The Science of Self-Learning – by Peter Hollins
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Teaching oneself new things is often the most difficult kind of bootstrapping, especially when one is unsure of such critical things as:
- Where to begin? How, for that matter, do we find where to begin?
- What can/should a learning journey look like?
- What challenges should we expect, and how will we overcome them?
Hollins answers all of these questions and more. The greatest value of this book is perhaps in its clear presentation of concrete step-by-step instructions. Hollins gives illustrated examples too, but most importantly, he gives models that can be applied to any given type of learning.
The book also covers the most difficult problems most people face when trying to learn something by themselves, including:
- Keeping oneself on-task (maintaining discipline)
- Measuring progress (self-testing beyond memorization)
- Keeping a fair pace of progress (avoiding plateaus)
- How to know when one’s knowledge is sufficient or not (avoiding Dunning-Kruger Club)
All in all, if you’re looking to learn a new subject or skill, this could be a first step that saves you a lot of time later!
Get your copy of the Science of Self-Learning on Amazon today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Many Heartbeats Do You Have Left?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our life is, of course, not literally measured in heartbeats—or at least not usefully so (since there are many other factors). However, there is a strong inverse correlation between resting heartrate and healthy longevity! That is to say, the slower your heart beats, the longer you’ll live.
Caveat: this is a generalization, and applies to a low resting heart rate that is the result of good cardiac health. It does not mean you should, for example, take up the use of heroin for its heartbeat-slowing effects. That will not help you to live longer!
Where’s the science?
Lest our opening claim there sound like popular wisdom rather than something backed by good science, let’s tend to that before moving on to the main thing today. There are, in fact, many papers to back up this claim, but here’s a good one:
It’s a 30-year longitudinal cohort study with 5,070 participants and baseline (as with most longitudinal studies, not everyone survived for the entire duration), and why we particularly like this one is not just its strong statistical significance, but also, because rather than simply looking at average resting heartrate and longevity, it also looked at changes in average resting heartrate and longevity, which makes the case for the link being causal much stronger.
❝In this study, we examined the association between resting heart rate and lifespan using linear regression in the Paris Prospective Study I, the Whitehall I Study, and the Framingham Heart Study. We used Cox proportional hazards regression to relate changes in heart rate over years to mortality risk.
We observed a statistically significant association between increases in resting heart rate over a 5-year period and risk of mortality in the Paris Prospective Study I (HR mortality per 10 bpm increase over time: 1.20; 95% CI: 1.13 to 1.27) and over an 8-year period in the Framingham Heart Study (HR: 1.13; 95% CI: 1.07 to 1.19 for men and HR: 1.09; 95% CI: 1.04 to 1.15 for women), after adjusting for classical risk factors and resting heart rate.
Our study shows that men and women who increase their resting heart rate over time increase their risk of mortality.❞
You may be wondering: why did we say 30 years, if the abstract is citing 5 years and 8 years?
And the answer is: it has to do with the statistical modeling used; the participants were followed for up to 30 years, but the statistical analysis allows us to look at what difference a change in resting heartrate makes over the course of 5 or 8 years, which is more illustrative for most people than “this is what will probably happen when you are [your age plus another 30 years]” statements. Indeed, the very fact that we can see a statistically significant change in mortality risk in just 5 years, makes it clear how big that risk is.
And how big is the risk? Translating the hazard ratios into percentages, we’re looking at, per 10 bpm increase over time, a 20% increase in mortality risk in the 5-year period per the Paris Prospective Study, or a 10%-ish increase in mortality risk in the 8-year period per the Framingham Heart Study. As for why the 5-year period has a bigger risk than the 8-year period, it’s likely down to a slightly different methodology and what other risk factors were controlled for.
One final note: about that “…and resting heart rate”, lest that seem confusing, we will mention that this too was controlled for because the primary input variable being looked at was the change in resting heartrate, not the resting heartrate itself.
In summary: if your resting heartrate increases, so does your mortality risk, at a rate of 10–20% over 5–8 years, for every 10 bpm increase (in other words: that stacks!).
So, what’s this about how many heartbeats we have left?
Based on the above, we can infer that since a change in heartrate is associated with an inverse change in longevity, the total number of heartbeats may often not change much, it’s just that the shorter-lived people squoze more heartbeats into less time.
With that in mind, a “common sense” logic tells us that we should conserve our heartbeats in order to live longer. This is somewhat consistent with the ideas behind some meditative practices.
However, while in a sense that’s not wrong (and such meditative practices can indeed help extend healthy lifespan), this presents an apparent paradox:
Should we avoid exercise, because it accelerates our heartrate while we are exercising?
And the robust answer is no, as some recent science by Dr. Kristel Janssens et al. shows clearly.
How it works: while exercise indeed speeds up the heartrate while exercising, it also lowers one’s resting heartrate by a sufficient amount (per metabolic equivalent of task minutes), that when all’s said and done, the hearts of those who regularly exercise beat fewer times per day than those who do not regularly exercise—and the difference isn’t small:
❝Athletes had an average heart rate of 68 beats per minute (bpm), while non-athletes had 76bpm. That translates to a total of 97,920 beats per day for athletes and 109,440 beats per day for non-athletes – around 10 percent less.❞
Note: that’s average heartrate, not average resting heartrate*. So it’s still counting all the heartbeats that happened during exercise, too. The athletes’ hearts were simply beating slowly enough the rest of the time to more than compensate.
*This is also worth bearing in mind because 68 bpm would be an astonishingly high resting heartrate for a very fit person.
Read the paper in full, here: Balancing Exercise Benefits Against Heartbeat Consumption in Elite Cyclists
Want to do more for your heart?
Check out:
How To Improve Your Heart Rate Variability
…for another thing to bear in mind (and helpfully, it’ll usually lower your resting heartrate, too).
Enjoy!
Share This Post
-

Wasting Your Vitamins?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Are you flushing away your vitamins?
Most likely…but you don’t have to.
We all know what a wasteful expense supplements can sometimes be, but you can optimise your intake to get more bang for your buck!
Top Tips for Getting Your Money’s Worth:
- Liquids are better than tablets—the body can’t absorb nutrients from tablets anywhere as easily as it can from liquids, with some saying as low as a 50% absorption rate for tablets, so if your supplement can come in drinkable form, take it that way!
- Capsules are better than tablets—capsules, depending on the kind, contain either a powder (true capsules) or a liquid (softgels). Once the capsule/softgel is broken down in the stomach, it releases its contents, which will now be absorbed as though you took it as a drink.
- Stay hydrated—on that note, your body can only make use of nutrients that it can easily transport, and if you’re dehydrated, the process is sluggish! Having a big glass of water with your supplements will go a long way to helping your body get them where they’re needed.
- Take with black pepper—studies disagree on exactly how much black pepper improves absorption of nutrients. Some say it improves it by 50%, others say as much as 7x better. The truth is probably that it varies from one nutrient to the next, but what is (almost) universally accepted is that black pepper helps you absorb many nutrients you take orally.
- Take with a meal—bonus if you seasoned it with black pepper! But also: many nutrients are best absorbed alongside food, and many are specifically fat-soluble (so you want to take a little fat around the same time for maximum absorption)
- Consider split doses—a lot of nutrients are best absorbed when spread out a bit. Why? Your body can often only absorb so much at once, and what it couldn’t absorb can, depending on the nutrient, pass right through you. So better to space out the doses—breakfast and dinner make for great times to take them.
- Consider cycling—no, not the two-wheeled kind, though feel free to do that too! What cycling means when it comes to supplements is to understand that your body can build a tolerance to some supplements, so you’ll get gradually less effect for the same dose. Combat this by scheduling a break—five days on, two days off is a common schedule—allowing your body to optimise itself in the process!
- Check Medications—and, as is always safe, make sure you check whether any medications you take can interrupt your supplement absorption!
Share This Post
-
Chicken Skin: Do You Have Keratosis Pilaris, Or Something Else?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Andrea Suarez explains how to stop this from happening:
Keratin, Kerat-out
Dry skin cannot shed keratin properly, so it accumulates around hair follicles, creating small, rough, sandpaper-like bumps. Depending on various conditions (and your baseline skin pigmentation), can be anywhere from pale white (dead skin) through to dark brown. If it’s unusually pink or red, that’s probably inflammation.
Notably, the bumps are dry and rough rather than painful, and any itch is usually mild unless your skin is extremely dry, and there may be no itch at all.
There are some lookalikes, which are either related conditions (like folliculitis) or unrelated (like acne). Here’s what to watch out for.
- Folliculitis: inflamed hair follicles caused by bacteria, yeast, or irritation, often red, tender, itchy, or pus-filled, and commonly triggered by shaving, sweating, or friction.
- Follicular erythema from hair removal: redness around hair follicles that appears shortly after shaving, waxing, or plucking and usually settles within a few days, unlike keratosis pilaris which lingers.
- Eczema (atopic dermatitis): can resemble keratosis pilaris but is typically very itchy, may ooze or weep, and involves inflamed skin beyond the hair follicle itself.
- Pityrosporum folliculitis (fungal acne): uniform, itchy red bumps caused by yeast overgrowth, often worsens with heat, humidity, and sweating, and commonly affects the forehead, chest, and upper back.
- Milia: tiny white keratin-filled cysts that are not linked to a hair follicle, are not inflamed, and do not respond to moisturizers or exfoliating acids.
- Acne: larger, deeper, often painful or pus-filled lesions that may scar or leave dark marks, which is not typical of keratosis pilaris.
So, if it is keratosis pilaris, how to deal with it?
The main thing is consistent use of moisturizers containing keratolytics such as urea, lactic acid, glycolic acid, and/or salicylic acid to smooth skin and improve hydration.
Improvement usually takes 4–6 weeks of regular use, and ongoing maintenance is needed because the condition tends to recur if left unchecked. You can also help reduce its recurrence if you keep showers short and not too hot, pat your skin dry instead of rubbing, moisturize immediately after bathing, and use a humidifier in otherwise dry environments.
When to see a dermatologist: if the bumps are painful, itchy, spreading, or unresponsive to over-the-counter treatments, or if it is unclear what condition is present, then it’s time to let a professional take a look.
For more on all of this plus some visual illustrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Beyond Castor: Vegetable Oils That Regenerate Your Skin
Take care!
Share This Post



Related Posts
-

Is Chiropractic All It’s Cracked Up To Be?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is Chiropractic All It’s Cracked Up To Be?

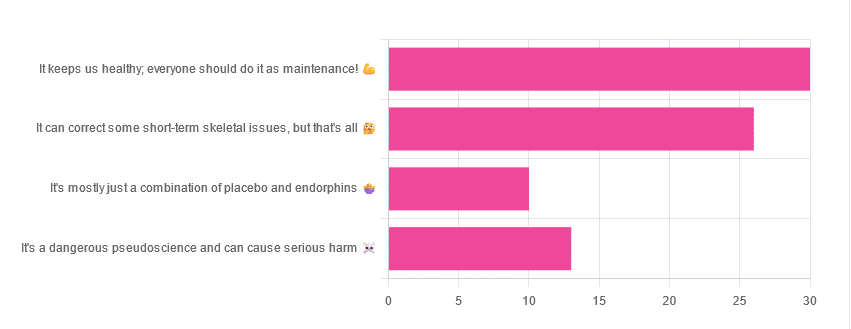
Yesterday, we asked you for your opinions on chiropractic medicine, and got the above-depicted, below-described set of results:
- 38% of respondents said it keeps us healthy, and everyone should do it as maintenance
- 33% of respondents said it can correct some short-term skeletal issues, but that’s all
- 16% of respondents said that it’s a dangerous pseudoscience and can cause serious harm
- 13% of respondents said that it’s mostly just a combination of placebo and endorphins
Respondents also shared personal horror stories of harm done, personal success stories of things cured, and personal “it didn’t seem to do anything for me” stories.
What does the science say?
It’s a dangerous pseudoscience and can cause harm: True or False?
Mixed and True, respectively.
That is to say, chiropractic in its simplest form that makes the fewest claims, is not a pseudoscience. If somebody physically moves your bones around, your bones will be physically moved. If your bones were indeed misaligned, and the chiropractor is knowledgeable and competent, this will be for the better.
However, like any form of medicine, it can also cause harm; in chiropractic’s case, because it more often than not involves manipulation of the spine, this can be very serious:
❝Twenty six fatalities were published in the medical literature and many more might have remained unpublished.
The reported pathology was usually vascular accidents involving the dissection of a vertebral artery.
Conclusion: Numerous deaths have occurred after chiropractic manipulations. The risks of this treatment by far outweigh its benefit.❞
Source: Deaths after chiropractic: a review of published cases
From this, we might note two things:
- The abstract doesn’t note the initial sample size; we would rather have seen this information expressed as a percentage. Unfortunately, the full paper is not accessible, and nor are many of the papers it cites.
- Having a vertebral artery fatally dissected is nevertheless not an inviting prospect, and is certainly a very reasonable cause for concern.
It’s mostly just a combination of placebo and endorphins: True or False?
True or False, depending on what you went in for:
- If you went in for a regular maintenance clunk-and-click, then yes, you will get your clunk-and-click and feel better for it because you had a ritualized* experience and endorphins were released.
- If you went in for something that was actually wrong with your skeletal alignment, to get it corrected, and this correction was within your chiropractor’s competence, then yes, you will feel better because a genuine fault was corrected.
*this is not implying any mysticism, necessarily, though that can certainly also be a component for many, and indeed, chiropractic was originally founded as a new religious movement. Outside of the context of spirituality, however, it means simply that placebo effect is strongest when there is a ritual associated with it. In this case it means going to the place, sitting in a pleasant waiting room, being called in, removing your shoes and perhaps some other clothes, getting the full attention of a confident and assured person for a while, this sort of thing.
With regard to its use to combat specifically spinal pain (i.e., perhaps the most obvious thing to treat by chiropractic spinal manipulation), evidence is slightly in favor, but remains unclear:
❝Due to the low quality of evidence, the efficacy of chiropractic spinal manipulation compared with a placebo or no treatment remains uncertain. ❞
Source: Clinical Effectiveness and Efficacy of Chiropractic Spinal Manipulation for Spine Pain
It can correct some short-term skeletal issues, but that’s all: True or False?
Probably True.
Why “probably”? The effectiveness of chiropractic treatment for things other than short-term skeletal issues has barely been studied. From this, we may wish to keep an open mind, while also noting that it can hardly claim to be evidence-based—and it’s had hundreds of years to accumulate evidence. In all likelihood, publication bias has meant that studies that were conducted and found inconclusive or negative results were simply not published—but that’s just a hypothesis on our part.
In the case of using chiropractic to treat migraines, a very-related-but-not-skeletal issue, researchers found:
❝Pre-specified feasibility criteria were not met, but deficits were remediable. Preliminary data support a definitive trial of MCC+ for migraine.❞
Translating this: “it didn’t score as well as we hoped, but we can do better. We got some positive results, and would like to do another, bigger, better trial; please fund it”
Source: Multimodal chiropractic care for migraine: A pilot randomized controlled trial
Meanwhile, chiropractors’ claims for very unrelated things have been harshly criticized by the scientific community, for example:
Misinformation, chiropractic, and the COVID-19 pandemic
About that “short-term” aspect, one of our subscribers put it quite succinctly:
❝Often a skeletal correction is required for initial alignment but the surrounding fascia and muscles also need to be treated to mobilize the joint and release deep tissue damage surrounding the area. In combination with other therapies chiropractic support is beneficial.❞
This is, by the way, very consistent with what was said in the very clinically-dense book we reviewed yesterday, which has a chapter on the short-term benefits and limitations of chiropractic.
A truism that holds for many musculoskeletal healthcare matters, holds true here too:
❝In a battle between muscle and bone, muscle will always win❞
In other words…
Chiropractic can definitely help put misaligned bones back where they should be. However, once they’re there, if the cause of their misalignment is not treated, they will just re-misalign themselves shortly after you walking out of your session.
This is great for chiropractors, if it keeps you coming back for endless appointments, but it does little for your body beyond give you a brief respite.
So, by all means go to a chiropractor if you feel so inclined (and you do not fear accidental arterial dissection etc), but please also consider going to a physiotherapist, and potentially other medical professions depending on what seems to be wrong, to see about addressing the underlying cause.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Blueberries vs Raspberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing blueberries to raspberries, we picked the raspberries.
Why?
In terms of macros, blueberries have slightly more carbs, while raspberries have 2.5x the fiber and also slightly more protein, not that the protein figure is why people are eating raspberries, as a general rule of thumb. In any case, we say raspberries win this round based on the higher fiber content and resultantly much lower glycemic index.
In the category of vitamins, blueberries have more of vitamins A and K, while raspberries have more of vitamins B3, B4, B9, C, E, and choline, making for a convincing win for raspberries here.
When it comes to minerals, blueberries are not higher in any mineral, while raspberries are higher in calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. A very clear win for raspberries in this round.
Looking at polyphenols, both are good but blueberries have more polyphenols in total, so they score a win in this round.
Adding up the sections makes for a compelling overall win for raspberries, but blueberries have their merits too, so by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
21 Most Beneficial Polyphenols & What Foods Have Them
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
A new diagnosis of ‘profound autism’ is on the cards. Here’s what could change
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to autism, few questions spark as much debate as how best to support autistic people with the greatest needs.
This prompted The Lancet medical journal to commission a group of international experts to propose a new category of “profound autism”.
This category describes autistic people who have little or no language (spoken, written, signed or via a communication device), who have an IQ of less than 50, and who require 24-hour supervision and support.
It would only apply to children aged eight and over, when their cognitive and communication abilities are considered more stable.
In our new study, we considered how the category could impact autism assessments. We found 24% of autistic children met, or were at risk of meeting, the criteria for profound autism.
Why the debate?
The category is intended to help governments and service providers plan and deliver supports, so autistic people with the highest needs aren’t overlooked. It also aims to re-balance their under-representation in mainstream autism research.
This new category may be helpful for advocating for a greater level of support, research and evidence for this group.
But some have raised concerns that autistic people who don’t fit into this category could be perceived as less in need and excluded from services and funding supports.
Others argue the category doesn’t sufficiently emphasise autistic people’s strengths and capabilities, and places too much emphasis on the challenges that are experienced.
What did we do?
We conducted the first Australian study to examine how the “profound autism” category might apply to children attending publicly funded diagnostic services for developmental conditions.
Drawing on the Australian Child Neurodevelopment Registry, we examined data from 513 autistic children assessed between 2019 and 2024. We asked:
- how many children met the criteria for profound autism?
- were there behavioural features that set this group apart?
Because we focused on children at the time of diagnosis, most (91%) were aged under eight years. We described these children as being “at risk of profound autism”.
What did we find?
Around 24% of autistic children in our study met, or were at risk of meeting, the criteria for profound autism. This is similar to the proportion of children internationally.
Almost half (49.6%) showed behaviours that were a safety risk, such as attempting to run away from carers, compared with one-third (31.2%) of other autistic children.
These challenges weren’t limited to children who met criteria for profound autism. Around one in five autistic children (22.5%) engaged in self-injury, and more than one-third (38.2%) showed aggression toward others.
So, while the category identified many children with very high needs, other children who didn’t meet these criteria also had significant needs.
Importantly, we found the definition of “profound autism” doesn’t always line up with the official diagnostic levels which determine the level of support and NDIS funding children receive.
In our study, 8% of children at risk of profound autism were classified as level 2, rather than level 3 (the highest level of support). Meanwhile, 17% of children classified as level 3 did not meet criteria for profound autism.
Our concern
We looked at children when they first received an autism diagnosis. Children were aged 18 months to 16 years, with more than 90% under the age of eight years.
This aligns with our earlier research, showing the average age of diagnosis in public settings is 6.6 years.
From a practical perspective, our biggest concern about the profound autism category is the age threshold of eight years.
Because most children are already assessed before age eight, introducing this category into assessment services would mean many families would need repeat assessments, placing additional strain on already stretched developmental services.
Second, modifications will be needed if this criteria is going to be used to inform funding decisions as it didn’t map perfectly onto level 3 support criteria.
On balance, however, our results suggest the profound autism category may provide a clear, measurable way to describe the needs of autistic people with the highest support requirements.
Every autistic child has individual strengths and needs. The term “profound autism” would need to be promoted with inclusive and supportive language, so as to not replace or diminish individual needs, but to help clinicians tailor supports and obtain additional resources when needed.
Including the category in future clinical guidelines, such as the national guideline for the assessment and diagnosis of autism, could help ensure governments, disability services and clinicians plan and deliver supports.
What can you do in the meantime?
If you’re concerned your child requires substantial support, here are some practical steps you can take to ensure their needs are recognised and addressed:
Explain your concerns
Not all clinicians have experience working with children with high support needs. Be as clear as possible about behaviours that affect your child’s safety or daily life, including self-injury, aggression or attempts to run away. These details, while difficult to share, help give a clearer picture of your child’s support needs.
It can also be a challenge to find and access clinicians with appropriate expertise. Another potential benefit of having a defined category is that it can better help families navigate care.
Ask about support for the whole family
Our studies show that many caregivers want more support for themselves but don’t always ask. Talk with clinicians about supports for yourself as well, including respite, or family support groups.
Reach out
Coming together with other carers and families can reduce your own isolation and normalise many of the unique challenges you face. Connecting with like-minded people can provide a supportive, empathetic and empowering community.
Plan for safety
For children with high support needs, prioritise safety planning with your child’s care team. This can include strategies to reduce risks, as well as planning how best to support your child’s interactions with health, education and disability services over time.
Kelsie Boulton, Senior Research Fellow in Child Neurodevelopment, Brain and Mind Centre, University of Sydney; Marie Antoinette Hodge, Clinical Lecturer, University of Sydney, and Rebecca Sutherland, Lecturer & Speech Pathologist, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: