The Uses of Delusion – by Dr. Stuart Vyse
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most of us try to live rational lives. We try to make the best decisions we can based on the information we have… And if we’re thoughtful, we even try to be aware of common logical fallacies, and overcome our personal biases too. But is self-delusion ever useful?
Dr. Stuart Vyse, psychologist and Fellow for the Committee for Skeptical Inquiry, argues that it can be.
From self-fulfilling prophecies of optimism and pessimism, to the role of delusion in love and loss, Dr. Vyse explores what separates useful delusion from dangerous irrationality.
We also read about such questions as (and proposed answers to):
- Why is placebo effect stronger if we attach a ritual to it?
- Why are negative superstitions harder to shake than positive ones?
- Why do we tend to hold to the notion of free will, despite so much evidence for determinism?
The style of the book is conversational, and captivating from the start; a highly compelling read.
Bottom line: if you’ve ever felt yourself wondering if you are deluding yourself and if so, whether that’s useful or counterproductive, this is the book for you!
Click here to check out The Uses of Delusion, and optimize yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Addiction Myths That Are Hard To Quit

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Which Addiction-Quitting Methods Work Best?

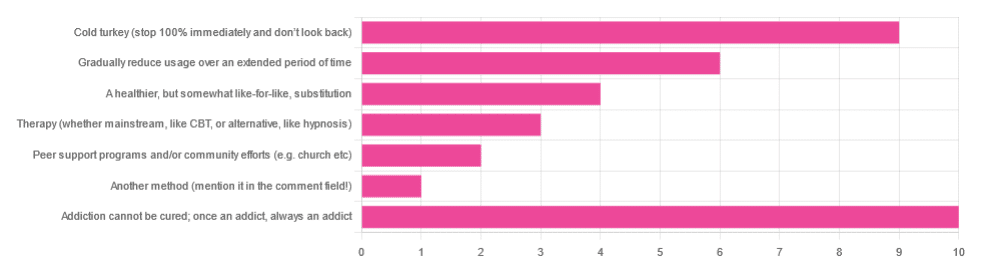
In Tuesday’s newsletter we asked you what, in your opinion, is the best way to cure an addiction. We got the above-depicted, below-described, interesting distribution of responses:
- About 29% said: “Addiction cannot be cured; once an addict, always an addict”
- About 26% said “Cold turkey (stop 100% and don’t look back)”
- About 17% said “Gradually reduce usage over an extended period of time”
- About 11% said “A healthier, but somewhat like-for-like, substitution”
- About 9% said “Therapy (whether mainstream, like CBT, or alternative, like hypnosis)”
- About 6% said “Peer support programs and/or community efforts (e.g. church etc)”
- About 3% said “Another method (mention it in the comment field)” and then did not mention it in the comment field
So what does the science say?
Addiction cannot be cured; once an addict, always an addict: True or False?
False, which some of the people who voted for it seemed to know, as some went on to add in the comment field what they thought was the best way to overcome the addiction.
The widespread belief that “once an addict, always an addict” is a “popular truism” in the same sense as “once a cheater, always a cheater”. It’s an observation of behavioral probability phrased as a strong generalization, but it’s not actually any kind of special unbreakable law of the universe.
And, certainly the notion that one cannot be cured keeps membership in many 12-step programs and similar going—because if you’re never cured, then you need to stick around.
However…
❝What is the definition of addiction?
Addiction is a treatable, chronic medical disease involving complex interactions among brain circuits, genetics, the environment, and an individual’s life experiences. People with addiction use substances or engage in behaviors that become compulsive and often continue despite harmful consequences.
Prevention efforts and treatment approaches for addiction are generally as successful as those for other chronic diseases.❞
~ American Society of Addiction Medicine
Or if we want peer-reviewed source science, rather than appeal to mere authority as above, then:
❝What is drug addiction?
Addiction is defined as a chronic, relapsing disorder characterized by compulsive drug seeking and use despite adverse consequences. It is considered a brain disorder, because it involves functional changes to brain circuits involved in reward, stress, and self-control. Those changes may last a long time after a person has stopped taking drugs.
Addiction is a lot like other diseases, such as heart disease. Both disrupt the normal, healthy functioning of an organ in the body, both have serious harmful effects, and both are, in many cases, preventable and treatable.❞
~ Nora D. Volkow (Director, National Institute of Drug Abuse)
Read more: Drugs, Brains, and Behavior: The Science of Addiction
In short: part of the definition of addiction is the continued use; if the effects of the substance are no longer active in your physiology, and you are no longer using, then you are not addicted.
Just because you would probably become addicted again if you used again does not make you addicted when neither the substance nor its after-effects are remaining in your body. Otherwise, we could define all people as addicted to all things based on “well if they use in the future they will probably become addicted”.
This means: the effects of addiction can and often will last for long after cessation of use, but ultimately, addiction can be treated and cured.
(yes, you should still abstain from the thing to which you were formerly addicted though, or you indeed most probably will become addicted again)
Cold turkey is best: True or False?
True if and only if certain conditions are met, and then only for certain addictions. For all other situations… False.
To decide whether cold turkey is a safe approach (before even considering “effective”), the first thing to check is how dangerous the withdrawal symptoms are. In some cases (e.g. alcohol, cocaine, heroin, and others), the withdrawal symptoms can kill.
That doesn’t mean they will kill, so knowing (or being!) someone who quit this way does not refute this science by counterexample. The mortality rates that we saw while researching varied from 8% to 37%, so most people did not die, but do you really want (yourself or a loved one) to play those odds unnecessarily?
See also: Detoxification and Substance Abuse Treatment
Even in those cases where it is considered completely safe for most people to quit cold turkey, such as smoking, it is only effective when the quitter has appropriate reliable medical support, e.g.
- Without support: 3–5% success rate
- With support: 22% success rate
And yes, that 22% was for the “abrupt cessation” group; the “gradual cessation” group had a success rate of 15.5%. On which note…
Gradual reduction is the best approach: True or False?
False based on the above data, in the case of addictions where abrupt cessation is safe. True in other cases where abrupt cessation is not safe.
Because if you quit abruptly and then die from the withdrawal symptoms, then well, technically you did stay off the substance for the rest of your life, but we can’t really claim that as a success!
A healthier, but somewhat like-for-like substitution is best: True or False?
True where such is possible!
This is why, for example, medical institutions recommend the use of buprenorphine (e.g. Naloxone) in the case of opioid addiction. It’s a partial opioid receptor agonist, meaning it does some of the job of opioids, while being less dangerous:
It’s also why vaping—despite itself being a health hazard—is recommended as a method of quitting smoking:
Similarly, “zero alcohol drinks that seem like alcohol” are a popular way to stop drinking alcohol, alongside other methods:
This is also why it’s recommended that if you have multiple addictions, to quit one thing at a time, unless for example multiple doctors are telling you otherwise for some specific-to-your-situation reason.
Take care!
Share This Post
-

Bird flu has been detected in a pig in the US. Why does that matter?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The United States Department of Agriculture last week reported that a pig on a backyard farm in Oregon was infected with bird flu.
As the bird flu situation has evolved, we’ve heard about the A/H5N1 strain of the virus infecting a range of animals, including a variety of birds, wild animals and dairy cattle.
Fortunately, we haven’t seen any sustained spread between humans at this stage. But the detection of the virus in a pig marks a worrying development in the trajectory of this virus.

David MG/Shutterstock How did we get here?
The most concerning type of bird flu currently circulating is clade 2.3.4.4b of A/H5N1, a strain of influenza A.
Since 2020, A/H5N1 2.3.4.4b has spread to a vast range of birds, wild animals and farm animals that have never been infected with bird flu before.
While Europe is a hotspot for A/H5N1, attention is currently focused on the US. Dairy cattle were infected for the first time in 2024, with more than 400 herds affected across at least 14 US states.
Bird flu has enormous impacts on farming and commercial food production, because infected poultry flocks have to be culled, and infected cows can result in contaminated diary products. That said, pasteurisation should make milk safe to drink.
While farmers have suffered major losses due to H5N1 bird flu, it also has the potential to mutate to cause a human pandemic.
Birds and humans have different types of receptors in their respiratory tract that flu viruses attach to, like a lock (receptors) and key (virus). The attachment of the virus allows it to invade a cell and the body and cause illness. Avian flu viruses are adapted to birds, and spread easily among birds, but not in humans.
So far, human cases have mainly occurred in people who have been in close contact with infected farm animals or birds. In the US, most have been farm workers.
The concern is that the virus will mutate and adapt to humans. One of the key steps for this to happen would be a shift in the virus’ affinity from the bird receptors to those found in the human respiratory tract. In other words, if the virus’ “key” mutated to better fit with the human “lock”.
A recent study of a sample of A/H5N1 2.3.4.4b from an infected human had worrying findings, identifying mutations in the virus with the potential to increase transmission between human hosts.
Why are pigs a problem?
A human pandemic strain of influenza can arise in several ways. One involves close contact between humans and animals infected with their own specific flu viruses, creating opportunities for genetic mixing between avian and human viruses.
Pigs are the ideal genetic mixing vessel to generate a human pandemic influenza strain, because they have receptors in their respiratory tracts which both avian and human flu viruses can bind to.
This means pigs can be infected with a bird flu virus and a human flu virus at the same time. These viruses can exchange genetic material to mutate and become easily transmissible in humans.
The Conversation, CC BY-SA Interestingly, in the past pigs were less susceptible to A/H5N1 viruses. However, the virus has recently mutated to infect pigs more readily.
In the recent case in Oregon, A/H5N1 was detected in a pig on a non-commercial farm after an outbreak occurred among the poultry housed on the same farm. This strain of A/H5N1 was from wild birds, not the one that is widespread in US dairy cows.
The infection of a pig is a warning. If the virus enters commercial piggeries, it would create a far greater level of risk of a pandemic, especially as the US goes into winter, when human seasonal flu starts to rise.
How can we mitigate the risk?
Surveillance is key to early detection of a possible pandemic. This includes comprehensive testing and reporting of infections in birds and animals, alongside financial compensation and support measures for farmers to encourage timely reporting.
Strengthening global influenza surveillance is crucial, as unusual spikes in pneumonia and severe respiratory illnesses could signal a human pandemic. Our EPIWATCH system looks for early warnings of such activity, which can speed up vaccine development.
If a cluster of human cases occurs, and influenza A is detected, further testing (called subtyping) is essential to ascertain whether it’s a seasonal strain, an avian strain from a spillover event, or a novel pandemic strain.
Early identification can prevent a pandemic. Any delay in identifying an emerging pandemic strain enables the virus to spread widely across international borders.
Australia’s first human case of A/H5N1 occurred in a child who acquired the infection while travelling in India, and was hospitalised with illness in March 2024. At the time, testing revealed Influenza A (which could be seasonal flu or avian flu), but subtyping to identify A/H5N1 was delayed.
This kind of delay can be costly if a human-transmissible A/H5N1 arises and is assumed to be seasonal flu because the test is positive for influenza A. Only about 5% of tests positive for influenza A are subtyped further in Australia and most countries.
In light of the current situation, there should be a low threshold for subtyping influenza A strains in humans. Rapid tests which can distinguish between seasonal and H5 influenza A are emerging, and should form part of governments’ pandemic preparedness.
A higher risk than ever before
The US Centers for Disease Control and Prevention states that the current risk posed by H5N1 to the general public remains low.
But with H5N1 now able to infect pigs, and showing worrying mutations for human adaptation, the level of risk has increased. Given the virus is so widespread in animals and birds, the statistical probability of a pandemic arising is higher than ever before.
The good news is, we are better prepared for an influenza pandemic than other pandemics, because vaccines can be made in the same way as seasonal flu vaccines. As soon as the genome of a pandemic influenza virus is known, the vaccines can be updated to match it.
Partially matched vaccines are already available, and some countries such as Finland are vaccinating high-risk farm workers.
C Raina MacIntyre, Professor of Global Biosecurity, NHMRC L3 Research Fellow, Head, Biosecurity Program, Kirby Institute, UNSW Sydney and Haley Stone, Research Associate, Biosecurity Program, Kirby Institute & CRUISE lab, Computer Science and Engineering, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The End of Food Allergy – by Dr. Kari Nadeau & Sloan Barnett
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We don’t usually mention author credentials beyond their occupation/title. However, in this case it bears acknowledging at least the first line of the author bio:
❝Kari Nadeau, MD, PhD, is the director of the Sean N. Parker Center for Allergy and Asthma Research at Stanford University and is one of the world’s leading experts on food allergy❞
We mention this, because there’s a lot of quack medicine out there [in general, but especially] when it comes to things such as food allergies. So let’s be clear up front that Dr. Nadeau is actually a world-class professional at the top of her field.
This book is, by the way, about true allergies—not intolerances or sensitivities. It does touch on those latter two, but it’s not the main meat of the book.
In particular, most of the research cited is around peanut allergies, though the usual other common allergens are all discussed too.
The authors’ writing style is that of a science educator (Dr. Nadeau’s co-author, Sloan Barnett, is lawyer and health journalist). We get a clear explanation of the science from real-world to clinic and back again, and are left with a strong understanding, not just a conclusion.
The titular “End of Food Allergy” is a bold implicit claim; does the book deliver? Yes, actually.
The book lays out guidelines for safely avoiding food allergies developing in infants, and yes, really, how to reverse them in adults. But…
Big caveat:
The solution for reversing severe food allergies (e.g. “someone nearby touched a peanut three hours ago and now I’m in anaphylactic shock”), drug-assisted oral immunotherapy, takes 6–24 months of weekly several-hour-long clinic visits, relies on having a nearby clinic offering the service, and absolutely 100% cannot be done at home (on pain of probable death).
Bottom line: it’s by no means a magic bullet, but yes, it does deliver.
Click here to check out The End of Food Allergy to learn more!
Share This Post




-

Algorithms to Live By – by Brian Christian and Tom Griffiths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As humans, we subconsciously use heuristics a lot to make many complex decisions based on “fuzzy logic”. For example:
Do we buy the cheap shoes that may last us a season, or the much more expensive ones that will last us for years? We’ll—without necessarily giving it much conscious thought—quickly weigh up:
- How much do we like each prospective pair of shoes?
- What else might we need to spend money on now/soon?
- How much money do we have right now?
- How much money do we expect to have in the future?
- Considering our lifestyle, how important is it to have good quality shoes?
How well we perform this rapid calculation may vary wildly, depending on many factors ranging from the quality of the advertising to how long ago we last ate.
And if we make the wrong decision, later we may have buyer’s (or non-buyer’s!) remorse. So, how can we do better?
Authors Brain Christian and Tom Griffiths have a manual for us!
This book covers many “kinds” of decision we often have to make in life, and how to optimize those decisions with the power of mathematics and computer science.
The problems (and solutions) run the gamut of…
- Optimal stopping (when to say “alright, that’s good enough”)
- Overcoming cognitive biases
- Scheduling quandaries
- Bayes’ Theorem
- Game Theory
- And when it’s more efficient to just leave things to chance!
…and many more (12 main areas of decision-making are covered).
For all it draws heavily from mathematics and computer science, the writing style is very easy-reading. It’s a “curl up in the armchair and read for pleasure” book, no matter how weighty and practical its content.
Bottom line: if you improve your ability to make the right decisions even marginally, this book will have been worth your while in the long run!
Order your copy of “Algorithms To Live By” from Amazon today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Zucchini vs Okra – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing zucchini to okra, we picked the okra.
Why?
Looking at the macros first, okra has nearly 2x the protein and more than 3x the fiber (for about 2x the carbs).
In terms of vitamins, things are also quite one-sided; zucchini has a little more vitamin B2, while okra has a lot more of vitamins A, B1, B3, B5, B6, B9, C, E, K, and choline.
Nor does the mineral situation make any compelling counterargument; zucchini is higher only in sodium, while okra has a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium*, selenium, and zinc.
*Actually it’s only a little more potassium. But the rest are with big margins of difference.
Both of these on-the-cusp-of-being-pungent vegetables have beneficial antioxidant polyphenols (especially various forms of quercetin), but okra has more.
In short: enjoy both, of course, but there’s a clear winner here and it’s okra.
Want to learn more?
You might like to read:
Enjoy Bitter/Astringent/Pungent Foods For Your Heart & Brain
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Feta or Parmesan – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing feta to parmesan, we picked the parmesan.
Why?
It’s close! Looking at the macros, parmesan has more protein and slightly less fat. Of the fat content, parmesan also has slightly less saturated fat, but neither of them are doing great in this category. Still, a relative win for parmesan.
In the category of vitamins, feta is a veritable vitamin-B-fest with more of vitamins B1, B2, B3, B5, B6, and B9. On the other hand, parmesan has more of vitamins A, B12, and choline. By strength of numbers, this is a win for feta.
Minerals tell a different story; parmesan has a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Meanwhile, feta is not higher in any minerals. A clear win for parmesan.
Both cheeses offer gut-healthy benefits (if consumed regularly in small portions), while neither are great for the heart.
On balance, we say parmesan wins the day.
Want to learn more?
You might like to read:
Feta Cheese vs Mozzarella – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: