod to an old joke amongst people with chronic illnesses in general:
“Are you just saying that because you want attention?”
“Yes… Medical attention!”
Want to learn more?
You can find a lot of resources at…
NIH | National Institute of Neurological Disorders & Stroke | Migraine
and…
The Migraine Trust ← helpfully, this one has a “Calm mode” to tone down the colorscheme of the website!
Particularly useful from the above site are its pages:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Insomnia Decoded – by Dr. Audrey Porter
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve written about sleep books before, so what makes this one different? Its major selling point is: most of the focus isn’t on the things that everyone already knows.
Yes, there’s a section on sleep hygiene and yes it’ll tell you to cut the caffeine and alcohol, but most of the advice here is beyond that.
Rather, it looks at finding out (if you don’t already know for sure) what is keeping you from healthy sleep, be it environmental, directly physical, or psychological, and breaking out of the stress-sleep cycle that often emerges from such.
The style is light and conversational, but includes plenty of science too; Dr. Porter knows her stuff.
Bottom line: if you feel like you know what you should be doing, but somehow life keeps conspiring to stop you from doing it, then this is the book that could help you break out that cycle.
Click here to check out Insomnia Decoded, and get regular healthy sleep!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: