Doctors From 15 Specialties Tell The Worst Common Mistakes People Make
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Whatever your professional background, you probably know many things about it that are very obvious to you, but that most people don’t know. So it is for doctors too; here are the things that doctors from 15 specialties would never do, and thus advise people against doing:
Better safe than sorry
We’ll leap straight into it:
- General Surgery: avoid rushing into musculoskeletal or spinal surgery unless absolutely necessary; conservative treatments like physical therapy are often effective.
- Interventional Gastroenterology: avoid long-term, around-the-clock use of anti-inflammatory pain medications (e.g. Ibuprofen and friends) to prevent stomach ulcers.
- Podiatry: never place feet on the car dashboard due to the risk of severe injuries from airbag deployment.
- Rheumatology: avoid daily use of high heels to prevent joint and foot deformities, bunions, and pain.
- Otorhinolaryngology: never smoke, as it can lead to severe consequences like laryngectomy and other life-altering conditions.
- Pediatrics: avoid dangerous activities for children, such as swimming alone, eating choking hazards, biking or skiing without a helmet, or consuming raw meat/fish/dairy. Also, be cautious with firearms in homes.
- Orthopedic Surgery: avoid riding motorcycles and handling fireworks due to high risks of accidents.
- Emergency Medicine: never drink and drive or ride ATVs. Always use eye protection during activities like woodworking.
- Ophthalmology: always wear safety glasses during activities like grinding metal or woodworking. Sunglasses are essential to prevent UV damage even on cloudy days.
- Urology: avoid shaving pubic hair if diabetic or immunocompromised to prevent severe infections like Fournier’s gangrene.
- Gastroenterology: do not use gut health supplements as they lack proven efficacy and are often a waste of money*
- Plastic Surgery: avoid contour threads (barbed sutures for facial rejuvenation) and butt implants due to risks like infection, complications, and poor outcomes.
- Psychiatry: never take recreational drugs from unknown sources to avoid accidental overdoses, especially from substances laced with fentanyl. Carry Narcan for emergencies.
- Dermatology: use sunscreen daily to prevent skin cancer, aging, pigmentation issues, and texture problems caused by UV exposure.
- Cardiology: avoid the carnivore diet as it increases heart disease risks due to its negligible fiber content and high saturated fat intake.
*We had an article about this a while back; part of the problem is that taking probiotics without prebiotics can mean your new bacteria just die in about 20 minutes, which is their approximate lifespan in which to multiply or else die out. Similar problems arise if taking them with sugar that feeds their competitors instead. See: Stop Sabotaging Your Gut!
For more on each of these, in the words of the respective doctors, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Dates vs Prunes – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing dates to prunes, we picked the prunes.
Why?
First let’s note: we’re listing the second fruit here as “prunes” rather than “plums”, since prunes are dehydrated plums, and it makes more sense to compare the dried fruit to dates which are invariably dried too. Otherwise, the water weight of plums would unfairly throw out the nutrient proportions per 100g (indeed, upon looking up numbers, dates would overwhelmingly beat plums easily in the category of pretty much every nutrient).
So let’s look at the fairer comparison:
In terms of macros, dates have a little more protein, carbohydrate, and fiber. This is because while both are dried, prunes are usually sold with more water remaining than dates; indeed, per 100g prunes still have 30g water weight to dates’ 20g water weight. This makes everything close, but we are going to call this category a nominal win for dates. Mind you, hydration is still good, but please do not rely on dried fruit for your hydration!
When it comes to vitamins, dates have more of vitamins B5 and B9, while prunes have more of vitamins A, B2, B3, B6, C, E, K, and choline. A clear win for prunes here.
In the category of minerals, it’s a similar story: dates have more iron, magnesium, and selenium, while prunes have more calcium, copper, manganese, phosphorus, potassium, and zinc. Another win for prunes.
In short, enjoy either or both, but prunes win on overall nutritional density!
Want to learn more?
You might like to read:
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
Take care!
Share This Post
-

28-Day FAST Start Day-by-Day – by Gin Stephens
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have previously reviewed Gin Stephens’ other book, “Fast. Feast. Repeat.”, so what’s so special about this one that it deserves reviewing too?
This one is all about troubleshooting the pitfalls that many people find when taking up intermittent fasting.
To be clear: the goal here is not a “28 days and yay you did it, put that behind you now”, but rather “28 days and you are now intermittently fasting easily each day and can keep it up without difficulty”. As for the difficulties that may arise early in the 28 days…
Not just issues of willpower, but also the accidental breaks. For example, some artificial sweeteners, while zero-calorie, trigger an insulin response, which breaks the fast on the metabolic level (avoiding that is the whole point of IF). Lots of little tips like that peppered through the book help the reader to stop accidentally self-sabotaging their progress.
The author does talk about psychological issues too, and also how it will feel different at first while the liver is adapting, than later when it has already depleted its glycogen reserves and the body must burn body fat instead. Information like that makes it easier to understand that some initial problems (hunger, getting “hangry”, feeling twitchy, or feeling light-headed) will last only a few weeks and then disappear.
So, understanding things like that makes a big difference too.
The style of the book is simple and clear pop-science, with lots of charts and bullet points and callout-boxes and the like; it makes for very easy reading, and very quick learning of all the salient points, of which there are many.
Bottom line: if you’ve tried intermittent fasting but struggled to make it stick, this book can help you get to where you want to be.
Share This Post
-

Ice Baths: To Dip Or Not To Dip?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

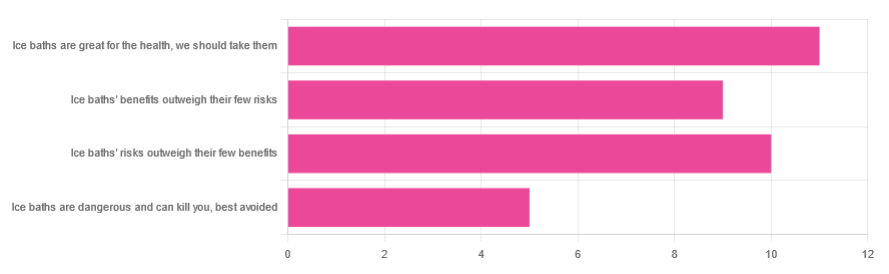
We asked you for your (health-related) view of ice baths, and got the above-depicted, below-described, set of responses:
- About 31% said “ice baths are great for the health; we should take them”
- About 29% said “ice baths’ risks outweigh their few benefits”
- About 26% said “ice baths’ benefits outweigh their few risks”
- About 14% said “ice baths are dangerous and can kill you; best avoided”
So what does the science say?
Freezing water is very dangerous: True or False?
True! Water close to freezing point is indeed very dangerous, and can most certainly kill you.
Fun fact, though: many such people are still saveable with timely medical intervention, in part because the same hypothermia that is killing them also slows down the process* of death
Source (and science) for both parts of that:
Cold water immersion: sudden death and prolonged survival
*and biologically speaking, death is a process, not an event, by the way. But we don’t have room for that today!
(unless you die in some sudden violent way, such as a powerful explosion that destroys your brain instantly; then it’s an event)
Ice baths are thus also very dangerous: True or False?
False! Assuming that they are undertaken responsibly and you have no chronic diseases that make it more dangerous for you.
What does “undertaken responsibly” mean?
Firstly, the temperature should not be near freezing. It should be 10–15℃, which for Americans is 50–59℉.
You can get a bath thermometer to check this, by the way. Here’s an example product on Amazon.
Secondly, your ice bath should last no more than 10–15 minutes. This is not a place to go to sleep.
What chronic diseases would make it dangerous?
Do check with your doctor if you have any doubts, as no list we make can be exhaustive and we don’t know your personal medical history, but the main culprits are:
- Cardiovascular disease
- Hypertension
- Diabetes (any type)
The first two are for heart attack risk; the latter is because diabetes can affect core temperature regulation.
Ice baths are good for the heart: True or False?
True or False depending on how they’re done, and your health before starting.
For most people, undertaking ice baths responsibly, repeated ice bath use causes the cardiovascular system to adapt to better maintain homeostasis when subjected to thermal shock (i.e. sudden rapid changes in temperature).
For example: Respiratory and cardiovascular responses to cold stress following repeated cold water immersion
And because that was a small study, here’s a big research review with a lot of data; just scroll to where it has the heading“Specific thermoregulative adaptations to regular exposure to cold air and/or cold water exposure“ for many examples and much discussion:
Health effects of voluntary exposure to cold water: a continuing subject of debate
Ice baths are good against inflammation: True or False?
True! Here’s one example:
Uric acid and glutathione levels (important markers of chronic inflammation) are also significantly affected:
Uric acid and glutathione levels during short-term whole body cold exposure
Want to know more?
That’s all we have room for today, but check out our previous “Expert Insights” main feature looking at Wim Hof’s work in cryotherapy:
A Cold Shower A Day Keeps The Doctor Away?
Enjoy!
Share This Post


-

How to Change – by Katy Milkman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes it seems that we know everything we should be doing… We have systems and goals and principles, we know about the importance of habits, and we do our best to live them. Yet, somehow, life has other plans for us and things don’t quite come together they way they did in our genius masterplan.
So, what happened? And more importantly, what are we supposed to do about this? Katy Milkman has answers, right from the start.
Sometimes, it can be as simple as when we try to implement a change. It’s not that there’s a “wrong time” for a good change, so much that there are times that are much more likely to succeed than others… and those times can be identified and used.
Sometimes we’re falling prey to vices—which she explains how to overcome—such as:
- Impulsivity
- Procrastination
- Forgetfulness
- Laziness
We also learn some counterintuitive truths about what can boost or sabotage our confidence along the way!
Milkman writes in a compelling, almost narrative style, that makes for very easy reading. The key ideas, built up to by little (ostensibly true) stories and then revealed, become both clear and memorable. Most importantly, applicable.
Bottom line: this is a great troubleshooting guide for when you know how everything should be working, but somehow, it just doesn’t—and you’d like to fix that.
Click here to check out “How To Change” on Amazon, and get those changes rolling!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Signs That Are Present When Someone Is Dying
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You’ve probably been there a few times, although given the emotional nature of the thing, it’s likely that you weren’t taking notes. Hospice workers, on the other hand, do take notes, so here are some things you might want to know, and if anything makes the next time even a little easier, that’ll be good:
Last stages
Here are the discussed signs of the “active dying” phase:
- Increasing unconsciousness:
- The person will be mostly unresponsive most of the time.
- Eyes may be open or partially open but not making eye contact.
- Mouth will likely remain open due to muscle relaxation.
- Cessation of food and water intake
- The person will likely not eat or drink for several days.
- This is a natural process and does not cause suffering per se (e.g. thirst, hunger).
- Dryness of mouth, however, can be treated with a little moistening, for comfort.
- Changes in breathing
- Breathing patterns will change and may be irregular.
- This is a natural metabolic response, and is not a sign of distress.
- Terminal secretions (“death rattle”) may occur:
- A gurgling sound caused by saliva buildup due to loss of swallowing reflex.
- Not painful or distressing for the person.
- Can be managed by repositioning or using medication to dry secretions.
- Skin color changes / mottling:
- First appears on fingers and toes (purple or gray discoloration).
- May spread to knees, nose, or other extremities.
- Temperature fluctuations:
- The body loses its ability to regulate temperature.
- Person may feel hot but be cold (or vice versa).
- Fevers are common—cooling measures and/or Tylenol can help.
A person in discomfort may appear restless, have a furrowed brow, or show physical agitation. If on the other hand they appear peaceful and unresponsive, they are almost certainly not in distress. At such times, it’s best to focus on just keeping them clean and comfortable.
For more on all of these, see:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Managing Mortality: When Planning Is a Matter of Life and Death
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Increasing unconsciousness:
-
Starfruit vs Soursop – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing starfruit to soursop, we picked the soursop.
Why?
First, by starfruit, we also mean carambola, which is a different name for the same fruit, and by soursop we also mean graviola/guyabano/guanábana, which are different namers for the same fruit. Now, as for their health qualities:
In terms of macros, the soursop has more carbs and fiber, the ratio of which also give it the lower glycemic index. So, a win for soursop here.
When it comes to vitamins, starfruit has more of vitamins A, B5, C, and E, while soursop has more of vitamins B1, B2, B3, B6, B7, B9, and K. Another win for soursop.
In the category of minerals, starfruit has slightly more copper, manganese, and zinc, while soursop has much more calcium, iron, magnesium, phosphorus, and potassium. One more win for soursop!
Adding up the sections makes for a clear and overwhelming win for soursop, but let’s address to quick safety considerations while we’re here:
- Soursop extract has been claimed to be an effective cancer treatment. It isn’t. There is no evidence for this at all; just one unscrupulous company that spread the claims.
- Soursop contains annonacin, a neurotoxin. That sounds scary, but much like with apple seeds and cyanide, the quantities you’d have to consume to suffer ill effects are absurd. Remember how capsaicin (as found in hot peppers) is also a neurotoxin, too and has many health benefits. Humans have a long and happy tradition of enjoying things that are toxic at high doses, but in small doses are neutral or even beneficial. Pretty much all things we can consume (including oxygen, and water) are toxic at sufficient doses.
In short, both of these fruits are fine and good, neither will treat cancer, but both will help to keep you in good health. As for nutritional density, the soursop wins in every category.
Want to learn more?
You might like to read:
Top 8 Fruits That Prevent & Kill Cancer ← soursop has no special cancer treatment properties, but actual evidence shows these fruits are beneficial (being good as a preventative, and also definitely a worthy adjunct to—but not a replacement for—mainstream anticancer therapies if you have cancer).
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: