How To Lower Your Cholesterol By 50+ Points Without Drugs
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Siobhan Deshauer explains:
The Plan
She recommends:
- Dietary patterns: rather than tracking individual nutrients, follow Mediterranean, DASH, or plant-based diets; these reduce LDL and heart risk by emphasizing whole foods and minimizing processed foods and animal fats
- Plant proteins: replacing animal proteins with legumes, seeds, and nuts lowers LDL by 6 points; benefits come from lower saturated fat and added fiber and sterols
- Soluble fiber: traps cholesterol in the gut and removes it through stool; 1g of soluble fiber may reduce LDL by 2 points; psyllium can lower LDL by 13 points with 2 tbsp/day
- Phytosterols/stanols: plant-based cholesterol analogs can lower LDL by 5–10 points at 2g/day, but hard to get from diet alone; supplements may help, but carry risks for hyperabsorbers
- Unfiltered coffee: brewing methods like espresso, French press, and Turkish coffee retain cafestol, which raises LDL; using a paper filter can lower LDL by 15 points
- Probiotics: early studies show they may lower LDL by 8 points, but individual products vary too much to recommend supplements; fermented foods like kimchi, yogurt, and kefir can reliably help though
- Exercise: moderate cardio (4×/week) can reduce LDL by 5–6 points; adding weight training may drop it by 11 points; exercise improves overall cardiovascular health even if LDL impact is modest
- Weight loss: long-term loss of 1kg can reduce LDL by 1.3 points; effect strongest for those starting at higher BMI
You might notice, therefore, that the results of some things might not be what you’d expect. For example, using a paper filter when making coffee can lower LDL more than 10x more than losing 1kg of weight. Yet for some reason, that’s rarely what’s first to get recommended to a patient.
So, you don’t have to do everything on the list, but choose wisely! For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Lower Cholesterol Naturally ← our own main feature on such
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Some patients wait 6 years to see a public hospital specialist. Here’s how to fix this

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
ABC analysis shows some patients wait six years or more for outpatient medical appointments in Australia’s public hospital system.
According to the ABC, the delays are longest in parts of South Australia, where some patients waited more than six years to see a neurologist and 5.5 years to see ear, nose and throat (ENT) specialists and gastroenterologists.
In parts of Tasmania, waits for ENT specialists, neurologists and urologists were almost five years. Some families needing their child assessed for allergies waited more than five years.
Some patients find their condition deteriorates as they wait. Others live with chronic pain. All live with uncertainty. In our past interviews patients described “becoming more anxious”, and feeling “forgotten” and “alone […] like no one cares”.
Health Minister Mark Butler says the government is working to bolster the medical workforce. But while training more specialist doctors is an important part of a long-term plan, it’s not the only thing needed to reduce outpatient wait times.
Our research spanning more than a decade shows there are ways to reduce waiting lists that can be implemented now.

SDI Productions/Getty Images What’s going wrong?
When a patient needs to see a specialist but doesn’t require hospitalisation, a GP or emergency department can refer them to a public outpatient clinic. In a public outpatient clinic, they can see a specialist or allied health provider – or receive a test or treatment – for free.
Some patients may go on to have elective surgery, but they must first wait for an outpatient appointment.
There are around 41 million public hospital outpatient visits each year. But data isn’t routinely collected on how long patients wait for outpatient appointments, so it’s often referred to as the “hidden waiting list”.
Outpatient services typically manage their demand using a triaged waiting list. Referrals are received, given a triage category based on urgency and placed on a waiting list, to be contacted when a place eventually becomes available.
There are several problems with this approach.
First, it’s difficult to come up with systems to make fair decisions about who should be seen first, which can turn access into a lottery.
Second, triage systems weigh up the needs of patients as they arrive but don’t reassess the priority of those already in the system.
Third, managing long waiting lists diverts resources from patient care, but poorly maintained lists create inefficiencies and are demoralising for health providers, contributing to burnout.
Finally, the unlucky patients at the lowest triage level are constantly overtaken by those entering at higher priority.
First, clean up the list
Our research shows investing in short-term, targeted strategies can reduce outpatient backlogs.
We tackled a waiting list of 600 patients in a neurology outpatient clinic. We found the list was full of errors, patients who no longer wanted or needed the service, and patients who had previously been offered appointments but never attended.
In the end, only 11% of patients still required an appointment.
Then consider supply and demand
These strategies work in the short term but waiting lists will soon grow back if underlying imbalances between supply and demand are not addressed.
We created a new approach to address this issue. It starts with an analysis of supply and demand, followed by protecting sufficient capacity in clinic schedules to see all new patients at the rate they arrive.
These changes are coupled with short-term, targeted strategies to reduce existing waiting lists, enabling services to “catch up” while underlying service changes allow them to “keep up”.
On referral, all patients get rapid access to a first appointment but are then triaged for ongoing care according to need – anything from a brief assessment and advice to intensive ongoing treatment.
Using more of each health workers’ skills
Thinking creatively about models of care can then help to maximise the value of specialised clinicians. Empowering allied health professionals or nurses to see less straightforward cases or conduct preparatory assessments can free up specialists’ time to provide complex assessment and treatment.
Some care can be delivered by different types of health-care providers without compromising quality.
Physiotherapists, for example, have been shown to be very effective at assessing some patients waiting for hip and knee joint replacements and identifying those who might benefit from exercise-based treatment, allowing orthopaedic surgeons to focus on those who require surgery.
Investing in clerical staff can ensure patients have the information they need to get to their appointments at the right time, with the right test results in hand.
Testing this approach
In a trial involving more than 3,000 patients, we tested the model across eight allied health and community services in Victoria. These services provide care from professionals such as physiotherapists and occupational therapists, as well as team-based services such as memory clinics, in the community.
Each participating service received a small grant to support targeted strategies to address the existing backlog, such as waiting lists audits, but no ongoing additional funding. Changes were made by reorganising existing resources, not adding new ones.
This multi-pronged approach reduced waiting time by 34% with minimal extra resources. Median waiting times reduced from 42 to 24 days, with bigger reductions for the longest waiters. This model is now being widely used in Victorian Community Health Services.
We are now testing this way of managing demand in a group of outpatient medical specialist clinics with waiting lists of 13,000 patients to see if it can work at the scale required in specialist clinics at public hospitals.
It’s still early days but initial signs are promising, suggesting that waiting lists can be reduced by better understanding supply and demand, cleaning up long waiting lists, and using more of each health-care workers’ skills.
Nicholas Taylor (Professor of Allied Health at La Trobe University and Eastern Health) and Annie Lewis (Post-Doctoral Researcher at La Trobe University and Eastern Health) co-authored the research on which this article is based.
Katherine Harding, Professor of Allied Health and Implementation Science, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Ageless Aging – by Maddy Dychtwald
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Maddy Dychtwald, herself 73, has spent her career working in the field of aging. She’s not a gerontologist or even a doctor, but she’s nevertheless been up-to-the-ears in the industry for decades, mostly as an organizer, strategist, facilitator, and so forth. As such, she’s had her finger on the pulse of the healthy longevity movement for a long time.
This book was written to address a problem, and the problem is: lifespan is increasing (especially for women), but healthspan has not been keeping up the pace.
In other words: people (especially women) are living longer, but often with more health problems along the way than before.
And mostly, it’s for lack of information (or sometimes: too much competing incorrect information).
Fortunately, information is something that a woman in Dychtwald’s position has an abundance of, because she has researchers and academics in many fields on speed-dial and happy to answer her questions (we get a lot of input from such experts throughout the book—which is why this book is so science-based, despite the author not being a scientist).
The book answers a lot of important questions beyond the obvious “what diet/exercise/sleep/supplements/etc are best for healthy aging” (spoiler: it’s quite consistent with the things we recommend here, because guess what, science is science), questions like how best to prepare for this that or the other, how to get a head start on preventative healthcare for some things, how to avoid being a burden to our families (one can argue that families are supposed to look after each other, but still, it’s a legitimate worry for many, and understandably so), and even how to balance the sometimes conflicting worlds of health and finances.
Unlike many authors, she also talks about the different kinds of aging, and tackles each of them separately and together. We love to see it!
Bottom line: this book is a very good one-stop-shop for all things healthy aging. It’s aimed squarely at women, but most advice goes for men the same too, aside from the section on hormones and such.
Click here to check out Ageless Aging, and plan your future!
Share This Post
-

Apricots vs Peaches – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apricots to peaches, we picked the apricots.
Why?
Both are great! But there’s a clear winner:
In terms of macros, apricots have more fiber and, which is less important because the numbers are small, more protein. Apricots do also have more carbs, and/but carbs from whole fruit are not a problem for most people (especially because of the fiber), unless undertaking a very carb-controlled diet.
When it comes to vitamins, apricots sweep with more of vitamins A, B1, B2, B5, B6, B9, C, E, & K. Peaches meanwhile boast more vitamin B3, and that only marginally, as well as more choline.
In the category of minerals, apricots sweep again with more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc. Peaches are not higher in any minerals.
Finally, if we consider polyphenols, apricots sweep yet again. The flavonols that peaches have, apricots have more of, and apricots have a long list of flavonols that peaches don’t.
Outside of flavonols, there is one (1) phenolic acid that peaches have more of (it’s 3-Caffeoylquinic acid), and it’s only slightly more, and it’s mostly in the skin which isn’t included if you buy your fruit ready-chopped. So in those cases, apricots would have the higher 3-Caffeoylquinic acid content anyway.
All in all, with their higher content of fiber, vitamins, minerals, and polyphenols, apricots easily win the day.
Enjoy both, though! Diversity is healthy!
Want to learn more?
You might like to read:
- Dried Apricots vs Dried Prunes – Which is Healthier?
- Which Sugars Are Healthier, And Which Are Just The Same? ← we know we link this one a lot, but we think it’s important for everyone to know how fruit is good and juice isn’t (and why, less that seem bizarrely arbitrary)
Take care!
Share This Post


Related Posts
-
Music can affect your driving – but not always how you’d expect
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For many of us, listening to music is simply part of the driving routine – as ordinary as wearing a seatbelt. We build playlists for road trips, pick songs to stay awake, and even turn the volume up when traffic gets stressful.
More than 80% of drivers listen to music on most trips. And many young drivers find it difficult to concentrate without it.
We tend to think music relaxes us, energises us, or helps us focus when we’re behind the wheel.
But the science paints a more complicated picture. Decades of studies show music can sharpen some aspects of driving and dull others. And it affects young drivers differently from more experienced ones.
davidf/Getty Images How do researchers study driving and music?
Most studies use driving simulators, where participants drive through realistic road scenarios while researchers change only one thing: the music.
This allows precise measurement of indicators such as speed, reaction time, lane-keeping, braking, following distance, simulated collisions and even the driver’s physiological state under different music conditions.
Because everything else is held constant, any difference in driving performance can be attributed to the music.
Researchers have tested different music and driving scenarios in dozens of small studies – often with conflicting conclusions. To make sense of these results, researchers combine them in “meta-analyses” to see broad patterns.
So how does music affect our driving?
Meta-analyses show music changes how we drive in several ways.
Drivers listening to music tended to have more simulated collisions, poorer speed control and less stable following distances than those driving in silence.
Other outcomes such as lane position, signalling errors and pure reaction time show more mixed or inconsistent effects.
Music often changes the driver’s heart rate and makes it more variable. It also increases their arousal and mental workload, meaning how mentally “busy” or stretched they are while trying to drive.
Music can also help tired drivers stay alert on long, monotonous stretches but only for a short window. The boost fades by about 15 to 25 minutes.
So music can make you feel better and more alert, for shorter distances, even while it’s adding extra cognitive load and competing with the main task of driving.
Does the volume and type of music matter?
Volume does influence driving, but the effects are more subtle than many assume.
High- and medium-volume music tend to nudge drivers’ speeds slightly upward, while low-volume music consistently leads to slower driving. These effects are small, but relatively consistent in direction.
Fast music has a bad reputation, but the pooled evidence is less clear-cut. One meta-analysis found no overall effect of tempo on driving performance for an average driver. But it’s slightly different if you’re a novice driver.
Individual studies still suggest that very high-arousal, aggressive tracks can nudge some drivers toward riskier behaviour and make them more prone to errors. But tempo by itself doesn’t neatly predict safety.
Music tempo itself doesn’t predict safety. Gustavo Fring/Pexels Music you choose yourself tends to be less distracting than music imposed on you. Drivers often select music to regulate their mood and arousal – and that can stabilise their driving.
Conversely, several experiments show researcher-selected or imposed music leads to poorer performance: more collisions and violations, especially when the driver doesn’t like the music.
So it’s not just the music itself, but your relationship with it, that shapes how it affects your driving. Familiar or preferred music tends to maintain mood and reduce stress without adding as much mental load.
Inexperienced drivers are more affected
Inexperienced drivers are more vulnerable to distraction from music.
One study of 20- to 28-year-old drivers found less-experienced drivers were far more disrupted by music than experienced drivers. When music was playing – especially upbeat, “happy” tracks – inexperienced drivers were much more likely to drift into speeding.
Experienced drivers didn’t, suggesting their experience acts as a buffer.
Another experiment found exposing young drivers to more aggressive genres such as metal or certain folk-pop led to higher speeds, more driving errors and reduced attention to road signs.
For novice drivers, fast-tempo music increased their mental load and reduced their ability to spot hazards. This meant they were slower or less accurate in their responses.
Slow music, on the other hand, didn’t raise inexperienced drivers’ mental load and even moderately improved their ability to respond to hazards.
So what does this mean for my driving?
For most people, familiar songs, calmer genres and moderate volumes tend to create the least interference, while still keeping you alert and in a good mood.
Extremely loud, unfamiliar or highly aggressive tracks are the ones most likely to push up your speed, distract you, or overload your thinking.
But if you’re a newer driver, try turning the volume down, or even switching the music off, in demanding conditions.
Milad Haghani, Associate Professor and Principal Fellow in Urban Risk and Resilience, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Why is migraine more common in women than men?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve known for a long time that women are more likely than men to have migraine attacks.
As children, girls and boys experience migraine equally. But after puberty, women are two to three times more likely to experience this potentially debilitating condition.
Recently, an Australian study showed it may be even more common than we previously thought – as many as one in three women live with migraine.
For comparison, migraine affects roughly one in 15 men in Australia.
So, what’s behind the difference? Here’s what we know.
More than a headache
Migraine is not just a bad headache – it is a complex disorder that causes the brain to process sensory information abnormally.
This means “migraine brains” can have difficulty processing information from any of the five senses:
- sight (leading to problems with light sensitivity and glare)
- sound (leading to noise sensitivity)
- smell (certain smells can trigger headaches)
- touch (leading to face or scalp tenderness)
- taste (causing distorted taste, nausea and vomiting).
Migraine attacks typically last anywhere from four hours to three days – but can be longer.
In addition to the symptoms above, attacks can include throbbing head pain, dizziness, fatigue and difficulty concentrating. It is these extra symptoms that help diagnose migraine – not the location of head pain or pain severity.
Why are attacks more frequent in women?
Puberty is when the difference between men and women emerges. This is when our bodies massively increase the production of sex hormones.
People are often surprised to learn that both men and women produce oestrogen, progesterone and testosterone. Testosterone levels are higher in men, whereas women have higher levels of oestrogen and progesterone.
However, it is not just the type of hormone that makes a difference, but the way they fluctuate over time.
For many women, there are certain “milestone moments” when their migraine tends to worsen due to hormonal fluctuations – puberty, menstruation, pregnancy and perimenopause (the lead-up to your final period).
For example, some women notice migraine flare-ups every month, linked to phases in their monthly menstrual cycle when oestrogen levels drop.
They might even be able to predict when their period will start, as migraine attacks typically start a few days before the bleeding.
How hormones affect the brain
Women with migraine can be more sensitive to hormonal changes. This is particularly the case for sudden decreases in oestrogen. But even more subtle changes to hormone levels can cause migraine attacks.
These hormonal changes can activate brain processes that trigger migraine, such as cortical spreading depression. This is a very slow wave of electrical activity that spreads in the brain, causing some areas to function more slowly than others after it passes.
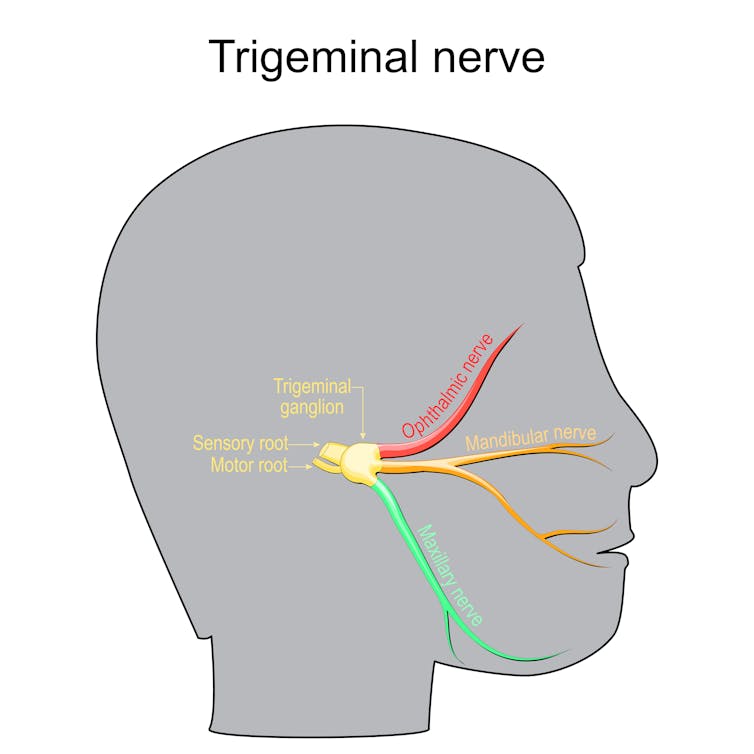
Decrease in oestrogen can also affect how we receive and process information through the trigeminal nerve. This plays a key role in the onset and maintenance of migraine pain.
Oestrogen can affect how we process information through the trigeminal nerve. ttsz/Getty All kinds of fluctuations can be a trigger
Pregnancy can often destabilise migraine again and make attacks more likely, even when someone has previously enjoyed a period of good migraine control.
Migraine symptoms often become uncontrolled in the first trimester in particular, due to rapid hormonal changes needed to sustain a pregnancy. This usually settles in the second and third trimesters, when hormonal changes stabilise.
However, giving birth is yet another change.
Towards the end of pregnancy, oestrogen levels can be 30 times higher than pre-pregnancy levels, and progesterone can be 20 times higher. When these hormones plummet back to normal after giving birth, migraine attacks can often sharply worsen again.
Perimenopause can also involve random surges of oestrogen from the dwindling supplies of eggs within the ovaries – which previously produced these hormones cyclically and in abundance. This irregular hormone production can cause random spikes in migraine attacks. It can be extra challenging when combined with other symptoms of menopause such as hot flushes or mood changes.
Hormonal contraceptives and menopause hormone therapy can also affect migraine control. Sometimes, supplementing hormones at a regular, steady daily dose can help manage the hormone-sensitive headaches and other symptoms. However, for others, adding extra hormones can cause head pain to flare up.
Does migraine run in the family?
Genes also play a role. It’s not a coincidence that migraine is passed down in families through the maternal side.
This is because mothers pass on mitochondria to children (while fathers do not). Mitochondria are parts inside the cell that control energy.
People with migraine have fewer functional enzymes within their mitochondria, meaning their brains are in an energy-deficient state. This worsens with migraine attacks as there is even more stress to the system.
This is also why extra stress (such as sleep deprivation, missed meals, or emotional stress) can trigger a migraine and worsen pain.
There is also a strong link between migraine in women and anxiety and depression – conditions women are more likely to develop in response to stressful life events.
Knowing your own patterns
If you suspect hormones may be affecting your migraine attacks, it is helpful to keep a diary of symptoms, including headaches. Mark each day per month where you get migraine symptoms, as well as your period, to find patterns.
Identifying patterns in pain flares helps doctors guide you to a personalised medication plan, which may include hormone therapies or non-hormonal therapies.
Lakshini Gunasekera, PhD Candidate in Neurology, Monash University; Caroline Gurvich, Associate Professor and Clinical Neuropsychologist, Monash University; Eveline Mu, Research Fellow in Women’s Mental Health, Monash University, and Jayashri Kulkarni, Professor of Psychiatry, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Asparagus vs Zucchini – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing asparagus to zucchini, we picked the asparagus.
Why?
It wasn’t close:
In terms of macros, asparagus has more fiber, carbs, and protein, making it the more nutritionally-dense option in this category.
In the category of vitamins, asparagus has more of vitamins A, B1, B2, B3, B5, B7, B9, E, K, and choline, while zucchini has more of vitamins B6 and C. An easy win for asparagus.
When it comes to minerals, asparagus has more calcium, copper, iron, phosphorus, selenium, and zinc, while zucchini has more magnesium and potassium. Another clear win for asparagus.
Looking at polyphenols, asparagus has 23.2mg/100g quercetin, while zucchini has 1.32mg/100g quercetin—one more easy win for asparagus.
Adding up the sections makes for an overwhelming win for asparagus, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Fight Inflammation & Protect Your Brain, With Quercetin
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: