5 Exercises You’ll Regret Ignoring In 10 Years!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Later, you’ll wish you’d started sooner. So, today’s a great day to learn these exercises and get the ball rolling:
Use It Or Lose It
The “alive five”:
- Handstands and wall variations: not about looking cool, but rather about building shoulder mobility, core engagement, wrist strength, and body awareness under pressure; teaches control, fear management, and structural alignment starting from the ground up.
- Crawling patterns, ground flow, and squat transitions: retrains coordination, rhythm, and spatial awareness by reconnecting the brain to the body; essential for core integration, joint cooperation, and real-world strength like standing up from the floor without hands.
- Single leg balance and other unilateral strength work: critical for injury prevention and joint stability; develops foot, knee, and hip control while revealing imbalances and improving strength on each side of the body independently.
- Dynamic backbends and spinal extension: counters modern posture issues by reopening the spine and chest; important for breathing, posture, spinal decompression, and reclaiming mobility lost through years of sitting and slouching.
- Rolling patterns and spinal reset: teaches the body to move with grace, not tension; helps the spine move fluidly, reconnects breath with movement, and restores nervous system softness and control.
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Mobility For Now & For Later: Train For The Marathon That Is Your Life!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Older Americans Say They Feel Trapped in Medicare Advantage Plans

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In 2016, Richard Timmins went to a free informational seminar to learn more about Medicare coverage.
“I listened to the insurance agent and, basically, he really promoted Medicare Advantage,” Timmins said. The agent described less expensive and broader coverage offered by the plans, which are funded largely by the government but administered by private insurance companies.
For Timmins, who is now 76, it made economic sense then to sign up. And his decision was great, for a while.
Then, three years ago, he noticed a lesion on his right earlobe.
“I have a family history of melanoma. And so, I was kind of tuned in to that and thinking about that,” Timmins said of the growth, which doctors later diagnosed as malignant melanoma. “It started to grow and started to become rather painful.”
Timmins, though, discovered that his enrollment in a Premera Blue Cross Medicare Advantage plan would mean a limited network of doctors and the potential need for preapproval, or prior authorization, from the insurer before getting care. The experience, he said, made getting care more difficult, and now he wants to switch back to traditional, government-administered Medicare.
But he can’t. And he’s not alone.
“I have very little control over my actual medical care,” he said, adding that he now advises friends not to sign up for the private plans. “I think that people are not understanding what Medicare Advantage is all about.”
Enrollment in Medicare Advantage plans has grown substantially in the past few decades, enticing more than half of all eligible people, primarily those 65 or older, with low premium costs and perks like dental and vision insurance. And as the private plans’ share of the Medicare patient pie has ballooned to 30.8 million people, so too have concerns about the insurers’ aggressive sales tactics and misleading coverage claims.
Enrollees, like Timmins, who sign on when they are healthy can find themselves trapped as they grow older and sicker.
“It’s one of those things that people might like them on the front end because of their low to zero premiums and if they are getting a couple of these extra benefits — the vision, dental, that kind of thing,” said Christine Huberty, a lead benefit specialist supervising attorney for the Greater Wisconsin Agency on Aging Resources.
“But it’s when they actually need to use it for these bigger issues,” Huberty said, “that’s when people realize, ‘Oh no, this isn’t going to help me at all.’”
Medicare pays private insurers a fixed amount per Medicare Advantage enrollee and in many cases also pays out bonuses, which the insurers can use to provide supplemental benefits. Huberty said those extra benefits work as an incentive to “get people to join the plan” but that the plans then “restrict the access to so many services and coverage for the bigger stuff.”
David Meyers, assistant professor of health services, policy, and practice at the Brown University School of Public Health, analyzed a decade of Medicare Advantage enrollment and found that about 50% of beneficiaries — rural and urban — left their contract by the end of five years. Most of those enrollees switched to another Medicare Advantage plan rather than traditional Medicare.
In the study, Meyers and his co-authors muse that switching plans could be a positive sign of a free marketplace but that it could also signal “unmeasured discontent” with Medicare Advantage.
“The problem is that once you get into Medicare Advantage, if you have a couple of chronic conditions and you want to leave Medicare Advantage, even if Medicare Advantage isn’t meeting your needs, you might not have any ability to switch back to traditional Medicare,” Meyers said.
Traditional Medicare can be too expensive for beneficiaries switching back from Medicare Advantage, he said. In traditional Medicare, enrollees pay a monthly premium and, after reaching a deductible, in most cases are expected to pay 20% of the cost of each nonhospital service or item they use. And there is no limit on how much an enrollee may have to pay as part of that 20% coinsurance if they end up using a lot of care, Meyers said.
To limit what they spend out-of-pocket, traditional Medicare enrollees typically sign up for supplemental insurance, such as employer coverage or a private Medigap policy. If they are low-income, Medicaid may provide that supplemental coverage.
But, Meyers said, there’s a catch: While beneficiaries who enrolled first in traditional Medicare are guaranteed to qualify for a Medigap policy without pricing based on their medical history, Medigap insurers can deny coverage to beneficiaries transferring from Medicare Advantage plans or base their prices on medical underwriting.
Only four states — Connecticut, Maine, Massachusetts, and New York — prohibit insurers from denying a Medigap policy if the enrollee has preexisting conditions such as diabetes or heart disease.
Paul Ginsburg is a former commissioner on the Medicare Payment Advisory Commission, also known as MedPAC. It’s a legislative branch agency that advises Congress on the Medicare program. He said the inability of enrollees to easily switch between Medicare Advantage and traditional Medicare during open enrollment periods is “a real concern in our system; it shouldn’t be that way.”
The federal government offers specific enrollment periods every year for switching plans. During Medicare’s open enrollment period, from Oct. 15 to Dec. 7, enrollees can switch out of their private plans to traditional, government-administered Medicare.
Medicare Advantage enrollees can also switch plans or transfer to traditional Medicare during another open enrollment period, from Jan. 1 to March 31.
“There are a lot of people that say, ‘Hey, I’d love to come back, but I can’t get Medigap anymore, or I’ll have to just pay a lot more,’” said Ginsburg, who is now a professor of health policy at the University of Southern California.
Timmins is one of those people. The retired veterinarian lives in a rural community on Whidbey Island just north of Seattle. It’s a rugged, idyllic landscape and a popular place for second homes, hiking, and the arts. But it’s also a bit remote.
While it’s typically harder to find doctors in rural areas, Timmins said he believes his Premera Blue Cross plan made it more challenging to get care for a variety of reasons, including the difficulty of finding and getting in to see specialists.
Nearly half of Medicare Advantage plan directories contained inaccurate information on what providers were available, according to the most recent federal review. Beginning in 2024, new or expanding Medicare Advantage plans must demonstrate compliance with federal network expectations or their applications could be denied.
Amanda Lansford, a Premera Blue Cross spokesperson, declined to comment on Timmins’ case. She said the plan meets federal network adequacy requirements as well as travel time and distance standards “to ensure members are not experiencing undue burdens when seeking care.”
Traditional Medicare allows beneficiaries to go to nearly any doctor or hospital in the U.S., and in most cases enrollees do not need approval to get services.
Timmins, who recently finished immunotherapy, said he doesn’t think he would be approved for a Medigap policy, “because of my health issue.” And if he were to get into one, Timmins said, it would likely be too expensive.
For now, Timmins said, he is staying with his Medicare Advantage plan.
“I’m getting older. More stuff is going to happen.”
There is also a chance, Timmins said, that his cancer could resurface: “I’m very aware of my mortality.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

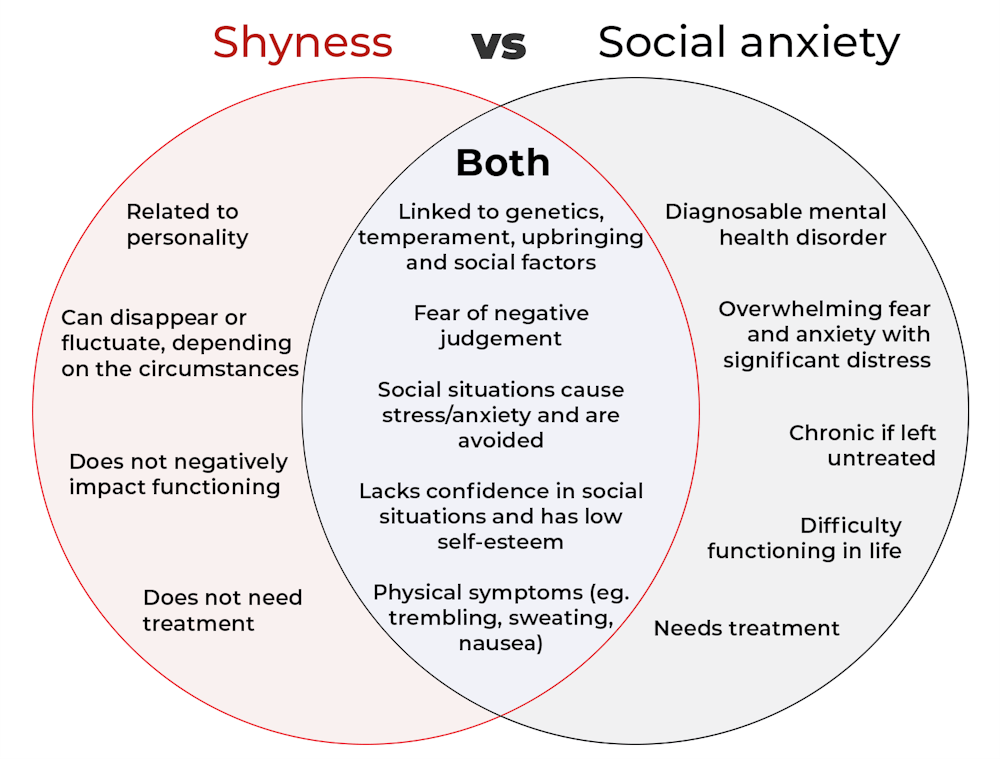
What’s the difference between shyness and social anxiety?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
The terms “shyness” and “social anxiety” are often used interchangeably because they both involve feeling uncomfortable in social situations.
However, feeling shy, or having a shy personality, is not the same as experiencing social anxiety (short for “social anxiety disorder”).
Here are some of the similarities and differences, and what the distinction means.

pathdoc/Shutterstock How are they similar?
It can be normal to feel nervous or even stressed in new social situations or when interacting with new people. And everyone differs in how comfortable they feel when interacting with others.
For people who are shy or socially anxious, social situations can be very uncomfortable, stressful or even threatening. There can be a strong desire to avoid these situations.
People who are shy or socially anxious may respond with “flight” (by withdrawing from the situation or avoiding it entirely), “freeze” (by detaching themselves or feeling disconnected from their body), or “fawn” (by trying to appease or placate others).
A complex interaction of biological and environmental factors is also thought to influence the development of shyness and social anxiety.
For example, both shy children and adults with social anxiety have neural circuits that respond strongly to stressful social situations, such as being excluded or left out.
People who are shy or socially anxious commonly report physical symptoms of stress in certain situations, or even when anticipating them. These include sweating, blushing, trembling, an increased heart rate or hyperventilation.
How are they different?
Social anxiety is a diagnosable mental health condition and is an example of an anxiety disorder.
For people who struggle with social anxiety, social situations – including social interactions, being observed and performing in front of others – trigger intense fear or anxiety about being judged, criticised or rejected.
To be diagnosed with social anxiety disorder, social anxiety needs to be persistent (lasting more than six months) and have a significant negative impact on important areas of life such as work, school, relationships, and identity or sense of self.
Many adults with social anxiety report feeling shy, timid and lacking in confidence when they were a child. However, not all shy children go on to develop social anxiety. Also, feeling shy does not necessarily mean a person meets the criteria for social anxiety disorder.
People vary in how shy or outgoing they are, depending on where they are, who they are with and how comfortable they feel in the situation. This is particularly true for children, who sometimes appear reserved and shy with strangers and peers, and outgoing with known and trusted adults.
Individual differences in temperament, personality traits, early childhood experiences, family upbringing and environment, and parenting style, can also influence the extent to which people feel shy across social situations.
Not all shy children go on to develop social anxiety. 249 Anurak/Shutterstock However, people with social anxiety have overwhelming fears about embarrassing themselves or being negatively judged by others; they experience these fears consistently and across multiple social situations.
The intensity of this fear or anxiety often leads people to avoid situations. If avoiding a situation is not possible, they may engage in safety behaviours, such as looking at their phone, wearing sunglasses or rehearsing conversation topics.
The effect social anxiety can have on a person’s life can be far-reaching. It may include low self-esteem, breakdown of friendships or romantic relationships, difficulties pursuing and progressing in a career, and dropping out of study.
The impact this has on a person’s ability to lead a meaningful and fulfilling life, and the distress this causes, differentiates social anxiety from shyness.
Children can show similar signs or symptoms of social anxiety to adults. But they may also feel upset and teary, irritable, have temper tantrums, cling to their parents, or refuse to speak in certain situations.
If left untreated, social anxiety can set children and young people up for a future of missed opportunities, so early intervention is key. With professional and parental support, patience and guidance, children can be taught strategies to overcome social anxiety.
Why does the distinction matter?
Social anxiety disorder is a mental health condition that persists for people who do not receive adequate support or treatment.
Without treatment, it can lead to difficulties in education and at work, and in developing meaningful relationships.
Receiving a diagnosis of social anxiety disorder can be validating for some people as it recognises the level of distress and that its impact is more intense than shyness.
A diagnosis can also be an important first step in accessing appropriate, evidence-based treatment.
Different people have different support needs. However, clinical practice guidelines recommend cognitive-behavioural therapy (a kind of psychological therapy that teaches people practical coping skills). This is often used with exposure therapy (a kind of psychological therapy that helps people face their fears by breaking them down into a series of step-by-step activities). This combination is effective in-person, online and in brief treatments.
Treatment is available online as well as in-person. ImYanis/Shutterstock For more support or further reading
Online resources about social anxiety include:
- This Way Up’s online program for managing excessive shyness and fear of social situations
- Beyond Blue’s resources on social anxiety
- a guide to looking after yourself if you have social anxiety, from the Western Australian health department
- social anxiety online program for children and teens from the University of Queensland
- inroads, a self-guided online program for young adults who drink alcohol to manage their anxiety.
We thank the Black Dog Institute Lived Experience Advisory Network members for providing feedback and input for this article and our research.
Kayla Steele, Postdoctoral research fellow and clinical psychologist, UNSW Sydney and Jill Newby, Professor, NHMRC Emerging Leader & Clinical Psychologist, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Apple vs Cucumber – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apple to cucumber, we picked the cucumber.
Why?
In terms of macros, apples have more carbs and fiber, while the ratio of these means that cucumber has the lower glycemic index. This could be spun either way, so in the interests of fairness, we’ll call this first round a tie.
In the category of vitamins, apples have more of vitamins C and E, while cucumber has more of vitamins A, B1, B2, B3, B5, B7, and K, winning.
Looking at minerals, apples are not higher in any minerals, while cucumber has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, winning completely here.
In other considerations, cucumber extract has amazing anti-inflammatory properties (which you can learn more about in the “learn more” section below), so that’s another point in its favor.
Adding up the sections makes for a clear overall win for cucumber, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
Cucumber Extract Beats Glucosamine & Chondroitin… At 1/135th Of The Dose?!
Enjoy!
Share This Post




-

Building & Maintaining Mobility
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Building & Maintaining Mobility!

This is Juliet Starrett. She’s a CrossFit co-founder, and two-time white-water rafting world champion. Oh, and she won those after battling thyroid cancer. She’s now 50 years old, and still going strong, having put aside her career as a lawyer to focus on fitness. Specifically, mobility training.
The Ready State
Together with her husband Kelly, Starrett co-founded The Ready State, of which she’s CEO.
It used to be called “Mobility WOD” (the “WOD” stands for “workout of the day”) but they changed their name as other companies took up the use of the word “mobility”, something the fitness world hadn’t previously focussed on much, and “WOD”, which was also hardly copyrightable.
True to its origins, The Ready State continues to offer many resources for building and maintaining mobility.
Why the focus on mobility?
When was the last time you had to bench-press anything larger than a small child? Or squat more than your partner’s bodyweight? Or do a “farmer’s walk” with anything heavier than your groceries?
For most of us, unless our lifestyles are quite extreme, we don’t need ridiculous strength (fun as that may be).
You know what makes a huge difference to our quality of life though? Mobility.
Have you ever felt that moment of panic when you reach for something on a high shelf and your shoulder or back twinges (been there!)? Or worse, you actually hurt yourself and the next thing you know, you need help putting your socks on (been there, too!)?
And we say to ourselves “I’m not going to let that happen to me again”
But how? How do we keep our mobility strong?
First, know your weaknesses
Starrett is a big fan of mobility tests to pinpoint areas that need more work.
Most of her resources for this aren’t free, and we’re drawing heavily from her book here, so for your convenience, we’ll link to some third party sources for this:
- Timed Up and Go—start with this, before progressing to the next!
- Sit To Rise Test—not to be underestimated (this page also has excerpts from Starrett’s mobility book, by the way)
- Shoulders/Spine/Hips—7 quick tests; note any that you can’t do, or struggle with
Next, eliminate those weaknesses
Do mobility exercises in any weak areas, until they’re not weak:
Want to train the full body in one session?
Try out The Ready State’s 10-Minute Morning Mobility Routine
Want to learn more?
You might enjoy her book that we reviewed previously:
Built to Move: The Ten Essential Habits to Help You Move Freely and Live Fully
You might also enjoy The Ready State App, available for iOS and for Android:
The Ready State Virtual Mobility Coach
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
You Don’t Need To Stretch After Your Workout For Better Flexibility
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Liv Townsend, flexibility coach, explains why:
Some of the claimed benefits are a bit of a stretch
The reason you don’t need to stretch after a workout to improve flexibility is because research doesn’t show meaningful benefits for recovery, soreness, or muscle “relengthening.”
On which note: contrary to a myth floating around, muscles don’t permanently shorten from strength training, so there’s nothing that needs to be “stretched back out” after a session.
To bust a few further myths: post-workout stretching also doesn’t meaningfully reduce delayed-onset muscle soreness, speed up recovery, or “flush out lactic acid”.
So, why do you sometimes feel tight after a workout? It’s just because of increased blood flow (the “pump”) and/or fatigue affecting how smoothly your muscles contract and relax, that’s all.
In reality, lifting through a full range of motion already stretches your muscles under load, which can improve flexibility as effectively—or sometimes more effectively—than passive stretching. For this reason, movements that allow deeper ranges contribute more to flexibility than partial-range exercises.
That said, passive stretching does still have a role, because static stretching (a kind of passive stretching) improves flexibility by training your nervous system to tolerate more stretching, which is different from what strength training provides.
Still, the timing of when you do that doesn’t matter much; stretching works through consistent exposure over time, not because it’s done immediately after a workout.
A practical approach instead: if you’re short on time and/or dislike post-workout stretching, skip it and instead do dedicated stretching sessions 2x per week for 10–15 minutes.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Overdone It? How To Speed Up Recovery After Exercise ← for what actually helps in that regard!
PS: this above-linked article of ours also cites some of the research being talked about above, and further details how post-workout stretching probably won’t help—so you know we’re singing from the same songsheet on this one!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Eggplant vs Mushroom – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing eggplant to mushrooms, we picked the mushrooms.
Why?
Well, there wasn’t mushroom for disagreement!
But first, you may be wondering: which mushrooms? Button mushrooms? White mushrooms? Chestnut mushrooms? Portobello mushrooms? And the answer is yes.
Those (and more; it represents most mushrooms that are commonly sold fresh in western supermarkets) are all the same species at different ages; namely, Agaricus bisporus—not to be mistaken for fly agaric, which despite the name, is not even a member of the Agaricus genus, and is in fact Amanita muscari. This is an important distinction, because fly agaric is poisonous, though fatality is rare, and it’s commonly enjoyed recreationally (after some preparation, which reduces its toxicity) for its psychoactive effects. It’s the famous red one with white spots. Anyway, today we will be talking instead about Agaricus bisporus, which is most popular western varieties of “edible mushroom”.
Of course, technically all mushrooms are edible, just, some of them are edible only once 😉
(the above line is a joke, please do not eat the kind that will kill you)
With all that in mind, let’s get down to it:
In terms of macros, eggplant has nearly 2x the carbs and 3x the fiber, while mushrooms contain more than 3x the protein. We’ll call this a tie for macros.
In the category of vitamins, eggplant is higher in vitamins A, E, and K, while mushrooms contain more of vitamins B1, B2, B3, B5, B6, B7, B9, B12, and D. Most notably for vegans, mushrooms are a good non-animal source of vitamins B12 and D3, which nutrients are not generally found in plants. Mushrooms, of course, are not technically plants. In any case, the vitamins category is an easy win for mushrooms.
When it comes to minerals, eggplant has more calcium, magnesium, and manganese, while mushrooms have more copper, iron, phosphorus, potassium, selenium, and zinc. One more strong round in mushrooms’ favor!
One final thing worth noting is that mushrooms are a rich source of the amino acid ergothioneine, which has been called a “longevity vitamin” for its healthspan-increasing effects (see our article below), so that’s one more point for mushrooms.
Adding up the sections makes for an overwhelming win for mushrooms, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
The Magic Of Mushrooms: “The Longevity Vitamin” (That’s Not A Vitamin)
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: